
Positive Behaviour Support To Manage Challenging Behaviour Of Children On Autism Spectrum


Abstract
Children with autism spectrum disorder (ASD) are at increased risk of having challenging behavior that can affect success to education and community inclusion. This review examined the use of positive behavior support (PBS) to address the challenging behavior of children with ASD. Using vigorous selection criteria, a total of nine PBS intervention studies was identified; all of them employed a single subject design with seven of them rated high quality using Evaluative Method for Determining Evidence-Based Practices in Autism. Results indicated that PBS had positive impact on the replacement of challenging behavior with desirable performance for children with ASD. The maintenance effect and generalization in natural and structured settings were also found positive. Findings suggested that PBS is a promising intervention approach for promoting appropriate behavior of children with ASD. Nevertheless, large scale of PBS clinical trials for children with ASD are needed for more vigorous assessment of its efficacy.
Keywords:
Introduction
There has been a sizable increase in the number of children with autism spectrum disorder (ASD) throughout the world (Honda et al., 2009; Wong & Hui, 2007). Impairment in social communication and social interaction, and restricted, repetitive patterns of behaviour, interests, or activity characterize ASD (American Psychiatric Association, 2013). These deficits can adversely affect the quality of family life and access to education and community inclusion. In fact, children with ASD have more inappropriate behaviour when compared to their typically developing peers (Kozlowski, Matson, & Rieske, 2012; Mahan & Matson, 2011). Among children who display challenging behaviour, the majority of them have the diagnosis of ASD (Conroy et al. 2005).
Children with ASD are at risk of having complex and severe challenging behaviours such as aggression, noncompliance, property destruction, antisocial, bullying behaviour and self-injury (Matson, Hess, & Mahan, 2013; Matson & Nebel-Schwalm, 2007). These challenging behaviours lead to further difficulties in keeping up positive relationship with their teachers and become a burden on teacher stress (Lecavalier, Leone, & Wiltz, 2006; Robertson, Chamberlain, & Kasari, 2003). The behaviours could also create a hindrance to learning and teaching and children with ASD are often identified as “troublesome” (Barnard, Prior, & Potter, 2000; Robertson et al., 2003). It has been reported that unaddressed challenging behaviours lend to higher rate on severity over time and that childhood behavioural issues are associated with more extreme behavioural problems in adolescent and adult life, such as substance abuse, unemployment, mental health problems and criminal conduct (Conroy, Dunlap, Clarke, & Alter, 2005; Reid & Patterson, 1991). There is an alarming upsurge demand for evidence-based practice to address challenging behaviour of children with ASD.
Problem Statement
Behavioural interventions that have adopted the proactive and positive approach to prevent or reduce challenging behaviour are highlighted in the literature (Dunlap & Fox, 2011). Among the behavioural interventions for challenging behaviour, Positive Behaviour Support (PBS) has attracted much attention in recent years. PBS has adopted the strength-based perspective and its key features include functional behaviour assessment, principles of applied behaviour analysis and positive reinforcement (Horner et al., 1990). It can be applied in family, school and community settings (Algozzine, Daunic, & Smith, 2010; Neitzel, 2010; Riffel, 2011). PBS has been applied to address the inappropriate behaviour of children and young people. PBS requires comprehension understanding of why children take part in challenging behaviours and intervention for preventing the incidence by replacing them with desirable performance (Fox & Duda, 2011). The holistic approach of PBS can be implemented through different stakeholders, such as parents, teachers, peers and organizations (Buschbacher & Fox, 2003; Carr & Sidener, 2002; Dunlap et al., 2006). PBS has also gained much intention as a valuable and socially valid approach for children with ASD (Cheremshynski, Lucyshyn, & Olson, 2013; Dunlap et al., 2006; McIntosh et al., 2014; Neitzel, 2010).
Research Questions
Therefore, how efficient is PBS as an intervention approach for promoting appropriate behavior of children with ASD?
