
Familial relationships perceived by parents and adolescent depression: Psychosocial functioning moderating effect


Abstract
Depression is considered a health problem associated with significant impairment in psychosocial functioning. The quality of interpersonal relationships between parent and adolescents can be an important protective/vulnerability factor to depression. This study aims to understand if the psychosocial functioning of the adolescent is a moderator variable between the quality of interpersonal relationships perceived by the parents and depressive symptoms of the adolescents. Further, we analyse if gender of adolescents influence the quality of these relationships, and if psychosocial functioning and quality of interpersonal relationships is associated with depression. The sample is constituted by 132 adolescents and their parents, participants integrated in a research project about prevention of adolescent depression (PTDC/MHC-PCL/4824/2012). Self-report questionnaires were used to assess depressive symptoms (
Keywords: Psychosocial functioningQRI-PPdepressionmoderationadolescence
1.Introduction
It is during adolescence that intense developmental changes occur, that mark the transition be-tween childhood and adulthood. Thus, this step is very important to build the identity of the individual and for the search of his desired independence (Cicchetti & Toth, 2009; Eccles, Lord, & Roeser, 1996).
The majority of adolescents pass through this phase without encountering significant psycholog-ical, social or health care problems. However, adolescence is marked by an increase of the incidence and prevalence of psychiatric disorders, one of them being depression (Compas, 2004). Depression rates increase remarkably in this age group, being that one in five adolescents probably will develop depression (Birmaher et al., 1996). In addition, the sooner the manifestation of depression, the more likely is the occurrence of depressive episodes throughout life (Essau, Lewinsohn, Seeley, & Sasagawa, 2010). Studies also refer to the existence of gender differences in the development and manifestation of depressive symptoms in adolescents (Essau et al., 2010; Galambos, Leadbeater, & Barker, 2004), girls presenting a prevalence of about double compared to boys (Saluja et al., 2004).
Depression, characterized by a change in mood that is persistent and severe enough to be consid-ered a disturbance (Kolvin, 2005), is associated with symptoms such as depressed mood and clear decrease of interest in activities, significant weight gain or loss, insomnia or hypersomnia, agitation or psychomotor retardation, fatigue or loss of energy, feelings of devaluation or guilt, diminished ability to think or concentrate and recurrent thoughts about death (American Psychiatric Association, 2013). In adolescence, depression may be manifested through an irritable and unstable mood (Bahls & Bahls, 2002).
Depression presents a lasting nature, and is associated with significant functional losses and with a reduction of long-term quality of life (Bahls, 2002; Fergusson & Woodward, 2002; Greer, Kurian, & Trivedi, 2010). According to the World Health Organization (2008), it could even become the main cause of incapacity, in the most developed countries.
In this way, it becomes urgent to identify which risk factors may contribute to its development. Some of them may be: past depression (e.g. Lewinsohn, Hoberman, & Rosenbaum, 1988); presence of another disturbance (e.g., Sanford et al., 1995); belonging to the female gender (e.g. Block, Gjerde, & Block, 1991); having family members with the same pathology (e.g. Lieb, Isensee, Höfler, Pfister, & Wittchen, 2002); history of early losses (e.g. Slavich, Monroe, & Gotlib, 2011); having troubles at school (e.g. Fröjd et al., 2008); having experienced stressful life events and having low social support from friends and family (e.g., Monroe, Bromet, Connell, & Steiner, 1986); and, having poor psychosocial functioning (e.g. Lewinsohn et al., 1998).
Psychosocial functioning (PF) includes a variety of constructs that relate to achieving develop-mental tasks that are expected in a given age and context, approaching the concept of competence (Masten & Coatsworth, 1995).
Most researches study the relationship between development of depression and deterioration of PF (e.g., Greer et al., 2010; Fried & Nesse, 2014; Harrington & Vostanis, 1995; Lewinsohn, Rohde, Seeley, Klein, & Gotlib, 2003; Mehta, Mittal, & Swami, 2014; Puig-Antich et al., 1993). However, studies like the one from Lewinsohn et al. (1994, 1998) stressed out the importance of assessing psychosocial characteristics of adolescents in risk of developing depression, in order to prevent it. In his longitudinal study on a sample of 1709 teenagers, Lewinsohn et al. (1998) found that adolescents who revealed a functional impairment in regard to health, have a higher risk – about 19.4%- of becoming depressed (showing a risk of approximately more 12% in relation to young people who did not express dysfunctionality). In the same, the study of McCabe, Ricciardelli and Banfield (2011) revealed that children who were classified as being at risk of developing depression, showed problems in their PF.
Impairment can occur globally or in multiple domains, such as at work/school, in recreational ac-tivities/hobbies, in satisfaction with life and in interpersonal relationships (Costa, 2011; Fergusson & Woodward, 2002; Goldstein et al., 2009; Greer et al., 2010; Lewinsohn et al., 1994; Mehta et al., 2014). Some studies examine separately the relationship of these dimensions with depression.
