
Recovery of Patients With Lombosacrate Algofunctional Syndrome Through Specific Physiokinetotherapeutic Means


Abstract
Lumbosacral algofunctional syndrome is an arthritic disease, characterized by damage to the articular cartilage, being a common condition that appears as acute or chronic pain. Low back pain is currently one of the most common conditions, with a great medical and social significance, due to the increased frequency in large categories of the population, but especially in the young population, active through the effects that suffering has. In Western societies, from an economic point of view, of all neurological and psychiatric conditions, chronic pain is by far the most costly, due to the associated impact on the active population and the care requirements of the elderly. This enormous burden on society is not fueled in any way by the inadvertence of pharmacology-based treatments, especially for severe pain. Medical technology has the potential to become an integral part of the diagnosis and treatment of pain. In this study, we examine whether the technology can provide a new direction in the management of pain present in lumbosacral algofunctional syndrome through a different approach to kinetic recovery. The aim of this study is to demonstrate the effectiveness of the intervention on the content of the recovery program, by including a complementary therapy in order to make it more efficient in ameliorating lumbosacral algofunctional syndrome. The abstract should be presented as a single paragraph and briefly summarize the goals, methods, and new results presented in the manuscript. Reference citations are not allowed.
Keywords: Equispinen, lumbosacral algofunctional syndrome, recovery
Introduction
Globally, years of disability with low back pain increased by more than 50% between 1990 and 2015, mainly due to population growth and aging, with the largest increase observed in low- and middle-income countries. Low back pain is now the leading cause of disability worldwide. For almost all people with low back pain, it is not possible to identify a specific nociceptive cause (Shipton, 2018).
Low back pain is a very common symptom that occurs in high-income, middle-income and low-income countries and all age groups, from children to the elderly. The incapacity and costs associated with low back pain are projected to increase in the coming decades, especially in low- and middle-income countries, where health and other systems are often fragile and not equipped to cope with this growing burden. Research in the field is clearly needed to address the issue of low back pain (Freburger et al., 2011).
Physical therapy and occupational therapy, as well as other forms of physical activity are valuable, most specialized guides recommend non-pharmacological and non-invasive management, patients can also benefit from cognitive-behavioral therapy, because low back pain has a psychosocial dimension (Pergolizzi & LeQuang, 2020).
Problem Statement
Although health education systems have been organized (low back school) it is hard to believe that the whole issue of low back pain can be covered by a few standardized programs, even if they are realized on concrete data of complete balance sheet and are followed conscientiously (Maher, 2004).
The research highlights the need for intervention on the content of the recovery program by including a complementary therapy in order to make it more efficient for the improvement of the lumbosacral algofunctional syndrome. The data provided by the application of physiotherapy sessions and Equispine therapy, which emphasize the need to maintain a correct postural attitude, and in addition to physiotherapy sessions, led us to apply complex physiotherapy programs to patients with lumbosacral algofunctional syndrome.
Research Questions
Given the complexity of the intervention plan mentioned in the literature for subjects with lumbosacral algofunctional syndrome, this study raises the following questions:
Can the identification and application of the complex recovery program by integrating Equispine therapy be correlated with the increase in the efficiency of recovery through physiotherapy?
Does the use of the complex recovery program through the integration of Equispine therapy allow a better dynamic follow-up of the effectiveness of the applied therapeutic exercise?
Purpose of the Study
The aim of this paper is to carry out a scientific approach to demonstrate the effectiveness of the intervention on the content of the recovery program, by including a complementary therapy in order to make it more efficient for the improvement of lumbosacral algofunctional syndrome. .
Research Methods
The study was carried out at the Ortokineto Sport recovery center in Piteşti, for a period of 3 months, by applying physiotherapy sessions three times a week, for 60/90 minutes, to which was added Equispine therapy, with participation of 10 subjects, 5 female and 5 male, from different social backgrounds, participant’s characteristics are presented in table 1.
The inclusion criterion was the presence of low back pain at the time of assessment, with a level of self-assessment in the last 7 days greater than or equal to 3, on a scale of 1 to 10.
