
Development Of Sleep Regulation In The Childhood: The Role Of Parental Mediation


Abstract
Based on the psychological model of body functions regulation, we suggested that psychological sleep regulation is developing during childhood and is affected by mediation strategies that parents use to support child’s sleep-wake cycle. 103 pairs of students and one of their parents replied six items on different parental sleep mediation strategies, filled Insomnia Severity Index, Dysfunctional Beliefs About Sleep Scale, Subjective Sleep Vulnerability Scale, Scale of Behavioral Factors of Sleep Disturbances. Parental control for bedtime when students were children is related to poorer students’ current sleep through higher probability of non-medication intake during poor sleep. The more parents worried about their sleep when they were children, the better evening sleep hygiene students demonstrate. They also go to bed earlier and have shorter sleep latency if their parents worried about their sleep when they were children. The more students in their childhood went to their parents if they couldn’t asleep, the shorter sleep latency they currently have. The more parents were annoying when they couldn’t sleep, the poorer sleep efficacy and higher subjective sleep vulnerability students report. Both coming to parents and parental annoying when children couldn’t fall asleep are indirectly related in students to poorer sleep through self-limiting behavior.
Keywords: Parental mediationpsychological sleep regulationsleep-related behaviorstudentssubjective sleep
Introduction
Development of sleep psychology had a long way from earlier studies of behavioral factors if insomnia (Spielman et al., 1987) demonstrated the role of sleep hygiene and sleep-related behavior triggering and perpetuating sleep disturbances to complex psychological models of insomnia including dysfunctional beliefs, hypertrophied attention to sleep, attempts aimed at sleep regulation and self-limitations (Espie et al., 2006; Morin, 1993; Perlis et al., 2011; etc.). Sleep hygiene is considered to be only one of the plenty of psychological and behavioral factors affecting human sleep (Irish et al., 2015) and effectiveness of cognitive behavioral therapy for insomnia supports practical importance of these models (Trauer et al., 2015). Less is known about psychological sleep regulation in people without sleep disturbances although existing data demonstrate that in the case of sleep problems (that are frequent in population) many good sleepers tend to hold dysfunctional beliefs and efforts similar to those perpetuating insomnia (Rasskazova & Tkhostov, 2012). Moreover, experimental provoking in good sleepers of intentions to make himself sleep leads to objective sleep fragmentation (Rasskazova et al., 2014). There is an actual question in this context of how this psychological regulation of sleep is developing in people and what are the factors that makes in so vulnerable to insomnia perpetuation.
Despite the fact that sleep disorders and complaint are extremely frequent during early childhood and in adolescents (Owens, 2008), there are just a few studies on psychological factors of sleep regulation in children and especially – on the role of parental regulation of children’s sleep in further own sleep regulation development. In fact, some studies demonstrate that parental beliefs dysfunctional beliefs about their children’s sleep are related to children’s sleep (Gregory et al., 2009, Ng et al., 2013). It should be also noted that studies of parental beliefs and strategies of children’s sleep mediation is very sensitive to the culture so there is a clear need in taking into account cultural context of the studies of sleep regulation in children (Owens, 2004).
Problem Statement
Based on the psychological model of body functions regulation (Rasskazova & Tkhostov, 2012), we suggested that psychological sleep regulation in humans is developing during childhood and is affected by mediation strategies that parents use to support child’s sleep-wake cycle.
Research Questions
The aim of the study was to reveal the relationships between parental strategies of mediation of their children’s sleep and later sleep-related behavior and sleep quality in these children when they became adults (students).
Purpose of the Study
We hypothesized that:
1.Regardless of dysfunctional beliefs about sleep, sleep quality time and effectiveness in students is related to mediation strategies that their parents used in their childhood to control their sleep-wake cycle. In particular, control over time of going to sleep would be related to better sleep while parental annoying when child cannot fall asleep is related to poorer sleep in students after years.
2.Students’ own sleep related behavior (sleep hygiene, self-limiting behavior after bed nights, medication and non-medication intake during poor nights) mediate the relationship between parental sleep regulation strategies and students’ sleep after years.