Purpose of the Study
There have been two review studies on problem behavioural interventions specifically for children with ASD (Horner, Carr, Strain, Todd, & Reed, 2002; Odom et al., 2003), but PBS was not included in these reviews. Another review study, the efficacy of PBS was examined for children with problem behaviour in general (Conroy et al. 2005). To our knowledge, none of the three reviews focused specifically on PBS for children with ASD. The research gap indicates that literature on the intervention effectiveness attributable solely to PBS in reducing challenging behaviour of children with ASD is relatively meagre. Through this context, we initiated the present systematic review (SR) to examine the efficacy of PBS in managing the challenging behaviour of children with ASD. In this synthesis, we concentrated on only intervention studies using solely PBS for this group of children.
Research Methods
Literature search strategies and inclusion criteria
Two researchers conducted the literature search independently. PBS intervention studies were selected from the following 14 electronic databases: Academic search Premier, Education Research Complete, Wiley Online Library, Cochrane Library, ProQuest Database, ProQuest Social Science, Scopus, ProQuest Dissertation, Medline, ERIC, CINAHL, PsycINFO, Web of Science and Google Scholar. The databases were searched from their inception to April 2015. Keywords used in the search included the words “positive behaviour support” or “PBS” AND “autism” or “autism spectrum disorder” or “ASD” in article title, abstract or keywords. All articles identified were downloaded into EndNote X8 for finding the full text and also checking for duplication.
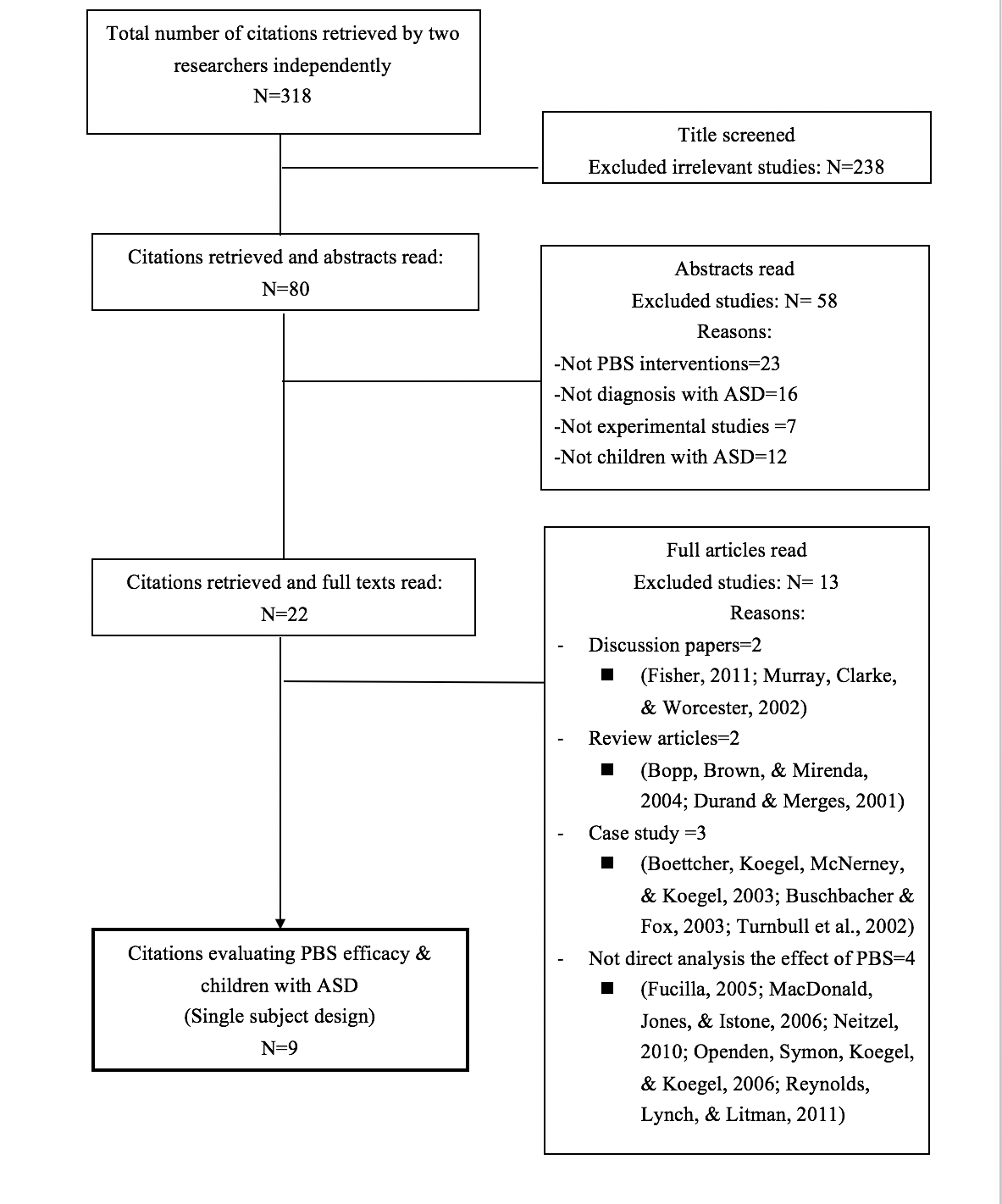
To be included in the present study, studies on PBS were required to meet all the specific criteria: (i) used experimental design: randomized clinical trial (RCT), controlled clinical trial (CCT), pre-post studies or single subject design; (ii) published in English peer-reviewed journals reporting an empirical intervention (editorials, correspondences, abstracts only without the full papers, discussion papers, review summaries and book chapters were excluded); (iii) the study used PBS as the only intervention method; and (iv) participants were children under the age of 18 with confirmed ASD diagnosis. Selection criterion (i) was screened on the basis of only the methods section of the searched studies. All other criteria were screened after examining the full report of each searched study. The overall percentage of agreement between the two researchers on the exclusion/inclusion status of the studies screened was 95%. Disagreements were settled by consensus and/or discussions with a senior author who had published several SRs before. The present study was in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Moher, Liberati, Tetzlaff, & Altman, 2009)
