
Scale Of Risk Behaviors, Associated With STI / HIV-AIDS, For Young Chileans


Abstract
STIs and HIV/AIDS are major public health problems. Both pathologies share risk from sexual behaviours, mainly inappropriate use of condoms, multiplicity of sexual partners and sex under the influence of alcohol and drugs, as main vectors. Despite the importance of evaluating these behaviours for preventive purposes in the Hispanic-American context, there are no tools with sufficient evidence of reliability and validity for this purpose. The present study reports the development of a free access instrument for this purpose, according to current psychometric standards. A total of 866 young people living in the cities of Arica and Iquique (northern Chile) were selected on time-space and social network sampling. The final instrument consists of 16 items, distributed in four dimensions: sexual activity with multiple partners; inadequate and/or insufficient use of protective barriers; sexual activity under the influence of alcohol and/or drugs; and perceived knowledge of the partner's sexual history. The instrument offers adequate evidence of reliability (ω > .8) and validity based on the internal structure of the test (RMSEA < .06; CFI > .95; TLI > .95). In addition, we offer differentiated scales by sex, discuss the possible uses of the instrument and suggest new courses of research.
Keywords: Alcohol drinkingHIV/AIDSinternetsexual behaviourSTI
Introduction
Sexually transmitted infections (STIs) and the human immunodeficiency virus, including its active manifestation, acquired immunodeficiency syndrome (HIV/AIDS), are health problems that affect millions of people in the world, with physical consequences such as infertility, acute disability and even death (World Health Organization, 2008); and psychological consequences such as depression, adaptive disorders, social isolation (Davis, 2004), a questioning of one's future (Edo & Ballester, 2006) and social damage associated with stigmatisation and discrimination (Harding & Molloy, 2008).
Due to the magnitude of these problems, enormous public-private efforts have been made to contain and reduce STIs or HIV/AIDS. However, the World Health Organization has estimated that, each day, more than one million people contract an STI and more than 30 million live with HIV/AIDS (UNAIDS, 2008). This, together with an estimate of growth for STIs of 11.3% between 2005 and 2008, and of 5.43% in HIV between 2013 and 2014 (UNAIDS, 2014), shows that these pathologies persist as one of the main worldwide public health problems (Ballester, Gil, Giménez, & Ruiz, 2009).
In Chile, the rate of confirmed cases of HIV/AIDS has increased consistently since the year of the first notification (1984), with an accumulated total of 36,820 cases diagnosed as of 2015 (Departamento de Epidemiología., & División de Planificación Sanitaria Ministerio de Salud de Chile, 2015). Notifiable STIs (syphilis and gonorrhoea), after a continuous decline from 1981 to 2007, have shown a slight and relatively stable increase as of 2014, in which year 5,806 new cases were diagnosed (Department of Epidemiology & Division of Health Planning Ministry of Health of Chile, 2015). Both STIs and HIV/AIDS are concentrated, proportionally and mostly, in urban districts of the country (Ministerio de Salud de Chile, 2010). Its regional distribution is heterogeneous, observing that the three regions that make up the North of Chile (i.e. composed by administrative regions of Arica y Parinacota, Tarapacá and Antofagasta) are within the five regions with the highest rates of HIV/AIDS and STIs over the last three five-year periods with available data (1998–2012). The difference with respect to the reality of the country is remarkable; for example, the rates of new HIV/AIDS notifications (2008–2012) in Arica and Parinacota (70.3/100,000 inhabitants) and Tarapacá (38.5/100,000 inhabitants), were respectively 2.6 and 1.6 times higher than the national rate (24.7/100,000 population) (Departamento de Epidemiología y División de Planificación Sanitaria Ministerio de Salud de Chile, 2015).
STIs or HIV/AIDS are concentrated in young people more than in any other sexually active age group (Cates, 1990), with the highest prevalence among young people between 18 and 35 years old (UNAIDS, 2013), who have a higher frequency of sexual behaviours that contain risk of contagion of STIs or HIV/AIDS (Kotchink, Shaffer, & Forehand, 2001). Therefore, this group concentrates the epidemiological search in the evaluation of risky sexual behaviours (Minnis & Padian, 2001).
