
Social Beliefs About Complaints In Interpersonal Communication And Subjective Pain


Abstract
Both common-sense model of health and illness and psychological model of body functions regulation suggest that any uncomfortable sensations make the person to look for their meaning in the world that could further lead to symptoms’ perpetuation. The study suggests that subjective beliefs about functions of pain-related complaints in interpersonal communication are related to pain severity in general population. 113 adults without severe somatic or mental illnesses appraised 9 wide-speeded pain complaints (headache, heartache, back pain etc.) by 6 functions they could be used for in the communication (“to make excuse”, “to blame others”, “to gain profit”, “to have or support own social status”, “to receive emotional support”, “to receive instrumental support”). Then they appraised to what degree they experience each type of pain themselves and filled Cognitions about Body and Health Questionnaire and Health Values Scale. For six out of nine pain types subjective beliefs in their usefulness in communication were related to their subjective severity (r=.20-.32). For abdominal pain, headache, heartache, pain in eyes and toothache social beliefs predicted pain severity after adjusting for other cognitive factors of somatization adding 4.4%-10.5% to the explained variance of pain severity.
Keywords: Cognitive factors of somatizationgeneral populationinterpersonal communicationpainsocial beliefs about pain
Introduction
Cross-cultural studies demonstrated that cultural differences in self-reported symptoms might be explained by differences in interoceptive perception and consequent different social expectations regarding way of sharing poor well-being with others (Ma-Kellams et al., 2012). Both common-sense model of health and illness (Leventhal et al., 2003) and psychological model of body functions regulation (Tkhostov, 2002) suggest that any uncomfortable sensations make the person to look for their meaning in the world. Subjective representation of symptoms that person constructs, further regulate his or her complaints as well as decisions in treatment and could lead to symptoms’ perpetuation. This is especially important for complaints on pain due to difficulties of its objective verification and so high dependence on psychological and social factors.
Based on these models we suggested that at least somatic complaints frequent in general population are related to specific social beliefs describing situations when these complaints could be used in the interpersonal interactions (Rasskazova & Migunova, 2014). Particularly, people tend to complaint on some somatic problems more if these complaints could help to receive emotional or instrumental support, social status, to make excuse, to gain some profit, to blame others, etc. Social beliefs about symptoms might further become a factor of their perpetuation due to body monitoring and somatosensory amplification (Barsky & Wyshak, 1990), catastrophizing of body sensations or dysfunctional behavior (Rief et al., 1998). We also suggest that social beliefs about the role of symptoms in interpersonal communication could directly lead to higher complaints in people holding such beliefs. Empirical study of sleep-related complaints (poor sleep and sleepiness) in general population supported that they were related to social belief that such complaints are helpful in obtaining instrumental support (Rasskazova, 2019). This effect remained after adjusting for other cognitive factors of somatization (Rief et al., 1998).
Problem Statement
This study is focused on wide-spreaded pain-related complaints in general population: abdominal, joint, back pain, pain in the eyes, in the arms and legs, headache, heartache, toothache and sore throat.
Research Questions
The aim was to reveal the relationship between pain-related complaints and subjective beliefs about their role in interpersonal communication in general population.
Purpose of the Study
In line with psychological model of body functions regulation we hypothesized that:
The more people believe that some pain-related complaints could be beneficial in interpersonal communication, the higher the probability that they themselves report such complaints.
Some social functions are more typical for some pain-related complaints than for other.
The relationship between social beliefs about functions of complaints and pain remains after adjusting for cognitive beliefs about body, health and illness.
Research Methods
Sample
113 adults living in Moscow or Moscow region, Russia (28 males, 24.8%) 21-76 years old (mean age was 37.8±15.2 years old) without chronic somatic illnesses related to pain and refusing mental health diagnoses in the past participated in the study.
Methods
First, they read a text: “Sometimes person really has some complaint and at the same moment use it for some other purpose (for instance to make excuse for some responsibilities that he didn’t complete). Please, for each symptom below appraise how frequently, to your opinion, people complaint for their real symptoms to receive something from others”. Then they appraised a list of 39 different mental and somatic complaints by 0-10-points Likert scale (“0” – never and “10” – always) by six social functions (“to make excuse”, “to blame others”, “to gain profit”, “to have or support own social status”, “to receive emotional support”, “to receive instrumental support”). Nine pain-related symptoms included abdominal, joint, back pain, pain in the eyes, in the arms and legs, headache, heartache, toothache and sore throat. Others were used as distractors.