Data extraction and assessment of study quality
Two researchers rated independently the methodological rigor of each selected study using the guidelines prescribed in the Evaluative Method for Determining Evidence-Based Practices in Autism (Reichow, Volkmar, & Cicchetti, 2008). These guidelines can assess the study quality of group and single subject research with reliable and valid assessment results (Knight & Sartini, 2015; Watkins et al., 2015). For the assessment of study quality, there are primary and secondary quality indicators. Using these guidelines, each PBS intervention study was assessed as having strong, adequate or weak methodological quality.
The assessment of PBS as evidence-based practice for children with ASD
The guidelines developed by Reichow and colleagues (2008) were used to assess PBS whether it reached the requirement as the category of “established or promising evidence-based practice” for children with ASD. There are criteria for group and single subject research. The two researchers completed the assessment exercise independently and the agreement was nearly 100%.
Findings
A total of nine intervention studies from peer-reviewed journals were extracted from 318 identified in the initial search. All of the included studies used single subject design and neither clinical trials nor pre-post studies were found in the search process. The nine included studies were published between 1999 and 2013. Among these studies, three were from the United States, three from Canada, two from South Korea and one from Ireland. Figure
Quality of included studies
Table
The nine studies together had a total of 17 participants (14 males; 3 females). The age of the participants ranged from 2.4 to 17 years old. Six studies had the single diagnosis of ASD (Binnendyk & Lucyshyn, 2009; Cheremshynski et al., 2013; Dunlap & Fox, 1999; Lee et al., 2007; Marshall & Mirenda, 2002). Two studies had dual diagnoses: cerebral palsy and intellectual disabilities (Blair et al., 2011; Lucyshyn et al., 2007). One study had triple diagnoses included intellectual disabilities, bipolar depression and attention deficit disorder (McClean & Grey, 2012). The intervention time to outcome assessment ranged from four to 152 weeks. Seven studies were conducted in the home setting, one study in two settings: home and school and one study in the community setting.