Problem Statement
STIs or HIV/AIDS can be contracted in many ways, although the main route of transmission is direct sexual contact (e.g. vaginal, anal or oral sex) with carriers and without the proper use of protective barriers (World Health Organization, 2007). Sexual risk behaviours (SRBs) are behaviours that increase the possibility of obtaining unwanted consequences of sexual activity (Ezzati, Lopez, Alan, Rodgers, & Murray, 2004), mainly the acquisition of HIV/AIDS, STIs and unwanted pregnancies (Spencer, Doull, & Shoveller, 2014). SRB can be differentiated according to the behavioural closeness with the risk, distinguishing: 1) proximal sexual risk behaviours (PSRBs), i.e. behaviours that directly increase the possibility of contact with fluids of carriers; and 2) distal sexual risk behaviours (DSRBs), i.e. those that indirectly increase the possibility of SRBs.
In the literature, two kinds of PSRBs are mentioned: a) inadequate or insufficient use of protection barriers (IUPB), i.e. absence or misuse of barriers (particularly condoms) that reduce the possibility of contact with flows of genitalia or vectors of STIs or HIV/AIDS (UNAIDS, 2014), with the condom being the only effective barrier for the pathogens causing STIs and HIV (Joint United Nations Programme on HIV/AIDS., United Nations Population Fund., & World Health Organization, 2015); and b) sexual activity with multiple partners (SAMP), referring to sexual encounters with more than one active sexual partner in parallel or simultaneously (Ramseyer, Brandon-Friedman, & Ely, 2016), increasing the probability of contracting STIs (Irala, 2012) and HIV/AIDS (UNAIDS, 2014). On the other hand, two DSRBs have been considered: a) sexual activity under the influence of alcohol or drugs (SAUIAD), defined as the use of substances that alter cognitive functioning, contingent on a sexual act (LaBrie, Grant, & Hummer, 2011); and b) perceived knowledge of the sexual history of the couple (PKSHC), referring to the perception of sexual history knowledge, past or present, of the sexual partner(s) that would affect the decision to have sexual activity with or without a condom (Lescano, Vazquez, Brown, Litvin, & Pugatch, 2006).
Purpose of the Study
Because identifying PSRBS and DSRBs is relevant to developing and evaluating preventive programs (Salvo, 2011), in the international context, some measurement instruments have been developed that have evidence of reliability and validity (Hendrick, Hendrick, & Reich, 2006; Vinaccia et al., 2007). However, these instruments do not have free access or official translations, and, most importantly, none of them has been adapted for the Chilean context, for which, in a broad review, no instrument for this purpose was found with evidence that guarantees an adequate interpretation of their scores.
Therefore, this work aimed to develop an instrument to assess sexual behaviours at risk of STI or HIV/AIDS infection in Chilean youth and young adults, providing evidence of reliability and validity that supports the adequacy of interpretations of the observed scores and, therefore, delivers minimum ethical guarantees to support the conclusions and decisions that derive from the measurement process (American Educational Research Association, American Psychological Association & National Council on Measurement in Education, 2014).
Research Methods
Design and participants
The study was cross-sectional and instrumental. Due to the difficulties in obtaining a probabilistic sample, two non-probabilistic samplings were used together: a) Social network samplings, which have proven useful in capturing samplings that require high confidentiality (Baltar & Brunet, 2012); and b) time-space samplings, which have proven useful in HIV/AIDS studies (Semaan, Lauby, & Liebman, 2002).
The initial social network sample, for the pilot debugging, was composed of 243 young people, excluding 8 for having failed control items, being finally made up of 30.6% (n = 72) men and 69.4% (n = 163) women, with an average age of 25.01 (SD = 5.72) years. The sample for the final evaluation of the scale was made up of 623 participants, of which 403 correspond to time-space sampling in public universities in the cities of Arica (n = 199) and Iquique (n = 204), and 220 correspond to a social network sample, after discarding 43 for having failed some control item, being made up of 580 participants, of which 56.4% correspond to women (n = 327), with an average age of 22.22 (SD = 2.96) years in Sample b.
