
Body Mass Index at Puberty Schoolchildren in Romania, Urban Areas


Abstract
In recent years, the prevalence of overweight increased as a result of complex interactions between genes, dietary intake, physical activity and environment. The aim of this study is to estimate the incidence of overweight of a sample of pupils and if there are significant differences in terms of demographic variables, such as gender and age, as well as body mass index and anthropometric indicators, such as height and weight. In order to obtain data on the overweight, anthropometric indicators, such as height and weight, were measured and the body mass index (BMI) was calculated, to a total of 261 schoolchildren, between 12 and 15 years. An ANOVA 2 (gender) x 2 (age) was performed to determine if there are significant differences between the dependent variable (Body Mass Index) and the independent variables. The results show significant differences in body mass index according to the age (F(3,254) = 5.35; p < 0.05; R2 = .059) and the gender (F(3, 254) = 4.19; p < 0.05; R2 = .047) of the schoolchildren. A very strong positive relationship between BMI and weight, according to the gender, was found and a high direct correlation between height and weight, according to the gender, was found, too. No relationships are found between body mass index according to the age of the measured schoolchildren. Measured anthropometric indicators show significant increases. A high percentage of overweight schoolchildren, are obese. WHO recognizes that overweight, in childhood and adolescence, represents a major problem for industrialized countries.
Keywords: Overweightschoolchildrenanthropometric indicatorsbody mass index
Introduction
The physical body growth is expressed by an increase of height and its development can be
defined in terms of the human organism’s functionality and abilities enhancement. These processes
depend on genetic, nutritional, environmental factors. Physical growth consists in reaching the height and
weight optimum values for the considered age group as well as the dimensional growth of all the organs
and systems (Beers, 2009, p 2248).
In general, the body height at the age of 5 represents 60% of the final height, at 10 years 75%, at
15 90%, and at 20 it represents 99% of the final body height(Ranga, 1990, Beers, 2009). Organism
maturation is a process which occurs earlier in girls than in boys. The growth rate in girls is 12.1±0.9
years in contrast to 14.1±0.9 years in boys [Beers, 2009, p 2248].
Until the age of 10, the differences between girls and boys are insignificant, the girls’ height and
weight being slightly less than those of the boys, with differences ranging between 1.5 and 0.5 cm.
Between 11 and 15 years of age, the girls’ height exceeds the boys’ height. At the age of 12, girls exceed
boys in weight. In boys, puberty starts at 12 years of age; these will exceed girls in height at 15 and in
weight after 16 years of age.
In boys, physical growth during puberty is a lengthy process involving deeper changes of the body
and limbs proportions. These changes occur in both genders and are part of the sexual maturation process.
Height growth occurs 1½ years earlier than weight growth. While between 13 and 14 girls weigh
more than boys of the same age, at 14 – 15 years of age these differences become insignificant. At the age
of 16 the boys exceed girls in height and weight at a higher rate due to puberty growth spurt as well as
due to the longer period of adolescence growth (Beers, 2006, p 2248). The staturo-ponderal growth also
involves changes of body proportions, a process which will eventually lead to adult body configuration.
It was found that, beginning with 11 – 12 years up to 15 years of age, girls exceed boys in weight,
and beginning with 11 years also in height. „C. H. Strantz maintains that girls reach half of their total
weight at 11 while boys reach half of their weight at the age of 13 years (Ranga, 1990, p.395)”. Between
6 – 10 years of age in girls and 6 – 12 years of age in boys the weight increase is around 3 – 3.5 kg, with
significant individual variations during puberty and adolescence.
Materials and Methods
This study was conducted between April and June 2014 at the General School No 30 of Braşov.
The study has been approved by the Ethics Commission of the Transilvania University of Brașov. Also,
the research on human subjects obtained the informed consent agreement of the participating subjects and
of their parents. Participation in this study was voluntary and the anonymity of the participants was
ensured.
The study comprised a number of 261 gymnasium-cycle schoolchildren of which 132 were girls
and 129 boys with ages between 12 and 15 years.
In order to emphasize the organism growth and development rate in 12 – 15 year-old children
measurements on the anthropometric indicators height and weight were conducted. The height was
measured using a stadiometer, and was expressed in centimetres (cm) whereas weight was determined
using digital scales and was expressed in kilograms (kg). The measurements were conducted in class
rooms provided by the school governance authority with the support of the teachers. The ratio of the two
indicators, height and weight, was interpreted using the Body Mass Index.
In order to find out whether there are significant differences between the dependent variables
(Body Mass Index) and the independent variables (age and gender), the ANOVA 2 test was conducted
(gender) x 2 (age), the T Student test was used to emphasize the difference between the two independent
samples, and a possible correlation between variables was examined using the Pearson coefficient.
Result interpretation, Tables, and graphs were completed using Microsoft Office Excel 2010.
Results
The relationship between the two anthropometric indicators, height and weight, provides important
information for evaluating the growth and development level of individuals. If analyzed separately, the
data regarding the height indicator appear conclusive for the evaluation of growth and development, since
body weight is affected by nutrition and the living conditions of each individual.