The nine included studies used four different types of single subject research designs. Four studies used the basic design (Becker-Cottrill, McFarland, & Anderson, 2003; Binnendyk & Lucyshyn, 2009; Dunlap & Fox, 1999; Marshall & Mirenda, 2002); two studies used the withdrawal/reversal design (Cheremshynski et al., 2013; Lee et al., 2007); two employed the multiple baseline design (Blair et al., 2011; Lucyshyn et al., 2007); and one study adopted the multiple-element baseline design (Blair et al., 2011; McClean & Grey, 2012). Table
Intervention outcomes
Study characteristics are found in Table
Calculation of effect size: Percent non-Overlapping Data (PND)
The method of PND described by Parker, Vannest, and Davis (2011) was used to calculate the effect sizes for the nine included PBS intervention studies. This method was specifically designed for single subject research design. For challenging behaviour, PND was calculated by summing the quantity of treatment data points that fell below the lowest baseline data point, divided by the total number of treatment data points, and the scores were multiplied by 100. For appropriate behaviour, the treatment data points above the highest baseline data point were divided by the total number of treatment data points, and the scores were also multiplied by 100. PND score could range from 0-100%. PND of 50% and above has been considered large for treatment effect. PND was not calculated for maintenance or generalization data.
There were 28 behavioural outcomes included for the calculation of PND score. The mean PND score across the nine included PBS intervention studies was 93.7% (SD=11.8%, range=45.5-100%). For the challenging behaviour, the mean PND score was 92.5% (SD= 13.7%). For the appropriate behaviour, the PND mean score was 96.2% (SD=5.8%). PND score could not be calculated for two studies due to limited data for visual analysis and data point information in baseline and intervention phases. PND scores are presented in Table
Maintenance, Generalization, Treatment fidelity, and Social validity
Seven of the included studies reported positive maintenance effect (Becker-Cottrill et al., 2003; Binnendyk & Lucyshyn, 2009; Blair et al., 2011; Cheremshynski et al., 2013; Lee et al., 2007; Lucyshyn et al., 2007; Marshall & Mirenda, 2002; McClean & Grey, 2012). One study reported the negative maintenance effect (Lee et al., 2007). The maintenance period ranged from three weeks to 10 years.
Four studies reported positive generalization: two studies illustrated the generalization to new skills (Binnendyk & Lucyshyn, 2009; Marshall & Mirenda, 2002), and another two studies showed that the generalization was across settings (Blair et al., 2011; Lucyshyn et al., 2007). One study reported that the generalization was failed (Lee et al., 2007).
Four studies reported the treatment fidelity with reliability greater than 0.80 (Blair et al., 2011; Cheremshynski et al., 2013; McClean & Grey, 2012). One study reported moderate level of treatment fidelity at 0.68 (Binnendyk & Lucyshyn, 2009). Four studies provided social validity with high statistics outcomes and the range was from 0.92 to 0.96. (Binnendyk & Lucyshyn, 2009; Blair et al., 2011; Cheremshynski et al., 2013; Lucyshyn et al., 2007).
PBS as evidence-based practice for children with ASD
For the assessment of evidence-based practice, this SR found that PBS was reported effective in two strong and five adequate quality studies, and implemented by seven different research teams across four countries (Binnendyk & Lucyshyn, 2009; Blair et al., 2011; Dunlap & Fox, 1999; Lee et al., 2007; Lucyshyn et al., 2007; McClean & Grey, 2012). These findings indicated PBS had the potential to be considered promising evidence-based practice for children with ASD.
Discussion
The present study aimed to critically appraise existing intervention studies to examine the efficacy of PBS for children with ASD following strictly the standardized criteria of SR. With rigorous process, we identified nine PBS intervention studies; all of them used single subject design. In the search process, no PBS group research for children with ASD was found. Seven of the included studies were ranked as having good methodological quality using the guidelines developed by Reichow and colleagues (2008). The high PND scores of these seven studies indicated that PBS was found effective in reducing challenging behaviour and at the same time could enhance desirable performance for children with ASD. The positive outcomes reported in all included studies suggested that PBS was a promising evidence-based practice for managing challenging behaviour for children with ASD.
An interesting finding in this review was that PBS targeted both challenging behaviour and desirable performance in social interaction and community inclusion. Given that one of the core characteristics of ASD behaviour is the lack of appropriate social and communication skills, this imperative finding would further assist this group of children for engagement in school and community settings. Another finding is the PBS was implemented in home environment. This outcome suggested PBS can be used in unstructured settings and that parents as the main caregivers are the key intervention agent. Another encouraging finding is the positive maintenance effect of the appropriate behaviour and skills. The ability to sustain appropriate behaviour is an important indicator of the overall effectiveness of an intervention (Watkins et al., 2015). Not all of the included studies reported generalization, social validity and treatment fidelity. This kind of practice is also reported in the review by Conroy et al. (2005) of PBS for children with challenging behaviour in general. The absence of these measures has impact on the research validity and future studies are encouraged to take this into considerations.