Instrument
The self-created questionnaire, whose final version consists of 16 items, was designed to assess four dimensions of risky sexual behaviour: a) sexual activity with multiple partners (items = 4); b) inadequate or insufficient use of protection barriers (items = 4); c) sexual activity under the influence of alcohol or drugs (items = 4); and d) the couple’s knowledge of each other’ sexual history (items = 4). Dimensions a and b correspond to PSRBs and dimensions c and d to DSRBs. The questions are behavioural/attitudinal statements on a Likert-type scale of 4 points (0 "never" – 3 "always"), conditioning to report only the behaviour of the past two years. Additionally, the questionnaire included 4 items that rate attention (4 items), in order to control some possible measurement errors, associated with patterns of aberrant responses (e.g. acquiescence, automatic responses or reading comprehension).
Procedure
Since the study was a theoretical review, a total of 101 items were drafted, which were refined in writing and content by expert judges (3 psychometricians and 3 health professionals), discarding a total of 54 items (i.e. 47 items remaining). An online pilot application (n = 104) was carried out, voluntarily and anonymously, with which depuration based on internal consistency were carried out; subsequently, 28 items were conserved, which were disseminated via social networks, collecting a total of 243 questionnaires answered voluntarily and anonymously, from the web platform google forms, which resulted in a version of 26 items; this version was applied in a time-space sampling in public universities in the cities of Arica and Iquique, in which the questionnaire was provided in an envelope that included an informed consent form, a statement of the objectives of research, a declaration of the rights of the participant and the commitment of anonymity, to be returned sealed and without the possibility of identification. Finally, a second social network sampling was carried out with the 26-item version of the questionnaire.
Both the instrument and the entire procedure was known and approved by an institutional ethics committee.
Statistic analysis
First, with Sample a, the measurement models were cleaned by eliminating items with intradimensional redundancies or slight factorial saturations (λ < .3), based on a confirmatory factorial analysis. Said analysis was carried out following the recommendations of various authors on factorial treatment of ordinal variables (Garrido, Abad, & Ponsoda, 2011), from the matrix of polychoric variables and using the robust weighted least squares (WLSMV) estimation method, which is robust with non-normal discrete variables (Asparouhouv & Muthén, 2007).
Subsequently, with the reduced instrument (26 items) a second depuration was carried out with Sample b using an exploratory structural equation model (ESEM) with TARGET rotation (matrix of polychoric variables and WLSMV estimation method), which allows for performance of confirmatory models without crossed saturation restrictions and identification of the multidimensionality of the items (Marsh et al., 2009). Finally, with the final model refined, a confirmatory factorial analysis (matrix of polychoric variables and WLSMV estimation method) was performed, including invariance tests by biological sex, as well as comparisons of means by biological sex and calculations of different scales for men and women (see Annex 3 in https://1drv.ms/b/s!Au5ZByp1rtTjiaY-2083G6PmIPfe7g).
All analyses were performed with the IBM SPSS Statistics (21) and MPLUS (7.4) programs.