According to the studies of Fröjd et al. (2008) and Chen and Li (2000), in a sample of 2329 and 540 students respectively, a poor school performance is significantly associated with depression.
Gledhill and Garralda (2010), highlighted the role of positive life events in reducing depression, mentioning the importance of scheduling pleasant or rewarding activities, in order to promote these events. Satisfaction with life also seems to be associated with subjective well-being, relating negatively with depression (Koivumaa-Honkanen et al., 2001). In a sample of 330 adults, the longitudinal study of Rissanen et al. (2011) revealed that dissatisfaction was strongly related to the development of depression.
Sheeber, Hops, Alpert, Davis and Andrews (1997) reported that depressive symptoms in adoles-cents are related with the quality of their family relationships. This is in accordance with what is defended by other authors, who report that less social support and more conflict in family relationships, particularly with the father and the mother, seems to be associated with depressive symptomatology (e.g. Cheng et al., 2014; Cole & McPherson, 1993; Lewinsohn et al., 1994; Lee, Wong, Chow, & McBride-Chang, 2006; McFarlane, Bellissimo, Norman, & Lange, 1994; Smojver-žić1 & Bezinović, 2011). Longitudinal studies have shown that when family relationships are positive, adolescents are less likely to develop depression (Cheng et al., 2014; Lewinsohn et al., 1994; Reinherz et al., 1993). Studies in Portugal, found that the support/depth dimension was negatively correlated with depressive symptomatology in adolescents. However, this happened to girls and boys regarding the relationship with the father and just for girls in regard to the relationship with the mother. In female adolescents, conflict in the relationships with the father is also associated with higher levels of depressive symptomatology (Matos, Pinheiro & Marques, 2013; Pinheiro, Matos & Marques, 2013).
According to the study of Greca and Harrison (2005), which featured a sample of 421 adoles-cents, the relationships with friends and lovers can also be factors of vulnerability/protection for the development of depressive symptomatology.
Some investigations also make reference to the role that the gender may have in the relation of these variables with depression. With regard to school performance, Pomerantz, Altermatt, and Saxon (2002), on a sample of 932 students, mentioned that although the girls had better performances at school, they assessed their performance in a more negative way and worried more about it, being more likely to develop depression. Similarly, Cole, Martin, Peeke, Seroczynski and Fier (1999), noted that that when children are underestimated as to their academic competence (especially girls), they report higher levels of depressive symptomatology.
Gender differences were also reported with regard to satisfaction with life, Goldbeck, Schmitz, Besier, Herschbach and Henrich (2007) revealed that boys consistently showed higher values in this variable.
Given the family relationships, including some dimensions that characterized the quality of rela-tions between parents and children, Matos et al. (2013) and Pinheiro et al. (2013) found differences between genders in support/depth dimension of the Quality of Relationships Inventory. Girls perceived more support/depth in their relationship with the mother, while boys perceived more conflict. Adolescents of the male gender also revealed higher levels of conflict with the father than girls. However, studies of Rueger, Malecki, and Demaray (2008, 2010), on a sample of students revealed that there were no gender differences in the perception of parental support.
When it comes to relations with friends and boyfriends, Neves and Pinheiro (2009) found that girls showed more positive relationships with their best friends, while boys reported more positive relationships with romantic partners. Rueger, Malecki, and Demaray (2008, 2010) e Bokhorst, Sumter and Westenberg (2009), found that girls perceived more support on the part of friends than boys.
Taking into account, in particular, the influence of variables associated with PF and with the quality of interpersonal relationships seem to have on well-being and psychological suffering, this research aims to: i) study existing associations between quality of parents/children relationship, as perceived by the parents, and depressive symptoms of their children; ii) analyze the relationship between psychosocial functioning and symptomatology in adolescents; iii) test the moderator effect of psychosocial functioning in the relationship between the quality of parents/children relationships and depressive symptomatology.
2. Methodology
2.1 Participants
The sample consisted of 132 students and their parents, who participated voluntarily and anony-mously in the research project "Prevention of depression in Portuguese adolescents: efficacy study of an intervention with adolescents and parents", in which the present study is inserted. In the sample there is a predominance of the female gender, both in young people and in parents. Thus, from the 132 students, 90 are female (68.2%) and 42 are males (31.8%). In respect to parents, 113 are female (85.6%) and 19 are male (14.4%). Student ages ranged between 13 and 17 years (
2.2 Instruments
2.3 Procedures
National entities that regulate scientific research authorized this study to students and their par-ents who have agreed to participate in the investigation. Confidentiality was assured and subjects were asked to sign an informed consent. The parents' assessment protocol was sent home to be filled, while students were evaluated and interviewed at school.
2.4 Analytical Strategy
Data insertion and statistical analyses were conducted using the Statistical Package for Social
Sciences (SPSS), version 22.0 for Windows.