It is forecasted that the use of single subject design is a developing trend in studying ASD. Single subject research is an approach used to establish evidence-based clinical practice (Barlow, Hersen, Barlow, Nock, & Hersen, 2009; Feuer, Towne, & Shavelson, 2002; Kazdin, 2011). It is argued that systematic and detailed analysis of single subject research method in fact has been growing in the acceptance among the research disciplines (Kazdin, 2011; Lekwa & Ysseldyke, 2010). In addition, single subject design is particularly useful for circumstances in which parents, teachers, therapists or other intervention resources are scarce (Horner et al., 2005; Kratochwill & Levin, 2010; Levin, 2007).
The trend of providing integrated intervention programs for children with ASD is witnessed to match with the learning needs and behavioural characteristics of this group of children (McConkey, Truesdale-Kennedy, Chang, Jarrah, & Shukri, 2008). Although large scale and long-term RCTs examining solely PBS for further efficacy evidence is very desirable, the feasibility might not be high due to ethical considerations and the trend of integrated intervention programs for persons with ASD. Boyd et al. (2014) suggested that the shift in thinking around the models designed for children with ASD is worth considering. They argued perhaps it is not the unique features of the models that most contribute to child growth; instead it is the common features of the models that affect the performance of children with ASD (i.e., the common factory theory).
This SR has limitations. The comparatively high PND score of PBS intervention outcome might be due to the small number of included studies and the stringent inclusion criteria. The authors are aware of the development of the new model of Prevent-Teach-Reinforce (PTR) which adopted the idea of PBS (Dunlap, Iovannone, Wilson, Kincaid, & Strain, 2009). PTR is in the early phase of its development and two studies about the use of PTR on children with ASD were identified in the search process (Dunlap et al., 2006; Strain, Wilson, Wilson, & Dunlap, 2011). Since the concepts of PTR are still evolving, it was decided that these two studies were not included in this SR but would be an area for future research. Another limitation was our decision to restrict selection to intervention studies written in English; that was partly due to the lack of resource for translation, and that the authors believe restricting to intervention studies is a desirable strategy for investigating efficacy.
Conclusion
In conclusion, the present SR of nine single subject design studies indicated that PBS was beneficial to children with ASD, particularly in replacing challenging behaviour with desirable performance. However, this review should not be seen as providing a definitive statement about PBS efficacy; rather, it is intended to describe what appears to be known to date as well as to explore the knowledge gaps. Care must be taken to generalize the results of the present study as the evidence is still not strong enough for us to make any definite conclusive remarks. Large scale and well-designed RCTs with long-term follow-up durations, if achievable, are required to further confirm the effect of PBS on children with ASD.
Acknowledgments
The project was partially funded by the General Research Fund, The Research Grants Council, Hong Kong (Reference Number: 843112).
References
- Algozzine, B., Daunic, A. P., & Smith, S. W. (2010). Preventing problem behaviors: Schoolwide programs and classroom practices: Corwin Press.
- American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5®): American Psychiatric Pub.
- Barlow, D. H. N., Hersen, M., Barlow, M. D., Nock, M., & Hersen, M. (2009). Single case experimental designs: Strategies for studying behavior for change.
- Barnard, J., Prior, A., & Potter, D. (2000). Inclusion and autism: Is it working. London: National Autistic Society.
- *Becker-Cottrill, B., McFarland, J., & Anderson, V. (2003). A model of positive behavioral support for individuals with autism and their families: The family focus process. Focus on Autism and Other Developmental Disabilities, 18(2), 113-123.
- *Binnendyk, L., & Lucyshyn, J. M. (2009). A Family-Centered Positive Behavior Support Approach to the Amelioration of Food Refusal Behavior An Empirical Case Study. Journal of Positive Behavior Interventions, 11(1), 47-62.
- *Blair, K.-S. C., Lee, I.-S., Cho, S.-J., & Dunlap, G. (2011). Positive Behavior Support Through Family-School Collaboration for Young Children With Autism. Topics in Early Childhood Special Education, 31(1), 22.