Findings
Table
With Sample b, an ESEM analysis was carried out, identifying and eliminating those items whose cross-saturations were significantly different from 0, leaving 16 items in the final version. The fit of the final ESEM and SEM models (Table
Estimates of factor saturations, based on the ESEM model, and dimensional reliability, using the omega and Cronbach’s alpha coefficients, are presented in Table
Note:
**
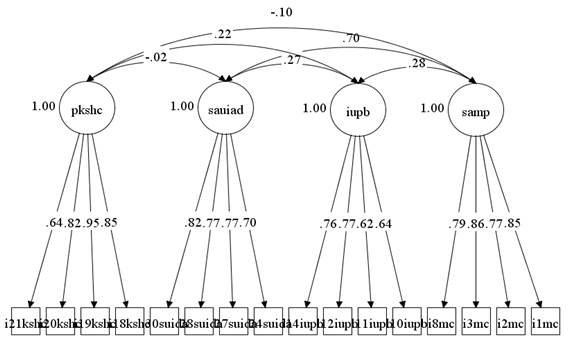
As regards the structural relationships represented in Figure
Finally, due to possible differences in the model by biological sex, and to check the need for differential scales, tests of metric and structural invariance were performed, rejecting the hypothesis of invariance in both scenarios (p_Δχ2 < .05); and mean comparisons between the observed scores, rejecting the assumptions of equality of mean for the IUPB dimensions (t_ (GL = 578) = 1.72, p < .01), SAMP (t_ (GL = 523.82) = 4.58, p <. 01) and PKSHC (t_ (GL = 560.87) = - 3.16; p <.01). Due to the differences observed, differential scales are offered by risk quintiles (see Annex 1 in https://1drv.ms/b/s!Au5ZByp1rtTjiaY-2083G6PmIPfe7g).
Conclusion
The current state of the instrument provides evidence of adequate levels of reliability and validity, based on the internal structure of the test, sufficient to support the use of the scale and the interpretation of the scores in populations equivalent to the study sample, mostly upper-level Chilean students, that have initiated some type of sexual activity.
Additionally, there is a close relationship between both DSRBs (i.e. sexual activity with multiple partners and inadequate or inadequate use of protective barriers) with the PSRBs (i.e. sexual activity dimension under the influence of alcohol or drugs and perceived knowledge of the sexual history of the couple).
Although the analysis of the relationships between the dimensions was not in itself an objective of the investigation, it is worth highlighting the observation of a dangerous triad, since, as expected according to the literature, sexual activity under the influence of alcohol or drugs increases PSRBs and, contrary to what might be expected, sexual activity with multiple partners increases the inadequate or insufficient use of protection barriers, exerting a multiplying effect of the risk that could be attributable to third variables (e.g. control of impulses). This scenario is alarming because those who are more likely to have sex with a carrier also take fewer precautions, maximising the likelihood of having direct contact with infected fluids.
In relation to the comparison by biological sex, significant differences were evidenced between the CSR, as indicated by the existing literature, which is why the respective scales were generated.
Considering all the above, the use of this instrument, in an equivalent population, in health, medical and educational contexts, with the objective of knowing the SRBs for risk diagnosis and the ex-post evaluation of preventive programs, is appropriate and recommended.
The main limitation of the study corresponds to the type of sampling used, which makes it pertinent that the instrument be subjected to new psychometric studies to increase the capacity of its viability, mainly in higher-risk populations. Additionally, it is suggested to use this instrument in conjunction with STI or HIV/AIDS medical exams, to verify the predictive power of the CSRs on these diseases.
Acknowledgments
R.F. acknowledges partial support from FONDECYT through grant FONDECYT INICIACIÓN N°11170395 and from UNIVERSIDAD DE TARAPACÁ through grant PROYECTO DE INVESTIGACIÓN MAYOR, Nº 3738-16, “Desarrollo de un instrumento psicométrico para evaluar factores de riesgo de ITS y VIH en jóvenes y adultos jóvenes tempranos residentes en el norte de Chile”.
References
- American Educational Research Association., American Psychological Association., & National Council on Measurement in Education (2014). Standards for educational and psychological testing. Washington DC, USA: American Educational Research Association.
- Asparouhouv, T., & Muthén, B. (2007). Wald test of mean equality for potential latent class predictors in mixture modeling. Retrieved from https://www.statmodel.com/download/MeanTest1.pdf
- Ballester, R., Gil, M., Giménez, C., & Ruiz, E. (2009). Actitudes y conductas sexuales de riesgo para la infección por VIH/SIDA en jóvenes españoles. Revista de Psicopatología y Psicología Clinica, 14(3), 181-191.
- Baltar, F., & Brunet, I. (2012). Social research 2.0: virtual snowball sampling method using Facebook. Internet Research, 22(1), 57-74.
- Cates, W. (1990). The epidemiology and control of sexually transmitted diseases in adolescents. Adolescent Medicine: State of the Art Reviews, 1(3), 409-428.