Second, participants appraised using 0-10-points Likert scale to what degree they experience each of the symptoms in their lives.
Finally, they filled Cognitions about Body and Health Questionnaire (Rief et al., 1998) and Health Values Scale (Rasskazova et al., 2016). Cognitions about Body and Health Questionnaire was developed to measure cognitive beliefs that are typical for patients with somatoform disorders and hypochondriac disorder and includes the next scales: Catasrophizing of Body Symptoms, Autonomic Sensations, Bodily Weakness, Intolerance of Bodily Complaints, Health Habits, Somatosensory Amplification. Health Values Scale assess cognitive beliefs in four different models of health and personal health care that are related to somatic complaints in general population: health as an exhaustible resource demanding for permanent defense and preservation, health as a capacity that could be lost and should be regularly monitored for possible risks, health as a necessary condition for success in life that might be achieved for money, health a mystical holistic thing that should be supported by alternative treatment only.
Data were processed in SPSS Statistics 23.0.
Findings
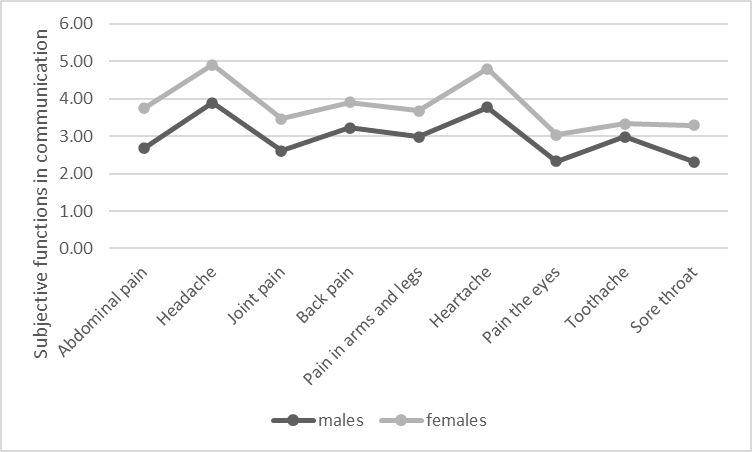
Subjective pain and social beliefs about functions of pain-related complaints in the interpersonal communication
As can be seen in Table
Beliefs about different functions of pain-related complaints in interpersonal communication demonstrated high consistency with each other (see Cronbach’s alphas in Table
Relationship between social beliefs about functions of complaints and different type of pain: the role of beliefs about health and body
Most pain-related complaints, except for joint pain, pain in arms and legs and sore throat are related to social beliefs that they could be used in interpersonal communication (Table
In line with the studies of cognitive factors of somatization (Rief et al., 1998), reports of autonomic sensations, belief in body weakness and somatosensory amplification are related to higher joint pain and toothache. Autonomic sensations and somatosensory amplification are higher in those complaining on abdominal pain, headache, backpain, heartache, pain in eyes and sore throat.
To reveal whether this effect of social beliefs is specific for different pain localizations or general for different types of pain we computed partial correlations between social beliefs about functions of complain and its severity after adjusting for social beliefs about other types of pain (so adjusting for 8 variables). Only for abdominal pain correlation remained significant (r=.21, p<.05) indicating that for most types of the pain in general population there is general not specific effect of social beliefs.
To test the hypothesis that subjective functions of complaints predict different types of pain after adjusting for cognitive beliefs about health and body we conducted a series of hierarchical regressions (for each pain-related complaint). Joint pain, pain in arms and legs and sore throat were not included in the analysis because their frequency was not related to their subjective functions in the communication. At Step 1 we included any beliefs about health and body that correlated with this complain in our sample (see Table
Conclusion
Due to correlational design this study does not allow to conclude whether people with higher pain-related complaints stronger believe that these complaints could be helpful in social interactions (for instance, as a coping with pain or due to more communication with others about their pain) or whether social beliefs about functions of pain-related complaints could be a factor for further pain perpetuation. Our data indicate that there is a relationship between personal beliefs about social functions of pain and subjective pain severity in general population. Moreover, in contrast with our second hypothesis, this relationship seems to be specific neither to concrete social functions (because social beliefs about different function of complain in communication are highly consistent with each other) nor to pain localization. The only exception is abdominal pain. It seems that social beliefs about complaints on abdominal pain could be specifically related to complaints regardless of beliefs about other types of pain.