- Boettcher, M., Koegel, R. L., McNerney, E. K., & Koegel, L. K. (2003). A family-centered prevention approach to PBS in a time of crisis. Journal of Positive Behavior Interventions, 5(1), 55-59.
- Bopp, K. D., Brown, K. E., & Mirenda, P. (2004). Forum on intervention strategies for severe disabilities. Speech-language pathologists' roles in the delivery of positive behavior support for individuals with developmental disabilities. American Journal of Speech-Language Pathology, 13(1), 5-19.
- Boyd, B., Hume, K., McBee, M., Alessandri, M., Gutierrez, A., Johnson, L., . . . Odom, S. (2014). Comparative Efficacy of LEAP, TEACCH and Non-Model-Specific Special Education Programs for Preschoolers with Autism Spectrum Disorders. Journal of Autism and Developmental Disorders, 44(2), 366-380.
- Buschbacher, P. W., & Fox, L. (2003). Understanding and intervening with the challenging behavior of young children with autism spectrum disorder. Language Speech and Hearing Services in Schools, 34(3), 217-227.
- Carr, J. E., & Sidener, T. M. (2002). On the relation between applied behavior analysis and positive behavioral support. The Behavior Analyst, 25(2), 245-253.
- Chandler, L. K., & Dahlquist, C. M. (2014). Functional assessment: Strategies to prevent and remediate challenging behavior in school settings: Pearson Higher Ed.
- *Cheremshynski, C. M. A., Lucyshyn, J. M. P., & Olson, D. L. P. (2013). Implementation of a Culturally Appropriate Positive Behavior Support Plan With a Japanese Mother of a Child With Autism: An Experimental and Qualitative Analysis. Journal of Positive Behavior Interventions, 15(4), 242.
- Conroy, M. A., Dunlap, G., Clarke, S., & Alter, P. J. (2005). A Descriptive Analysis of Positive Behavioral Intervention Research With Young Children With Challenging Behavior. Topics in Early Childhood Special Education, 25(3), 157-166.
- *Dunlap, G., & Fox, L. (1999). A Demonstration of Behavioral Support for Young Children with Autism. Journal of Positive Behavior Interventions, 1(2), 77-87.
- Dunlap, G., & Fox, L. (2011). Function-Based Interventions for Children With Challenging Behavior. Journal of Early Intervention, 33(4), 333-343.
- Dunlap, G., Iovannone, R., Wilson, K. J., Kincaid, D. K., & Strain, P. (2009). Prevent-Teach-Reinforce: A standardized model of school-based behavioral intervention. Journal of Positive Behavior Interventions.
- Dunlap, G., Strain, P. S., Fox, L., Carta, J. J., Conroy, M., Smith, B. J., . . . Sowell, C. (2006). Prevention and Intervention With Young Children's Challenging Behavior: Perspectives Regarding Current Knowledge. Behavioral Disorders, 32(1), 29-45.
- Durand, V. M., & Merges, E. (2001). Functional Communication Training: A Contemporary Behavior Analytic Intervention for Problem Behaviors. Focus on Autism and Other Developmental Disabilities, 16(2), 110-119,136.
- Feuer, M. J., Towne, L., & Shavelson, R. J. (2002). Scientific Culture and Educational Research. Educational Researcher, 31(8), 4-14.
- Fisher, J. (2011). Positive Behavior Support for Students with Autism. Principal, 91(2), 32-35.
- Fox, L., & Duda, M. A. (2011). Positive behavior support. Technical Assistance Center on Social Emotional Intervention for Young Children. Retrieved on November, 16, 2011.
- Fucilla, R. (2005). Post-Crisis Intervention for Individuals with Autism Spectrum Disorder. Reclaiming Children and Youth, 14(1), 44-51.
- Honda, H., Shimizu, Y., Nitto, Y., Imai, M., Ozawa, T., Iwasa, M., . . . Hira, T. (2009). Extraction and Refinement Strategy for detection of autism in 18-month-olds: a guarantee of higher sensitivity and specificity in the process of mass screening. Journal of Child Psychology and Psychiatry, 50(8), 972-981.
- Horner, R. H., Carr, E., Strain, P., Todd, A., & Reed, H. (2002). Problem Behavior Interventions for Young Children with Autism: A Research Synthesis. Journal of Autism and Developmental Disorders, 32(5), 423-446.