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Retrieved from http://www.utstat.toronto.edu/~brunner/oldclass/378f16/readings/CohenPower.pdf
- Davis, S. (2004). Clinical sequelae affecting quality of life in the HlV-infected patient. Journal of the Association of Nurses in AIDS Care, 15(5), 28-33. https://doi.org/10.1177/1055329004269478
- Departamento de Epidemiología., & División de Planificación Sanitaria Ministerio de Salud de Chile. (2015). Informe Nacional: evolución de la infección por VIH/SIDA Chile 1984-2012. Revista chilena de infectología, 32(1), 17-43. DOI: 10.4067/S0716-10182015000100003
- Departamento de Estadísticas e Información de Salud de Chile. (2014). Serie histórica de enfermedades de notificación obligatoria (ENO) 1950-2014. Retrieved from http://www.deis.cl/estadisticas-eno/
- Edo, M., & Ballester, R. (2006). Estado emocional y conducta de enfermedad en pacientes con VIH/SIDA y enfermos oncológicos. Revista de Psicopatología y Psicología Clínica, 11(2), 79-90.
- Ezzati, M., Lopez, A., Alan, D., Rodgers, A., & Murray, C. (2004). Comparative quantification of health risks: Global and regional burden of disease attributable to selected major risk factors. Retrieved from http://apps.who.int/iris/bitstream/handle/10665/42792/9241580348_eng_Volume1.pdf?1
- Garrido, L., Abad, F., & Ponsoda, V. (2011). Performance of Velicer’s Minimum Average Partial Factor Retention Method with Categorical Variables. Educational and Psychological Measurement, 71(3), 551-570. Available from: http://journals.sagepub.com/doi/abs/10.1177/0013164410389489
- Harding, R., & Molloy, T. (2008). Positive futures? The impact of HIV infection on achieving health, wealth and future planning. Psychological and Socio-medical Aspects of AIDS/HIV, 20(5), 565-570. Available from:
- Hendrick, C., Hendrick, S., & Reich, D. (2006). The Brief Sexual Attitudes Scale. The Journal of Sex Research, 43(1), 76-86. https://doi.org/10.1080/00224490609552301
- Irala, J. (2012). Efectos colaterales de la promiscuidad y de la infidelidad. Retrieved from http://congresomundial.es/wp-content/uploads/Jokin-de-Irala-Efectos-colaterales-de-la-promiscuidad-y-de-la-infidelidad-ESPA%C3%91OL.pdf
- Joint United Nations Programme on HIV/AIDS., United Nations Population Fund., & World Health Organization. (2015). UNFPA, WHO and UNAIDS: Position statement on condoms and the prevention of HIV, other sexually transmitted infections and unintended pregnancy. Retrieved from http://www.unaids.org/es/resources/presscentre/featurestories/2015/july/20150702_condoms_prevention
- Kotchink, B., Shaffer, A., & Forehand, R. (2001). Adolescent sexual risk behavior: a multi-system perspective. Clinical Psychology Review, 21(4), 493-519. https://doi.org/10.1016/S0272-7358(99)00070-7
- LaBrie, J., Grant, S., & Hummer, J. (2011). This would be better drunk: Alcohol expectancies become more positive while drinking in the college social environment. Addictive Behaviors, 36(8), 890-893. https://doi.org/10.1016/j.addbeh.2011.03.015
- Lescano, C., Vazquez, E., Brown, L., Litvin, E., & Pugatch, D. (2006). Condom use with “casual” and “main” partners: What’s in a name? Journal of Adolescent Health, 39(3), 443-443. https://doi.org/10.1016/j.jadohealth.2006.01.003
- Marsh, W., Muthén, B., Asparouhov, T., Lüdtke, O., Robitzsch, A., Morin, A., & Trautwein, U. (2009). Exploratory structural equation modeling, integrating CFA and EFA: Application to students’ evaluations of university teaching. Structural Equation Modeling, 16(3), 439-476.