In order to study differences between genders, Student t-tests for independent samples were used. Results were considered statistically significant when p ≤ .05 (Marôco, 2010). To study the relationship between the variables, Pearson correlation coefficients (r) were used –the convention of Pestana and Gageiro (2008) was adopted, which states that a value of r < .20 indicates a very low correlation; .20 < r < .39 low; .40 < r < .69 moderate; .70 < r < 0.89 high; e > .90 very high. Finally, the possible moderator effect of PF in the relationship between the quality of parents/children relationship and depressive symptomatology was studied. A variable is said to be a moderator if it affects the direction and/or strength of the relation between two variables (Baron &
Kenny, 1986; Holmbeck, 1997). To this end, we proceeded to the standardization of the independent and moderator variables, which allows a reduction of multicollinearity issues (Marôco, 2010). Then the interaction term variables were created, by multiplying the predictor variable (factors of QRI-PP) and the moderator variable (total score or PF areas). Finally, hierarchical multiple linear regressions were conducted, where adolescents’ depressive symptomatology was established as a criterion variable. In these regressions, firstly one of the factors of the predictor variable was entered, followed by one factor or the total of the moderator and, finally, the interaction between the two. If the interaction term is significant (p ≤ .05) we can say that there is a interaction effect.
3. Results
3.1 Preliminary analysis of the data
Assumption of normality of variables was analyzed using the Kolmogorov-Smirnov test, which suggests that the sample does not have a normal distribution ((K-S, p ≤ .001). However, when analyzing the bias relative to the mean through the values of asymmetry (sk < |3|) and flattening (ku < |10|), it was possible to conclude that there was no serious bias that compromises normal distribution of the data (Kline, 2011). The adequacy of the data to the realization of the hierarchical multiple regression was confirmed.
3.2. Gender Differences in depressive symptomatology, in the quality of parents/children relations (perceived by parents) and in psychosocial functioning
To find out whether there were gender differences,
3.3. Study of the relations between the quality of parents/children relationships (perceived by the parents), psychosocial functioning and depressive symptomatology Pearson correlations were performed to study the relationship between the variables. Therefore, it might be noted that the CDI correlated with all areas evaluated from PF (with the exception of school performance dimension) and with satisfaction. QRI-PP dimensions did not significantly correlate with depressive symptomatology (cf. Table
3.4 Analysis of the moderation effects
Hierarchical multiple regression analyses were made to ascertain if PF has a moderating effect in the relationship between quality of parents/children relationships (perceived by parents) and depressive symptomatology.
There were no significant interaction effects of PF and of satisfaction with the conflict dimen-sion. School performance and satisfaction were also the only significant moderators of the relationship between the factor support/depth in parents/children relationships and depressive symptomatology. Following, we present the analysis in which significant moderating effects were obtained.
3.4.1 The moderator effect of school performance in the relationship between support/depth (perceived by parents) and depressive symptomatology As previously stated, there was a moderator effect of school performance (β = -.203, p < .05). Examining each of the variables, it was found that both support/depth (β = -.140, p > .05) as well as school performance (β = .126, p > .05) were not predictors of depressive symptoms (see Table
The variables support/depth and school performance showed no significant models in step 1 and
2. However, in the third step (interaction term) a significant model was produced that showed an increase in the percentage of variance explained in relation to depressive symptoms. The interaction (support/depth * school performance) proved to be a significant predictor, explaining 7.3% of the variance in depressive symptomatology (see Table
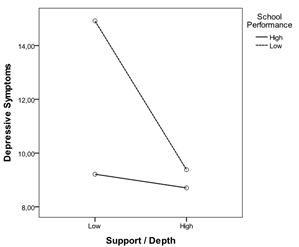
between support/depth and depressive symptoms
In Figure
Since significant differences for gender were found in some of the variables under considera-tion, it was decided to investigate the effects of moderation separately for males and for females.