Research Methods
Sample
103 pairs of psychology faculty students without diagnosed sleep disturbances and one of their parents (we asked to participate a parent who controlled the student’s sleep in his / her childhood) participated in the study. 90 (84.9%) were females and the age of students varied 17-33 years old (mean age 22.11±3.11 years old). 95 of parents were mothers (89.6%). The age of parents varied 42-66 years old (mean age 50.61±5.84 years old).
Methods
Students were interviewed about their typical pattern of sleep: time when going to sleep, sleep latency, number and length of awakenings during night, time of awake in the morning and length of staying in the bed after wake. Based on this data we calculated their typical total time in bed, sleep time and sleep efficacy.
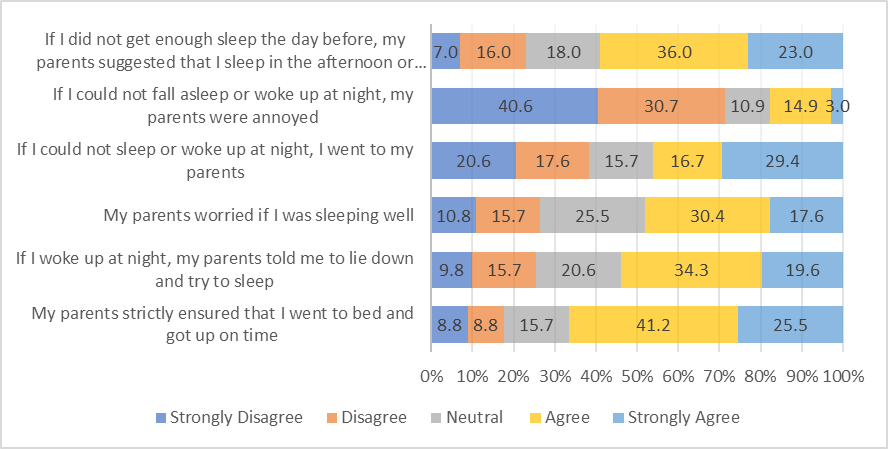
Based on existing studies of parental sleep regulation we created six items measuring parental involvement and active regulation of their child’s sleep (“My parents strictly ensured that I went to bed and got up on time”, “If I woke up at night, my parents told me to lie down and try to sleep”, “My parents worried if I was sleeping well”, “If I could not sleep or woke up at night, I went to my parents”, “If I could not fall asleep or woke up at night, my parents were annoyed”, “If I did not get enough sleep the day before, my parents suggested that I sleep in the afternoon or go to bed earlier”). Items were assessed by 1-5 point Likert scale.
Both students and one of their parents filled Insomnia Severity Index, Dysfunctional Beliefs About Sleep Scale (Morin, 1993) and Subjective Sleep Vulnerability Scale (Rasskazova & Tkhostov, 2012). Students also filled Epworth Sleepiness Scale (Johns, 1991). Insomnia Severity Index and Epworth Sleepiness Scale are screening instruments measuring subjective sleep quality and subjective sleepiness, respectively. Dysfunctional Beliefs About Sleep Scale is a brief measure of cognitive beliefs about sleep and it’s disturbances that could lead to insomnia perpetuation. Subjective Sleep Vulnerability Scale includes 12 different reasons of sleep disturbances (for instance, “Stress”, “Breath disturbances”, “Noise”). Participants are asked to appraise using 1-4 Likert scale to what extent their sleep is disturbed by these factors. Total score by the scale reflect cognitive beliefs about general stability versus vulnerability of sleep to different factors (Cronbach’s alpha .72).
Additionally, in 50 pairs from the initial sample (who didn’t differ from the others by age and gender) students and parents filled Scale of Behavioral Factors of Sleep Disturbances (Rasskazova, 2019) – screening measure for typical behavioral factors of sleep disturbances and perpetuation including Taking Medications and Non-Medications when cannot fall asleep or awake at night, Evening Sleep Hygiene Disturbance (alcohol or tonic drinks consumption, physical training in the evenings, using gadgets at night or too late, delayed bedtime), Self-Limiting Behavior after bad nights (including cancelling morning or daytime responsibilities, sleeping or resting during the day more than usually).