- Ministerio de salud de Chile. (2010). Estrategia nacional de salud para el cumplimiento de los objetivos sanitarios de la década 2011-2020. Retrieved from http://www.minsal.cl/portal/url/item/c4034eddbc96ca6de0400101640159b8.pdf
- Minnis, A., & Padian, N. (2001). Reliability of Adolescents’ self-reported sexual behavior: a comparison of two diary methodologies. Journal of Adolescent Health, 28(5), 394-403.
- Ponterotto, J., & Ruckdeschel, D. (2007). An overview of coefficient alpha and a reliability matrix for estimating adequacy of internal consistency coefficients with psychological research measures. Perceptual and Motor Skills, 105(3), 997-1014. https://doi.org/10.2466/pms.105.3.997-1014
- Ramseyer, V., Brandon-Friedman, R., & Ely, G. (2016). Sexual health behaviors and outcomes among current and former foster youth: A review of the literature. Children and Youth Services Reviw, 64, 1-14. https://doi.org/10.1016/j.childyouth.2016.02.023
- Salvo, A. (2011). Infecciones de transmisión sexual (ITS) en Chile. Revista Médica Clínica Las Condes, 22(6), 813-824. https://doi.org/10.1016/S0716-8640(11)70494-1
- Schreiber, J., Nora, A., Stage, F., Barlow, E., & King, J. (2006). Reporting structural equation modeling and confirmatory factor analysis results: A review. The Journal of Educational Research, 99(6), 323-338.
- Semaan, S., Lauby, J., & Liebman, J. (2002). Street and network sampling in evaluation studies of HIV risk-reduction interventions. AIDS Reviews, 4(4), 23-213.
- Spencer, G., Doull, M., & Shoveller, J. (2014). Examining the concept of choice in sexual health interventions for young people. Youth & Society, 46(6), 756-778.
- UNAIDS. (2008). Informe sobre la epidemia mundial de sida 2008. Retrieved from http://data.unaids.org/pub/globalreport/2008/jc1510_2008globalreport_es.pdf
- UNAIDS. (2013). El sida en cifras. 2013. Retrieved from http://files.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2013/JC2571_AIDS_by_the_numbers_es.pdf
- UNAIDS. (2014). Hoja informativa 2014: Datos estadísticos mundiales. Retrieved from http://www.unaids.org/sites/default/files/media_asset/20140716_FactSheet_es_0.pdf
- Vinaccia, S., Quiceno, J., Gaviria, A., Soto, A., Gil, M., & Ballester, R. (2007). Conductas sexuales de riesgo para la infección por VIH/Sida en adolescentes colombianos. Terapia psicológica, 25(1), 39-50. DOI: 10.4067/S0718-48082007000100003
- World Health Organization. (2007). Estrategia mundial de prevención y control de las infecciones de transmisión sexual 2006-2015. Retrieved from http://apps.who.int/iris/bitstream/handle/10665/43773/9789243563473_spa.pdf;jsessionid=19881957285EA7DF7B43D65855CE2418?sequence=1
- World Health Organization. (2008). Global incidence and prevalence of selected curable sexually transmitted infections-2008. Retrieved from http://www.who.int/reproductivehealth/publications/rtis/2008_STI_estimates.pdf
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
09 April 2019
Article Doi
eBook ISBN
978-1-80296-059-4
Publisher
Future Academy
Volume
60
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-1062
Subjects
Multicultural education, education, personal health, public health, social discrimination,social inequality
Cite this article as:
Ferrer-Urbina, R., Leal-Soto, F., Bravo, N., Huaranca, C., Perez, J., Salinas, T., & Villegas, N. (2019). Scale Of Risk Behaviors, Associated With STI / HIV-AIDS, For Young Chileans. In E. Soriano, C. Sleeter, M. Antonia Casanova, R. M. Zapata, & V. C. Cala (Eds.), The Value of Education and Health for a Global, Transcultural World, vol 60. European Proceedings of Social and Behavioural Sciences (pp. 800-809). Future Academy. https://doi.org/10.15405/epsbs.2019.04.02.99