In this way, it was observed that school performance has a significant moderator effect only for the female gender (
Variables support/depth and school performance showed a significant model in the second step, and in the interaction term. The interaction (support/depth * school performance) proved to be a significant predictor, explaining 15.8% of the variance in adolescents’ depression (cf. Table
school performance and interaction term for females (
A graphic of the moderation effect for the female gender is presented in Figure
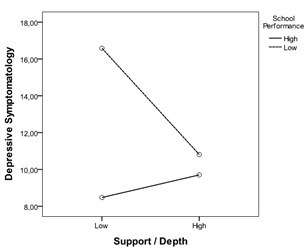
with support/depth and depressive symptomatology in females
3.4.2. Moderator effect of satisfaction with life in the relationship between support/depth (perceived by parents) and depressive symptomatology
Variable satisfaction also produced a significant moderating effect (
It was observed that satisfaction generated a significant model in the second step, along with the
interaction term in step 3. This interaction (support/depth * satisfaction) proved to be a significant predictor, explaining 29.6% of the variance in depressive symptomatology (cf. Table
In the graphical representation, the two levels for the support/depth remained and three levels were created for satisfaction (low: up to
Regarding the interpretation of the interaction effect, it turns out that when support/depth is low-er, lower levels of satisfaction are associated with more depressive symptoms, compared with average or high levels of satisfaction. When the support/depth is high, depressive symptomatology tends not to differentiate when there is a low or medium level of satisfaction, with a greater decline when satisfaction level is higher - This effect is observed through the approximation of the two lines of middle and low level of satisfaction, and through the line of high satisfaction that lies further down (cf. Figure
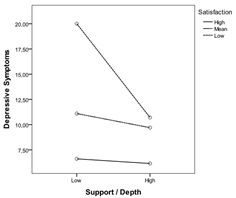
support/depth and depressive symptoms
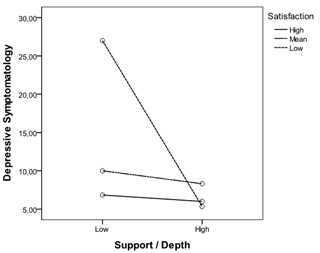
When we studied the moderator effect separately for male and female, it was observed that there
was a moderator effect meaningful only to the male gender (β = -.373, p < .05). When variables were analyzed separately, only the support/depth factor seemed to predict depressive symptomatology (β = -.425, p < .05) (cf. Table
The variables support/depth and satisfaction generated a significant model in step 1, along with the interaction term in the third. The interaction term (support/depth * satisfaction) proved to be a significant predictor, explaining 35.6% of the variance in depressive symptomatology (cf. Table
satisfaction and interaction term for males (
Observing the graph obtained for the male gender, and considering the main effect of sup-port/depth, lower levels of this variable predict greater depressive symptomatology. When support/depth is high, the symptomatology tends no to differentiate. Regarding the interaction effect, it reproduces what was already observed in the previous figure; high levels of support/depth seems to work as a protection factor of depressive symptoms, not seeming to be relevant the effect of satisfaction (approximation of levels of satisfaction low, medium and high when support/depth is high). In turn, when support/depth is low, low satisfaction levels (compared to high or medium) lead to greater depressive symptomatology (cf. Figure
4. Discussion
Literature has demonstrated an association between low social support and high conflict in pa-rental relationships with the development of depression (Cheng et al., 2014; Cole & McPherson, 1993; Lewinsohn et al., 1994; Lee et al., 2006; McFarlane et al., 1994; Smojver-Ažić1 & Bezinović, 2011). In this regard, studies have shown that positive family relationships can act as protective factors in the onset of depressive symptomatology (Cheng et al., 2014; Lewinsohn et al., 1994; Reinherz et al., 1993). In this investigation, specific characteristics existent in the relationships between adolescents and their parents were studied. This was the first study to analyze existing associations between the dimensions support/depth and conflict, evaluated by the parents (through the QRI-PP), and depressive symptoms in adolescents. In this study, these dimensions are not significantly associated with depressive symptomatology, contrary to what happened in previous studies, where they were evaluated by children’s perception, using the QRI (Matos et al., 2013; Pinheiro et al., 2013).
Some studies report that a poor global PF relates to depressive symptoms (Lewinsohn et al., 1994; Lewinsohn et al., 1998; McCabe, et al., 2011). Other authors have studied more specifically the relationship between some fields of the PF, such as school performance (Chen & Li, 2000; Fröjd et al., 2008), the quality of the relationships with the family (Matos et al., 2013; Pinheiro et al., 2013) and friends (Greca & Harrison, 2005) and recreational activities (Gledhill & Garralda, 2010), and satisfaction functioning in various areas of life (Koivumaa-Honkanen et al., 2001; Rissanen et al., 2011) and depressive symptoms in adolescence. This investigation the PF global and its various areas was studied, finding that the depressive symptoms are associated with PF global and with satisfaction with functioning, as with almost all dimensions of PF (relationships with family and friends and existence of recreational activities). These relations suggest that higher levels of functioning and satisfaction are associated with fewer depressive symptoms in adolescence. These data meet results obtained in other studies (Costa, 2011; Goldstein et al., 2009). A significant relationship between school performance and depressive symptoms was not found, unlike what Fröjd et al. (2008) obtained. In fact, family relations correlated with depression in the dimensions of the PF, contrary to what occurred in the QRI-PP, which can be explained by the fact that more relationships are included in these (not just father and/or mother) and because we are dealing with different information sources.
Significant differences in depressive symptoms for gender were also found, with girls having higher values of depression, what meets findings in literature (Essau et al., 2010; Galambos et al., 2004; Saluja et al., 2004). Boys reported more satisfaction with functioning than girls, which confirms the results obtained by Goldbeck, et al. (2007). With respect to parents’ perception of support/depth in the relationships with the children, it was found that these values were higher in boys.