By evaluating weight, height and BMI in relationship with age and gender of the children
comprised in the study, it was found that these parameters increase with age.
The BMI (Body Mass Index) is the ratio between an individual’s weight in kilograms and the
square of his height in metres.
According to CDC, in children with ages between 2 and 19, the BMI is expressed as percentile,
depending on age and gender: obesity - BMI > percentile 95, overweight - BMI > percentile 85 and
percentile 95 and underweight - BMI < percentile 5.
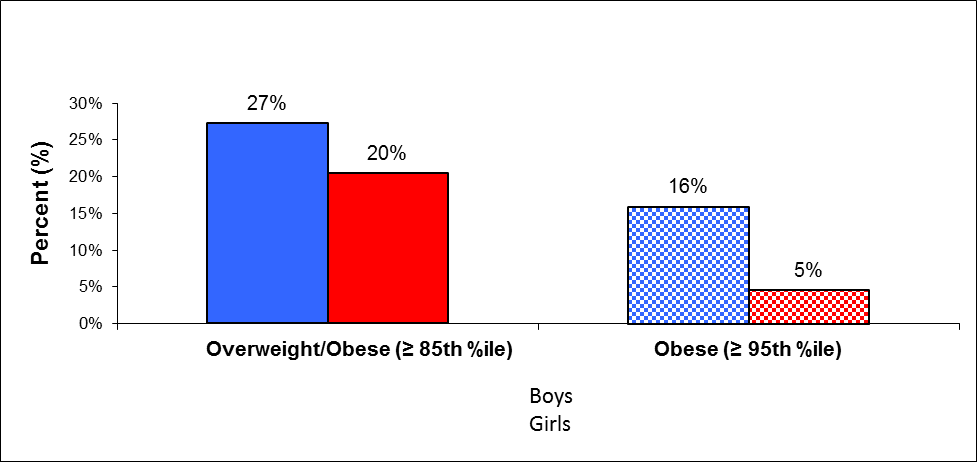
After comparing the data collected from the 12-year-old girls with the boys’ data, it can be observed that the proportion of the boys with excess weight exceeds by 7% the girls’ proportion. Obesity is more frequent in boys than in girls (16% in boys, in contrast with 5% girls) (Figure
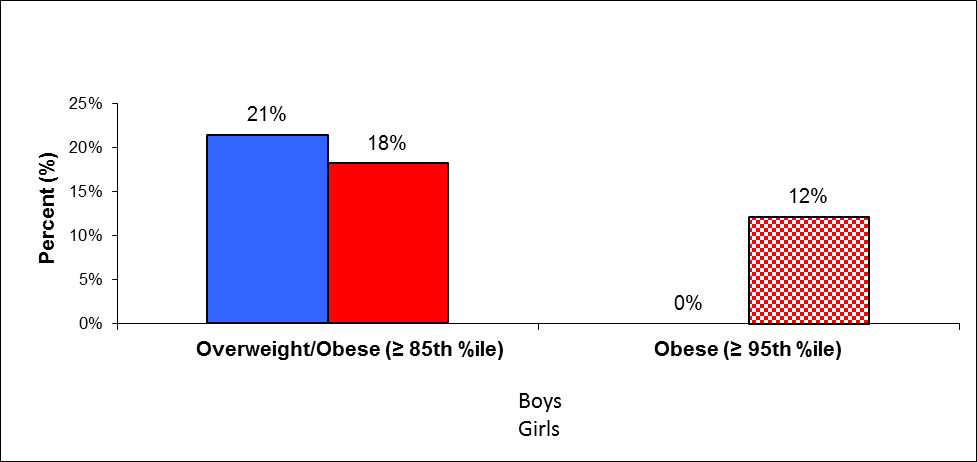
The data collected from 13-year-old boys show that 21% of the boys have excess weight, while 12% of the girls have a BMI ≥ 95th %ile. This situation indicates that a relatively high percentage of the 13-year-old boys have excess weight and 2/3 of the girls with excess weight are obese (Figure
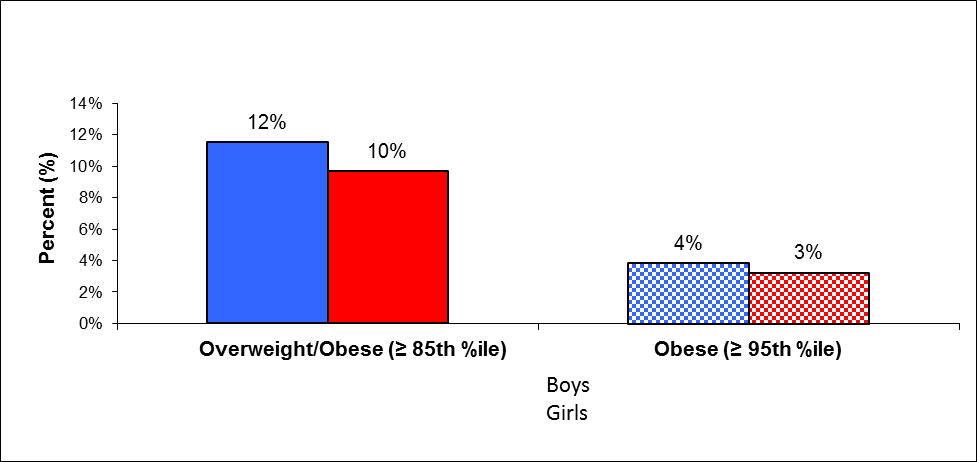
By comparatively analysing the data collected from 14-year-old girls with the boys’ data no significant differences were observed in overweight subjects. The values are 10%, in girls, and, respectively 12% in boys. Also, there are no significant differences for those with a BMI ≥ 95th %ile, 3% in girls and 4% in boys (Figure