- Horner, R. H., Carr, E. G., Halle, J., McGee, G., Odom, S., & Wolery, M. (2005). The Use of Single-Subject Research to Identify Evidence-Based Practice in Special Education. Exceptional Children, 71(2), 165-179.
- Horner, R. H., Dunlap, G., Koegel, R. L., Carr, E. G., Sailor, W., Anderson, J., . . . O'Neill, R. E. (1990). Toward a Technology of “Nonaversive” Behavioral Support. Research and Practice for Persons with Severe Disabilities, 15(3), 125-132.
- Kazdin, A. E. (2011). Single-case research designs: Methods for clinical and applied settings: Oxford University Press.
- Knight, V., & Sartini, E. (2015). A Comprehensive Literature Review of Comprehension Strategies in Core Content Areas for Students with Autism Spectrum Disorder. Journal of Autism and Developmental Disorders, 45(5), 1213-1229.
- Kozlowski, A. M., Matson, J. L., & Rieske, R. D. (2012). Gender effects on challenging behaviors in children with autism spectrum disorders. Research in Autism Spectrum Disorders, 6(2), 958-964.
- Kratochwill, T. R., & Levin, J. R. (2010). Enhancing the scientific credibility of single-case intervention research: Randomization to the rescue. Psychological Methods, 15(2), 124.
- Lecavalier, L., Leone, S., & Wiltz, J. (2006). The impact of behaviour problems on caregiver stress in young people with autism spectrum disorders. Journal of Intellectual Disability Research, 50(3), 172-183.
- *Lee, S.-H., Poston, D., & Poston, A. J. (2007). Lessons learned through implementing a positive behavior support intervention at home: A case study on self-management with a student with autism and his mother. Education and Training in Developmental Disabilities, 42(4), 418-427.
- Lekwa, A., & Ysseldyke, J. (2010). Dissertation Research in School Psychology: Changes in Topics and Methodology Over the Past 25 Years. Journal of Applied School Psychology, 26(1), 17-37.
- Levin, J. (2007). Randomization tests: Statistical tools for assessing the effects of educational interventions when resources are scarce. Real data analysis, Information Age, Greenwich, CT, 115-123.
- *Lucyshyn, J. M., Albin, R. W., Horner, R. H., Mann, J. C., Mann, J. A., & Wadsworth, G. (2007). Family implementation of positive behavior support for a child with autism: Longitudinal, single-case, experimental, and descriptive replication and extension. Journal of Positive Behavior Interventions, 9(3), 131-150.
- MacDonald, C., Jones, K., & Istone, M. (2006). Positive Behavioral Support. Teaching Elementary Physical Education, 17(6), 20-24
- Mahan, S., & Matson, J. L. (2011). Convergent and discriminant validity of the Autism Spectrum Disorder-Problem Behavior for Children (ASD-PBC) against the Behavioral Assessment System for Children, Second Edition (BASC-2). Research in Autism Spectrum Disorders, 5(1), 222-229.
- *Marshall, J. K., & Mirenda, P. (2002). Parent-professional collaboration for positive behavior support in the home. Focus on Autism and Other Developmental Disabilities, 17(4), 216-228.
- Matson, Hess, J. A., & Mahan, S. (2013). Moderating effects of challenging behaviors and communication deficits on social skills in children diagnosed with an autism spectrum disorder. Research in Autism Spectrum Disorders, 7(1), 23-28.
- Matson, & Nebel-Schwalm. (2007). Comorbid psychopathology with autism spectrum disorder in children: An overview. Research in Developmental Disabilities, 28(4), 341-352.
- *McClean, B., & Grey, I. (2012). An evaluation of an intervention sequence outline in positive behaviour support for people with autism and severe escape-motivated challenging behaviour. Journal of Intellectual & Developmental Disability, 37(3), 209-220.
- McConkey, R., Truesdale-Kennedy, M., Chang, M.-Y., Jarrah, S., & Shukri, R. (2008). The impact on mothers of bringing up a child with intellectual disabilities: A cross-cultural study. International Journal of Nursing Studies, 45(1), 65-74.