The possible interaction effects were explored, and a moderator effect of school performance and satisfaction in the relationship between parents/children relationships – parents’ perception (support dimension/depth) and depressive symptomatology. When effect of school performance was tested for the total sample, results showed a predictor effect of support/depth and of the interaction term. Thus, having high levels of support/depth seems to work as a protection factor of depressive symptomatology, since, regardless of academic performance levels, no significant differences in depressive symptoms are found. The same is not true when support/depth of the relationship is low, since when school performance is low, there is an increase in depressive symptoms. Analyzing this effect of moderation for the two genders, only a significant moderator effect was found for females. Thus, and considering the main effect of school performance, similar results to those obtained for the total sample were found: lower levels on this variable seems to predict greater depressive symptomatology. However, when support/depth is high, the symptoms tend no to differentiate, whether school
performance is low or high..
With regard to the moderator effect of satisfaction for the total sample, one can say that satisfac-tion and the interaction term were predictors of depressive symptoms. It was observed that having high levels of support/depth seems to work as a protective factor of depressive symptomatology when satisfaction is low or medium; and seems to contribute to a smaller development of depressive symptoms when satisfaction is high. When support/depth is low, the same is not observed: when satisfaction is low or medium, there is a significant increment in depressive symptoms - stressing that the satisfaction, when support/depth is smaller, plays an important role in predicting this symptomatology. Analyzing this effect of moderation for the two genders, we found a significant interaction effect only in the male sample. Thus, having high levels of support/depth seems to work as a protector factor of depressive symptomatology in males. In turn, when support/depth is low, low satisfaction levels (compared to high or medium) lead to greater depressive symptomatology. These results suggest, that in adolescents, school performance and satisfaction with functioning, as well as the support/depth in parents/children relationships, can act as protective factors for the development of depressive symptoms, interacting with each other. It was interesting to note the existence of a gender effect: school performance acts as a moderator just for girls while satisfaction with life assumes this role in boys. In future studies it is intended to deepen the sociocultural influence on gender and its role in relations that are established between parents and children and vulnerability/protection for the development and maintenance of depressive symptoms in adolescence.
This research has some limitations that should be taken into consideration in the interpretation of the results: the small size of the sample, as well as its constitution (mostly female, both in students and in parents). We must be aware that other variables may have influenced the responses obtained in self-report instruments, such as social desirability, fatigue and demotivation, that may have been due to the extension of the research protocol used, which consists of various scales. In the future, it would be relevant to develop studies with larger samples, more balanced in terms of gender and covering other age groups (e.g. children and the elderly). Longitudinal research and clinical samples should also be developed.
It should be noted that this research is an innovative study by studying PF moderator effect and taking into account the perspective of the parents in the assessment of the quality of the relationships that they have with their children. These relationships can be important mechanisms of depression in adolescence. We also highlight the importance of developing strategies to improve PF in general, as well as relationships with family and friends, recreational activities, school performance and satisfaction, in the prevention and treatment of relapse in depression during adolescence.
Acknowledgements
We would like to express our gratitude to all the participants that made this study possible and to FCT that funded the study. This work is funded by ERDF – European Regional Development Fund through the COMPETE Program (operational program for competitiveness) and by National Funds through the FCT – Fundação para a Ciência e a Tecnologia (Portuguese Foundation for Science and Technology) within project “Prevention of depression in Portuguese adolescents: efficacy study of an intervention with adolescents and parents” (PTDC/MHC-PCL/4824/2012).
References
- American Psychiatric Association., (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.).
- (), Arlington, VA: Author.
- Bahls, S. C.Bahls, F. (2002). Depressão na adolescência: Características clínicas [Depression in adoles-.
- (), cence: Clinical features] Interação em Psicologia, 6 (1), 49-57. doi:0021-7557/02/78-05/359
- Bahls, S. C. (2002). Aspectos clínicos da depressão em crianças e adolescentes [Clinical aspects of depression.