We also found that the relationship between social beliefs about functions of pain-related complaints and complaints’ severity is not explained by other cognitive factors of somatization and hypochondrization. Indeed pain-related complaints were related to reported autonomic sensations, belief in bodily weakness and somatosensory amplification, but beliefs about social functions of symptoms still predicted pain severity after adjusting for other cognitive beliefs.
In general, the data are in line with both common-sense model of health and illness (Leventhal et al., 2003) and psychological model of body functions regulation (Tkhostov, 2002) suggesting that subjective meaning of pain could be important component illness representation probably affecting further pain worsening or perpetuation. Subjective beliefs that pain-related complaints could be helpful in interpersonal communication were related to subjective pain severity for five out of 9 types of pain (abdominal pain, headache, heartache, pain in eyes and toothache) after adjusting for other cognitive factors of somatization.
Further research is necessary for explain whether social beliefs could be a factor of pain perpetuation or just a consequence of pain-related experience.
Acknowledgments
Research was supported by the Russian Foundation for Fundamental Research, project 20-013-00799 «Social psychological mechanisms of somatization and hypochondrization in the informational society».
References
- Barsky, A., & Wyshak, G. (1990). Hypochondriasis and somatosensory amplification. The British Journal Of Psychiatry, 157, 404-409. https://doi.org/10.1192/bjp.157.3.404
- Leventhal, H., Brissette, I., & Leventhal, E. (2003). The common-sense model of self-regulation of health anf illness. In L.D. Cameron, & H. Leventhal (Eds.), The self-regulation of health and illness behavior (pp. 42-65). Routledge.
- Ma-Kellams, C., Blascovich, J., & McCall, C. (2012). Culture and the body: East-West differences in visceral perception. Journal Of Personality And Social Psychology, 102(4), 718-728. https://doi.org/10.1037/a0027010
- Rief, W., Hiller, W., & Margraf, J. (1998). Cognitive aspects of hypochondriasis and the somatization syndrome. Journal of Abnormal Psychology, 107(4), 587-595. https://doi.org/10.1037//0021-843x.107.4.587
- Rasskazova, E. (2019). Funktsii zhalob na narusheniya sna i sonlivost' v mezhlichnostnom obshchenii: kul'turno-istoricheskii podkhod v psikhosomatike [Functions of Complaints on Sleep Disturbances and Sleepiness in Interpersonal Communication: Cultural-Historical Approach in Psychosomatics]. Kul'turno-istoricheskaya psikhologiya, 15(4), 44-55. https://doi.org/10.17759/chp.2019150405 (In Russian, abstr. in English)
- Rasskazova, E., & Migunova, J. (2014). Funktsii somaticheskikh simptomov v mezhlichnostnom obshchenii: kul'turno-istoricheskii podkhod v psikhosomatike [Functions of somatic symptoms in interpersonal communication: cultural-historical approach in psychosomatics]. Kul'turno-istoricheskaya psikhologiya, 10(1), 79-87. (In Russian, abstr. in English)
- Rasskazova, E., Guldan, V., & Tkhostov, A. (2016). Psikhologicheskoe soderzhanie «ipokhondricheskogo diskursa»: svyaz' tsennosti zaboty o zdorov'e s otnosheniem k telu, bolezni i lecheniyu [Psychological meaning of “hypochondriacal discourse”: the relationship between value of health care and beliefs about body, illness and treatment]. Bulletin of the South Ural State University. Ser. Psychology, 9(2), 60–70. https://doi.org/10.14529/psy160207 (In Russian, abstr. in English)
- Tkhostov, A. (2002). Psikhologiya telesnosti [Psychology of corporeality]. Smysl. (In Russian)
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
15 November 2020
Article Doi
eBook ISBN
978-1-80296-093-8
Publisher
European Publisher
Volume
94
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-890
Subjects
Psychology, personality, virtual, personality psychology, identity, virtual identity, digital space
Cite this article as:
Rasskazova, E., & Tkhostov, A. (2020). Social Beliefs About Complaints In Interpersonal Communication And Subjective Pain . In T. Martsinkovskaya, & V. Orestova (Eds.), Psychology of Personality: Real and Virtual Context, vol 94. European Proceedings of Social and Behavioural Sciences (pp. 653-660). European Publisher. https://doi.org/10.15405/epsbs.2020.11.02.80