Exclusion criteria were those that may be associated with back pain, but refer to other conditions, such as: congenital bone conditions, degenerative bone and joint conditions, lower limb surgery, spinal cord and back injuries.
Equispine comes with a very important contribution in achieving the balance of muscle tone at the level of the spine on the background of restoring muscle mass and implicitly of the functionality with the help of some therapeutic exercises of movement control. Movements performed in Equispine therapy have a major advantage with a permanent visual feedback of control over the movements performed by the patient. All this information, which the patient has at his disposal with the help of the software, helps him to control his movements so that he is as close as possible to the optimal parameters set on the monitor.
The following methods were used to achieve the proposed purpose and objectives:
Bibliographical research method - to make the approached theme’s theoretical profile
Observation method - to see and assess the progress of the degree of disability of the subjects during the study
Questionnaire survey method - to confirm/ infirm the efficiency of the kinetic treatment carried out using initial and final assessments made to the subject about gradul de dizabilitate
The Analog Visual Scale was used to assess the intensity of current pain before and after each physiokinetotherapy session, under the guidance of the physiokinetotherapist. The scale measures the intensity of subjective pain from 0 = no pain to 10 = the most intense pain imaginable. The level of disability was measured using the Oswestry Disability Index (ODI) questionnaire to determine lumbar spine dysfunction due to pain that provides information on how back pain affects the ability to manage daily life. The questionnaire consists of ten sections, each with 6 possible answers. Statement 1 is marked with 0 points; statement 6 - with 5 points. A total score of 50 points indicates a 100% disability, and a total score of 10 points indicates a 20% disability. The measurement of chronic disability for patients with low back pain was performed with the Chronic Disability Index of Waddell and Main for Patients with Low Back Pain, a questionnaire comprising 9 items (0 = minimum score; 9 = maximum score). Disability due to low back pain was measured using the Roland and Morris Low Back Pain Disability Questionnaire, which included 24 items (0 = minimum score; 24 = maximum score). A higher score or = 14 indicates a severely affected patient. Each patient answered the questionnaires individually, both at the time of the initial assessment and at the time of the final assessment.
basic statistics methods (numerical and graphic methods) - to render the evolution and trends of the data collected
Representation of the data gathered found the basic notions of the study as well as directions to apply practical conclusions about the effectiveness of the kinetic treatment underwent by the subject with lumbosacral algofunctional syndrome.
Findings
A comparative examination of the level of functional disability of the lumbar spine at the beginning and end of the program shows an average difference of 28.9 for ODI, 5.00 for LBP-WM, 14.50 for LBP-RM and 6.10 for VAS.
There is also an average difference of 1.10 for weight and 0.39 for BMI between the start and end of the test. The differences between the moments of testing, at the beginning and at the end of the intervention, in terms of the level of lumbar disability were statistically significant, as well as the weight and body mass index. Table 2 shows the results mentioned.
SD – standard deviation; ODI – Oswestry Disability Index, LBP-WM - Chronic Disability Index of Waddell and Main, LBP-RM - Low Back Pain Disability of Roland and Morris, VAS – Visual Analogue Scale;
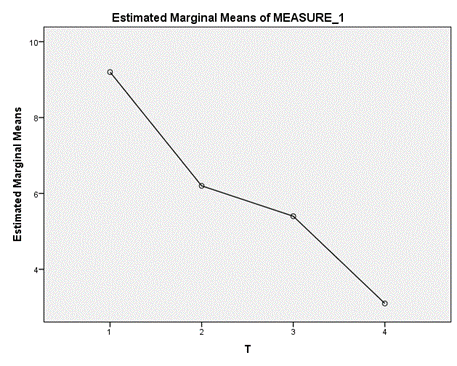
The results also indicated that patients had progressed throughout pain intensity therapy. There are statistically significant differences [F (3.27) = 88.93, p = 0.000] between the first, second and third month of physiokinetotherapeutic intervention, in terms of pain intensity, according to VAS.