- (), in children and adolescents] Journal de Pediatria, 78 (5), 359-366. doi:10.1590/S0021-
- (), 75572002000500004
- Baron, R.Kenny, D. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations.1037/0022-3514.51.. Journal of Personality and Social Psychology,– 10. 6.1173 Birmaher, B., Ryan, N. , 51(6), 1173-, 1182. doi
- Cheng, Y.Li, X.Lou, C.Sonenstein, F.Kalamar, A.Jejeebhoy, S.Ojengbede, O.Nolen-Hoeksema, S.Hilt, L. (2014). The associ-ation between social support and mental health among vulnerable adolescents in five cities: Findings from the study of the well-being of adolescents in vulnerable environments. A developmental psychopathology perspective on adolescent depression. , Handbook of Depression in Adolescents (pp. 3-32).. Journal of Adolescent Health, Cicchetti, D., & Toth, S. (2009). New York, NY. , 55, S31-S38. doi:10.1016/j.jadohealth.2014.08.020
- Cole, D.McPherson, A.Lerner, R.Steinberg, L. (1993). Relation of family subsystems to adolescent depression: Implementing a new family assessment strategy. Children’s over- and underestimation of academic competence: A longitudinal study of gender differences, depression, and anxiety. Child Development, 70 (2), 459–473. doi:0009-3920/99/7002-0014 Compas, B. (2004). Processes of risk and resilience during adolescence: Linking contexts and individuals. , Handbook of Adolescent Psychology (2nd ed., pp. 263-299).. Journal of Famify Psychology, Cole, D., Martin, J., Peeke, L., Seroczynski, A., & Fier, J. (1999). Hoboken, NJ: Jonh wily & Sons, Inc. , 7(1), 119-133. doi:10.1037/0893-3200.7.1.119
- Costa, A. (2011). Tradução da Entrevista A-LIFE - Adolescents Longitudinal Interval Follow-up Evaluation - Estudo Preliminar do Funcionamento Psicossocial numa Amostra de Adolescentes Portugueses [Translation of A-LIFE - Adolescents Longitudinal Interval Follow-up Evaluation - Preliminary Study of Psychosocial Functioning in a Sample of Portuguese Adolescents](Unpublished master’s thesis). Faculty of Psychology and Educational Sciences, University of Coimbra, Coimbra, Portugal
- Dias, P.Gonçalves, M. (1999). Avaliação da ansiedade e da depressão em crianças e adolescentes (STAIC-C2, CMAS-R, FSSC-R e ): Estudo normativo para a população portuguesa [Anxiety and depression assessment in children and adolescentes (STAIC-C2, CMAS-R, FSSC-R e ): Normative study for the Portuguese population]. In, S. Araújo, & S. Caires (Orgs.). Avaliação Psicológica: Formas e Contextos, 6, 553-564, CDI, A. Soares
- Eccles, J.Lord, S.Roeser, R. (1996). Round holes, square pegs, rocky roads, and sore feet: The impact of stage-environment fit on young adolescents' experiences in schools and D. Cicchetti & S. , families. In
- (), Toth (Eds.), Rochester Symposium on Developmental Psychopathology: Vol 7. Adolescence: Opportunities and challenges (pp. 47-92). Rochester, NY: University of Rochester Press.
- Essau, C.Lewinsohn, P.Seeley, J.Sasagawa, S. (2010). Gender differences in the developmental course of depression. Journal of Affective Disorders, 127, 185-190. doi
- Fergusson, D.Woodward, L. (2002). Mental health, educational, and social role outcomes of adolescents.
- (), with depression. Archives of General Psychiatry, 59 (3), 225-231. doi:10.1001/archpsyc.59.3.225
- Fried, E.Nesse, R. (2014). The impact of individual depressive symptoms on impairment of psychosocial.
- (), functioning. PLOS ONE, 9 (2), 1-7. doi:10.1371/journal.pone.0090311
- Fröjd, S.Nissinen, E.Pelkonen, M.Marttunen, M.Koivisto, A.Heino, R. (2008). Depression and school performance in middle adolescent boys and girls. Journal of Adolescence, 31, 485-498
- Galambos, N.Leadbeater, B.Barker, E. (2004). Gender differences in and risk factors for depression in adolescence: A 4-year longitudinal study. The short-term outcome of depressive disorder in adolescents attending primary care: A cohort study. Social Pshychiatry and Psychiatric Epidemiology, 46 (10), 993–1002. doi: 10.1007/s00127-010-0271-6 Goldbeck, L., Schmitz, T., Besier, T., Herschbach, P., & Henrich, G. (2007). Life satisfaction decreases dur-ing adolescence. Quality of Life Research, 16, 969–979. doi:10.. International Journal of Behavioral Development, Gledhill, J., & Garralda, M. (2010). 1007/s11136-007-9205-5 Goldstein, T., Birmaher, B., Axelson, D., Goldstein, B., Gill, M., Emposito-Smythers, C., …Keller, M. , 28(1), 16-25. doi:10.1080/01650250344000235
- (2009). Psychosocial functioning among bipolar youth.1207/s15374424jccp3401_5 Greer, T., Kurian, B., & Trivedi, M. (2010).. Adolescent peer relations, friendships, and romantic relationships: Do they predict social anxiety and depression? Journal of Clinical Child and Adolescent Psychology, 34 (1), 49–61. doi:10. Defining and measuring functional recovery from depression. , 144(1-3), 174-183. doi:10.1016/j.jad.2008.07.001