Data were processed in SPSS Statistics 23.0.
Findings
Strategies of parental regulation of their child’s sleep
As shown in Figure
None of the strategies were related to child’s gender or parental age.
Strategies of parental regulation and child’s sleep in adulthood
Strategies of parental regulation were not related to their adult children’s sleep quality, sleep time, sleepiness and dysfunctional beliefs about sleep. However, parental annoying as a reaction to child’s sleep problems was related to poorer sleep efficacy, perception of own sleep as more vulnerable to different factors and higher self-limiting behavior. On the contrary, parental worries and child’s referral to parents in the case of sleep problems correlated to shorter sleep latency in adulthood and – for parental worries – to earlier time when go to bed (table
Parental control over time of their child’s sleep was related to lower probability of use of substances (medications or non-medications) in their adult children to make themselves sleep.
Series of mediation analyses were completed to check for possible indirect effects of parental sleep mediation strategies on their adult children’s sleep. First, we examined the hypothesis that parental control for bedtime is indirectly related to later children’s sleep through less medication and non-medication that they take before sleep. Indeed, we found indirect (but not direct) effect (β=-.10, se=.05, 95% CI [-.20 - -.01]).
Second, it was hypothesized that parental worries about children’s sleep are indirectly related to their children’s sleep when they are youth through their better evening sleep hygiene. However, we found neither direct nor indirect effects in this mediation analysis.
Third, it is possible that going to parents when awake at night or parents annoying when children cannot fall asleep could be indirectly related to students’ sleep through higher self-limiting behavior in these students. Both children coming to parents at night and parental annoying indirectly predicted students poor sleep through higher self-limiting behavior (β=.11, se=.05, 95% CI [.02 - .21] for children coming to parents and β=.13, se=.06, 95% CI [.02 - .28] for parental annoying).
Conclusion
Although there was a long period of time between childhood and becoming university students, retrospective data supports that parental sleep regulation strategies in the past could be related to current students sleep both directly and indirectly.
In particular, parental control for bedtime when students were children is related to less current students’ medication and non-medication intake during poor sleep and has an indirect effect on students’ current sleep through this sleep-related behavior. We could hypothesize that better parental control leads to better sleep-wake cycle that could be a buffer factor in sleep disturbances perpetuations and attempts to regulate sleep by any substances.
The more parents worried about their sleep when they were children, the better evening sleep hygiene students demonstrate. They also go to bed earlier and have shorter sleep latency if their parents worried about their sleep when they were children. The more students in their childhood went to their parents if they couldn’t asleep, the shorter sleep latency they currently have. The more parents were annoying when they couldn’t sleep, the poorer sleep efficacy and higher subjective sleep vulnerability students report. However, both coming to parents and parental annoying when children couldn’t fall asleep are related in students to current self-limiting behavior after bad nights and are indirectly (mediated by self-limiting behavior) related to poorer sleep. In general, we suggest that parental negative emotional reaction to child’s difficulties to fall asleep could be the factor of poorer sleep both by negative expectations about sleep that children have (directly) and attempts to have some rest and to have less responsibilities after bad night. Metaphorically said, the bad night might mean for these people “stressful” night and they try to have rest after it. On the contrary, parental attention and support could be positive direct factor leading to positive expectations about sleep. However, when child comes to parents at night it seems also to support his or her self-limiting behavior and thus could negatively affect sleep as well.
The major limitation of the study is its retrospective design. Further studies on “parents – children” and “parents – adolescents” pairs could provide more detailed picture of psychological sleep regulation development.
Acknowledgments
Research is supported by the Russian Foundation for Basic Research, project No. 20-013-00740 “Development and disturbances of sleep-wake psychological regulation system: an approach of psychology of bodily functions regulation”.