The Bonferroni post hoc test shows that the average score at the end of the test (M = 3.10, σ = 0.994) was significantly lower than at the start of the test (M = 9.20, σ = 0.789), in the first month of testing (M = 6.20, σ = 1.317) or in the second month of testing (M = 5.40, σ = 1.265) (Table 3).
The change in pain intensity during the assessment stages was carefully monitored by the physiotherapist (Figure 1).
The results of the statistical data processing supported our hypothesis regarding the effectiveness of the use of this technique in the recovery programs of patients with lumbosacral algofunctional syndrome.
Conclusions
Study of the literature on the kinetic recovery mechanisms of lumbosacral algofunctional syndrome, reflects the influence of endogenous and exogenous factors that disrupt the body posture attitude causing the installation of functional physical deficiencies, thus, it is necessary to combine kinetic methods and techniques in order to recover the lumbosacral algofunctional syndrome (Hartvigsen et al., 2018).
Using the main objectives of sensory-motor correction of body position with proprioceptive stimuli (muscle, ligament, joint capsule) and exteroceptive stimuli (multiple and varied interventions and indications of the specialist and equipment, ie cognitive feedback), we can manage to make the patient aware of the vicious position he is taking, helping the brain to analyze and adopt the positions necessary for recovery at the cortical and subcortical level.
Visual feedback is very important in the economy of the recovery process, all this visual information obtained with the help of the accessories we have available in the recovery room, mirrors, laptop for Equispine therapy, helps us a lot in the therapeutic process.
What we can say with certainty is that while the patient is working without permanent visual feedback, traction movements are no longer so consistent and controlled, and the parameters measured by the Equispine device confirm this information. This program tries to correct the position of the spine and activates the superficial and deep muscle groups at the level of the spine and has a positive effect in combating back pain.
Following the program applied in order to develop muscle mass and functional rebalancing of muscles an important improvement was reached, by supporting some physical efforts that previously could not be achieved and, in addition, the psychic component obviously generated by the aspect of the deformation was obviously improved, realizing a psychic structure of a normal macroscopic person.
References
Freburger, J. K., Carey, T. S., & Holmes, G. M. (2011). Physical Therapy for Chronic Low Back Pain in North Carolina: Overuse, Underuse, or Misuse? Physical Therapy, 91(4), 484-495. DOI:
Hartvigsen, J., Hancock, M. J., Kongsted, A., Louw, Q., Ferreira, M. L., Genevay, S., Hoy, D., Karppinen, J., Pransky, G., Sieper, J., Smeets, R. J., Underwood, M., Buchbinder, R., Hartvigsen, J., Cherkin, D., Foster, N. E., Maher, C. G., Underwood, M., van Tulder, M., … Woolf, A. (2018). What low back pain is and why we need to pay attention. The Lancet, 391(10137), 2356-2367. DOI:
Maher, C. G. (2004). Effective physical treatment for chronic low back pain. Orthopedic Clinics of North America, 35(1), 57-64. DOI: 10.1016/S0030-5898(03)00088-9
Pergolizzi, J. V., Jr., & LeQuang, J. A. (2020). Rehabilitation for Low Back Pain: A Narrative Review for Managing Pain and Improving Function in Acute and Chronic Conditions. Pain and Therapy, 9(1), 83-96. DOI:
Shipton, E. A. (2018). Physical Therapy Approaches in the Treatment of Low Back Pain. Pain and therapy, 7(2), 127–137. DOI:
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
10 April 2023
Article Doi
eBook ISBN
978-1-80296-961-0
Publisher
European Publisher
Volume
5
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-1463
Subjects
Education sciences, teacher education, curriculum development, educational policies and management
Cite this article as:
Sorinel, D. G., & Luminiţa, G. (2023). Recovery of Patients With Lombosacrate Algofunctional Syndrome Through Specific Physiokinetotherapeutic Means. In E. Soare, & C. Langa (Eds.), Education Facing Contemporary World Issues - EDU WORLD 2022, vol 5. European Proceedings of Educational Sciences (pp. 1293-1298). European Publisher. https://doi.org/10.15405/epes.23045.130