- CNS , Drugs.Harrington, R.Vostanis, P. (1995). Longitudinal perspectives and affective disorder in children and I. Goodyer (Ed.), The depressed child and adolescent: developmental and clinical perspectives. , 311-345, ado-lescents. In
- Holmbeck, G. (1997). Toward terminological, conceptual, and statistical clarity in the study of mediators and moderators: examples from the child-clinical and pediatric psychology literatures. Journal of Consulting and Clinical Psychology, 65(4), 599-610
- Keller, M.Lavori, P.Friedman, B.Nielsen, E.Endincott, L.McDonald-Scott, P.Andreasen, N. (1987)
- Kline, R. (2011). Principles and practice of structural equation ed.). , modeling. (3rd
- Koivumaa-Honkanen, H.Honkanen, R.Viinamäki, H.Heikkilä, K.Kaprio, J.Koskenvuo, M. (2001)
- Life satisfaction and suicide: A 20-Year Follow-Up Study. American Journal of Psychiatry, 158 (3), 433–439. doi: 10.1176/appi.ajp.158.3.433 Kovacs, M., (1985). The Children's Depression Inventory (CDI). Psychopharmacology Bulletin (21),, M., Wong, B., Chow, B., & McBride-Chang, C. (2006). Predictors of suicide ideation and depression in Hong Kong adolescents: Perceptions of academic and family climates. Suicide and Life-Threatening Behavior,. doi:10.1521/suli.2006.36.1.82 Lewinsohn, P., Hoberman, H., & Rosenbaum, M. (1988). A prospective study of risk factors for unipolar depression.1037/0021-843X.97.3.251 Lewinsohn, P., Roberts, R., Seeley, J., Rohde, P., Gotlib, I., & Hops, H. (1994). Adolescent psychopathology: II. Psychosocial risk factors for depression.. Journal of Abnormal Psychology, 103 (2), 302-315. , 36(1), 82-96, 995-998. Lee
- Lewinsohn, P.Rohde, P.Seeley, J. (1998). Major depressive disorder in older adolescents: Prevalence, risk factors, and clinical implications. Clinical Psychology Review, Lewinsohn, P., Rohde, P., Seeley, J., Klein, D., & Gotlib, I. (2003). Psychosocial functioning of young adults who have experienced and recovered from major depressive disorder during adolescence.1037/0021-843X.112.3.353 Lieb, R., Isensee, B., Höfler, M., Pfister, H., & Wittchen, H. (2002) Parental major depression and the risk of depression and other mental disorders in offspring: A prospective-longitudinal community study.. Journal of Abnormal Psychology, 112 (3), 353–363. doi:10. Ar-. , 18(7), 765-794. doi:10.1016/S0272-7358(98)00010-5
- (), chives of General Psychiatry, 59 (4), 365-374. doi: 10.1001/archpsyc.59.4.365
- Marôco, J. (2010). Análise de equações estruturais: fundamentos teóricos, software & aplicações [Analysis of structural equations: Theoretical foundations, software & applications]. Pero Pinheiro, Portugal: Report Number
- Marujo, H. (1994). Síndromas depressivos na infância e na adolescência [Depressive syndromes in childhood and adolescence] (Unpublished doctoral dissertation). Faculty of Psychology and Educational Sciences, University of Lisbon, Portugal
- Masten, A.Coatsworth, J. (1995). Competence, resilience, and D. Cicchetti & D. , psychopathology. In
- (), Cohen (Eds.). Developmental psychopathology: Risk, disorder, and adaptation (Vol. 2, pp. 715-752). New York: Wiley.
- Matos, A. P.Costa, A. (2011). Estudo das propriedades psicométricas da entrevista Adolescents Longitudi-nal Interval Follow-up Evaluation (A-LIFE). [Study of Psychometric properties of the interview Adolescents Longitudinal Interval Follow-up Evaluation (A-LIFE)] (Unpublished manuscript)
- Matos, A.Pinheiro, M.Marques, D. (2013). A qualidade do relacionamento interpessoal com o pai: adaptação e validação do Quality of Relationships Inventory (QRI), numa amostra de adolescentes portugueses [The quality of the interpersonal relationship with the father: adaptation and validation of the Quality of Relationships Inventory (QRI) in a sample of Portuguese adolescents]. Symposium conducted at the meeting of the First World Congress of Children and Youth Health Behaviors, , M., Ricciardelli, L., & Banfield, S. (2011). Depressive symptoms and psychosocial functioning in preadolescent children. Depression Research and Treatment, 2011, 1-7. doi:10.1155/2011/548034 McFarlane, A., Bellissimo, A., Norman, G., & Lange, P. (1994). Adolescent depression in a school-based community sample: Preliminary findings on contributing social factors.. Journal of Youth and Adolescence. , 23(6), 601-620, Portugal. McCabe
- Mehta, S.Mittal, P.Swami, M. (2014). Psychosocial functioning in depressive patients: A comparative study between major depressive disorder and bipolar affective disorder.. Depression Research and Treatment. 1155/2014/302741. , 2014, 10-, 1-6. doi
- Neves, C.Pinheiro, M. (2009). A qualidade dos relacionamentos interpessoais com os amigos: adaptação e validação do Quality of Relationships Inventory (QRI) numa amostra de estudantes do ensino superior [The quality of interpersonal relationships with friends: adaptation and validation of the Quality of Relationships Inventory (QRI) in a sample of higher education students]. Exedra, . Pestana, M. & Gageiro, J. (2008).. Análise de dados para as Ciências Sociais: A Complementaridade do SPSS[Data analysis for the Social Sciences: The complementarity of the SPSS] (5th ed.). Lisboa, Portugal: Edições Sílabo. , 2, 1646-9526, 9-31. ISSN-e