- McIntosh, K., Predy, L. K., Upreti, G., Hume, A. E., Turri, M. G., & Mathews, S. (2014). Perceptions of Contextual Features Related to Implementation and Sustainability of School-Wide Positive Behavior Support. Journal of Positive Behavior Interventions, 16(1), 31-43.
- Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA StatementThe PRISMA Statement. Annals of Internal Medicine, 151(4), 264-269.
- Murray, M., Clarke, S., & Worcester, J. (2002). A teacher's perspective of using PBS in a classroom for a girl with multiple disabilities. Journal of Positive Behavior Interventions, 4(3), 189-192.
- Neitzel, J. (2010). Positive behavior supports for children and youth with autism spectrum disorders. Preventing School Failure: Alternative Education for Children and Youth, 54(4), 247-255.
- Odom, S. L., Brown, W. H., Frey, T., Karasu, N., Lee Smith-Canter, L., & Strain, P. S. (2003). Evidence-Based Practices for Young Children With Autism: Contributions for Single-Subject Design Research. Focus on Autism and Other Developmental Disabilities, 18(3), 166-175.
- Openden, D., Symon, J. B., Koegel, L. K., & Koegel, R. L. (2006). Developing a student respite provider system for children with autism. Journal of Positive Behavior Interventions, 8(2), 119-123.
- Parker, R. I., Vannest, K. J., & Davis, J. L. (2011). Effect Size in Single-Case Research: A Review of Nine Nonoverlap Techniques. Behavior Modification, 35(4), 303-322.
- Reichow, B., Volkmar, F., & Cicchetti, D. (2008). Development of the Evaluative Method for Evaluating and Determining Evidence-Based Practices in Autism. Journal of Autism and Developmental Disorders, 38(7), 1311-1319.
- Reid, J., & Patterson, G. (1991). Early prevention and intervention with conduct problems: A social interactional model for the integration of research and practice. Interventions for achievement and behavior problems, 715-740.
- Reynolds, S., Lynch, S. L., & Litman, S. (2011). Training care teams of children with autism spectrum disorders in positive behaviour support: an innovative approach. Healthcare quarterly (Toronto, Ont.), 14(3), 95-99.
- Riffel, L. A. (2011). Positive Behavior Support at the Tertiary Level: Red Zone Strategies: Corwin Press.
- Robertson, K., Chamberlain, B., & Kasari, C. (2003). General Education Teachers' Relationships with Included Students with Autism. Journal of Autism and Developmental Disorders, 33(2), 123-130.
- Strain, P. S., Wilson, K., Wilson, K., & Dunlap, G. (2011). Prevent-Teach-Reinforce: Addressing Problem Behaviors of Students with Autism in General Education Classrooms. Behavioral Disorders, 36(3), 160-171.
- Turnbull, A., Edmonson, H., Griggs, P., Wickham, D., Sailor, W., Freeman, R., Warren, J. (2002). A blueprint for schoolwide positive behavior support: Implementation of three components. Exceptional Children, 68(3), 377-402.
- Watkins, L., O’Reilly, M., Kuhn, M., Gevarter, C., Lancioni, G., Sigafoos, J., & Lang, R. (2015). A Review of Peer-Mediated Social Interaction Interventions for Students with Autism in Inclusive Settings. Journal of Autism and Developmental Disorders, 45(4), 1070-1083.
- Wong, V. C. N., & Hui, S. L. H. (2007). Epidemiological Study of Autism Spectrum Disorder in China. Journal of Child Neurology. doi:10.1177/0883073807308702. (Studies included in the review were marked with an asterisk (*).)
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
21 September 2018
Article Doi
eBook ISBN
978-1-80296-045-7
Publisher
Future Academy
Volume
46
Print ISBN (optional)
Edition Number
1st Edition
Pages
1-887
Subjects
Education, educational equipment, educational technology, computer-aided learning (CAL), Study skills, learning skills, ICT
Cite this article as:
Wong, W., Li, P., Ji, M., & Lo, S. K. (2018). Positive Behaviour Support To Manage Challenging Behaviour Of Children On Autism Spectrum. In S. K. Lo (Ed.), Education Environment for the Information Age, vol 46. European Proceedings of Social and Behavioural Sciences (pp. 875-887). Future Academy. https://doi.org/10.15405/epsbs.2018.09.02.103