References
- Espie, C. A., Broomfield, N. M., MacMahon, K. M. A., Macphee, L. M., & Taylor, L. M. (2006). The attention-intention-effort pathway in the development of psychophysiologic insomnia: a theoretical review. Sleep Medicine Review, 10, 215–245. https://doi.org/10.1016/j.smrv.2006.03.002
- Gregory, A.M., Cox, J., Crawford, M.R., Holland, J., & Harvey, A.G., (2009). Dysfunctional beliefs and attitudes about sleep in children. Journal of Sleep Research, 18, 422-426. https://doi: 10.1111/j.1365-2869.2009.00747.x
- Irish, L. A., Kline, C. E., Gunn, H. E., Buysse, D. J., & Hall, M. H. (2015). The role of sleep hygiene in promoting public health: A review of empirical evidence. Sleep Medicine reviews, 22, 23-36. https://doi.org/10.1016/j.smrv.2014.10.001
- Johns, M. W. (1991). A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep, 14, 540–545. https://doi.org/10.1093/sleep/14.6.540
- Morin, C. M. (1993). Insomnia: psychological assessment and management. Guilford Press.
- Ng, A. S., Dodd, H. F., Gamble, A. L., & Hudson, J. L. (2013). The relationship between parent and child dysfunctional beliefs about sleep and child sleep. Journal of Children Family Studies, 22, 827-835. https://doi.org/10.1007/s10826-012-9637-6
- Owens, J. (2004). Sleep in children: Cross‐cultural perspectives. Sleep and Biological Rhythms, 2(3), 165-173.
- Owens, J. (2008). Classification and Epidemiology of Childhood Sleep Disorders. Primary Care, 35(3), 533-546. https://doi.org/10.1016/j.pop.2008.06.003
- Perlis, M., Shaw, P.J., Cano, G., & Espie, C.A. (2011). Models of insomnia. In M. Kryger, T. Ross & W. Dement (Eds.), Principles and Practice of Sleep Medicine (pp. 850–865). Elsevier Saunders.
- Rasskazova, E. (2019). Ispol'zovanie elektronnykh gadzhetov vecherom i noch'yu kak povedencheskii faktor zhalob na narusheniya sna [Use of electronic gadgets in the evenings and nights as behavioral factor of sleep complaints]. S.S. Korsakov Journal of Neurology and Psychiatry, 119(4), 36-43. (In Russian, abstr. in English).
- Rasskazova, E. I., & Tkhostov, A. Sh. (2012). Klinicheskaya psikhologiya sna i ego narushenii [Clinical psychology of sleep and sleep disturbances]. Smysl. (In Russ.).
- Rasskazova, E., Zavalko, I., Tkhostov, A., & Dorokhov, V. (2014). High intention to fall asleep causes sleep fragmentation. Journal of Sleep Research, 23(3), 295-301. https://doi.org/10.1111/jsr.12120
- Spielman, A., Caruso, L., & Glovinsky, P. (1987). A behavioral perspective on insomnia treatment. Psychiatric Clinic of North America, 10, 541–553. https://doi.org/10.1016/s0193-953x(18)30532-x
- Trauer, J. M., Qian, M. Y., Doyle, J. S., Rajaratnam, S. M., & Cunnington, D. (2015). Cognitive Behavioral Therapy for Chronic Insomnia: A Systematic Review and Meta-analysis. Annual Internal Medicine, 163(3), 191-204. https://doi.org/10.7326/M14-2841
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
15 November 2020
Article Doi
eBook ISBN
978-1-80296-093-8
Publisher
European Publisher
Volume
94
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-890
Subjects
Psychology, personality, virtual, personality psychology, identity, virtual identity, digital space
Cite this article as:
Rasskazova, E. (2020). Development Of Sleep Regulation In The Childhood: The Role Of Parental Mediation. In T. Martsinkovskaya, & V. Orestova (Eds.), Psychology of Personality: Real and Virtual Context, vol 94. European Proceedings of Social and Behavioural Sciences (pp. 646-652). European Publisher. https://doi.org/10.15405/epsbs.2020.11.02.79