- Pierce, G.Sarason, I.Sarason, B. (1991). 1037/0022-3514.61.6.1028 Pinheiro, M., Matos, A., & Marques, D. (2013). A qualidade do relacionamento interpessoal com a mãe: adaptação e validação do Quality of the Interpersonal Relationships Inventory (QRI), numa amostra de adolescentes portugueses [The quality of the interpersonal relationship with the mother: adaptation and validation of the Quality of Relationships Inventory (QRI) in a sample of Portuguese adolescentes].. General and relationship-based perceptions of social support: are two constructs better than one? Journal of Personality and Social Psychology. Symposium conducted at the meeting of the First World Congress of Children and Youth Health Behaviors, Viseu, Portugal. , 61(6), 10-, 1028-1039. doi
- Pinheiro, M.Matos, A.Mota, A.Marques, C.Costa, J. (2015). Study of the psychometric properties of the Quality of Relationships Inventory – Parents Perception (QRI-PP). Unpublished manuscript
- Pomerantz, E.Altermatt, E.Saxon, J. (2002). Making the grade but feeling distressed: Gender differences in academic performance and internal distress. Journal of Educational Psychology, 94(2), 396-404
- Puig-Antich, J.Kaufman, J.Ryan, N.Williamson, D.Dahl, R.Lukens, E.Nelson, Y. (1993). The psy-chosocial functioning and family environment of depressed adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, Reinherz, H., Giaconia, R., Pakiz, B., Silverman, A., Frost, A., & Lefkowitz, E., 32(2), 244-253. doi:10.1097/00004583-199303000-00003
- Rissanen, T.Viinamäki, H.Honkalampi, K.Lehto, S.Hintikka, J.Saharinen, T.Koivumaa-Honkanen, H. (2011). Long term life dissatisfaction and subsequent major depressive disorder and poor mental Psychiatry,. doi:10.1186/1471-244X-11-140 Rueger, S., Malecki, C., & Demaray, M. (2008). Gender differences in the relationship between perceived social support and student adjustment during early adolescence. School Psychology Quarterly, 23 (4), 496 -514. doi:10.1037/1045-3830.23.4.496 Rueger, S., Malecki, C., & Demaray, M. (2010).. Relationship between multiple sources of perceived social support and psychological and academic adjustment in early adolescence: Comparisons across gender. , 11(140), 2-6, health. BMC
- s10964-008-9368-6 Saluja, G.achan, R.Scheidt, P.Overpeck, M.Sun, W.Giedd, J. (2004). Prevalence of and risk factors for depressive symptoms among young adolescents. Archives of Pediatrics and Adolescent Medicine, Sanford, M., Szatmari, P., Spinner, M., Munroe-Blum, H., Jamieson, E., Walsh, C., & Jones, D. (1995). Pre-dicting the one-year course of adolescent major depression.1097/00004583-199512000-00012 Sheeber, L., Hops, H., Alpert, A., Davis, B., & Andrews, J. (1997). Family support and conflict: Prospective relations to adolescent depression.. Journal of Abnormal Child Psychology, 25 (4), 333-344. , 158(8), 760-765. doi:10.1001/archpedi.158.8.760
- A:1025768504415 Slavich, G.Monroe, S.Gotlib, I. (2011). Early parental loss and depression history: Associations with recent life stress in major depressive disorder. Journal of Psychiatric Research, 45(9), 1146-1152
- Smojver-Ažić, S.Bezinović, P. (2011). Sex differences in patterns of relations between family interactions depressive symptoms in adolescents.3325/cmj.2011.52.469 Smucker, M., Craighead, W., Craighead, L. & Green, B. (1986). Normative and reliability data for the Chil-dren's Depression Inventory.. Journal of Abnormal Child Psychology, 14 (1), 25-39. , 52(4), 469-477. and
- BF00917219 Steele, R.Little, T.lardi, S.Forehand, R.Brody, G.Hunter, H. (2006). A confirmatory comparison of the factor structure of the Children’s Depression Inventory between European American and African American youth.1007/s10826-006-9054-9 World Health Organization. (2008).. Journal of Child and Family Studies. The Global Burden of Disease: 2004 Update. , 15, 10-, 779-794. doi
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
03 August 2015
Article Doi
eBook ISBN
978-1-80296-005-1
Publisher
Future Academy
Volume
6
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-220
Subjects
Child psychology, psychology, developmental psychology, psychological testing, psychological measurement, family psychology
Cite this article as:
Mota, A., Matos, A. P., Pinheiro, M. R., Costa, J. J., & Oliveira, S. (2015). Familial relationships perceived by parents and adolescent depression: Psychosocial functioning moderating effect. In Z. Bekirogullari, & M. Y. Minas (Eds.), Cognitive - Social, and Behavioural Sciences - icCSBs 2015, August, vol 6. European Proceedings of Social and Behavioural Sciences (pp. 21-37). Future Academy. https://doi.org/10.15405/epsbs.2015.08.4