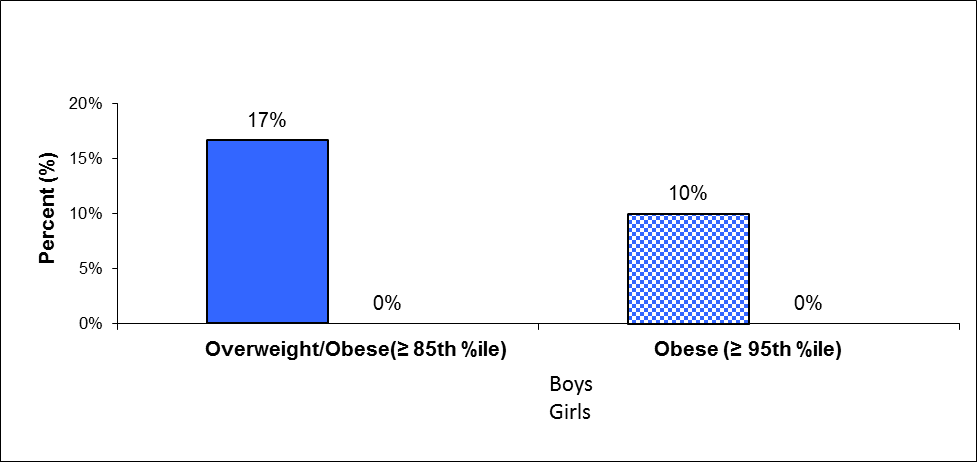
The data collected from 15-year-old boys indicate that 17% of the boys are overweight, 10% of
these having a BMI ≥ 95th %ile. By comparatively analysing the collected data, it could be ascertained
that the 15-year-old girls from the measured sample are not overweight, having a normal BMI, whereas a significant percentage of the measured boys are overweight and/or obese (Figure
From the measured girls, 59.09% of the 12-year-old, 63.64% of the 13-year-old, and 54.84% of
the 14-year-old have a BMI lower than the average age-specific value, while 58.33% of the 15-year-old
ones have a BMI above the age-specific average. The variability coefficient indicates an average sample
homogeneity, taking values between 10.01 and 20.28%, depending on age. The average values are still
representative (Table
From the measured boys, 54.55%% of the 12-year-old, 60.71% of the 13-year-old, 53.85% of the
14-year-old, and 61.29% of the 15-year-old have a BMI under the age-specific average. The measured
sample has an average homogeneity. The variability coefficient takes values between 15.69 and 23.73%,
depending on age. The average values are still representative (Table
The obtained results show significant differences of the Body Mass Index depending on age
(F(3,254) = 5.35; p < 0.05; ƞ2 = .059) and gender (F(3, 254) = 4.19; p < 0.05; ƞ2 = .047). This indicates that the percentage of boys (Ma = 8.25; SD = 5.44), with excess weight is higher than the girls’ (Ma = 5.75; SD = 5.62) (Figures
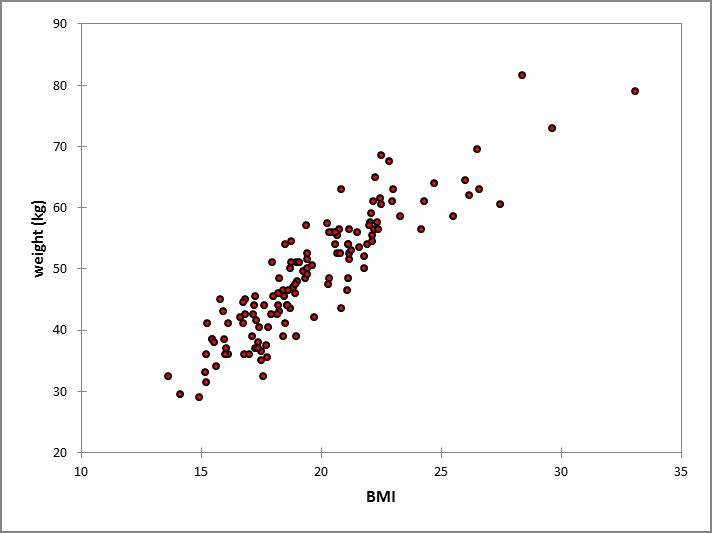
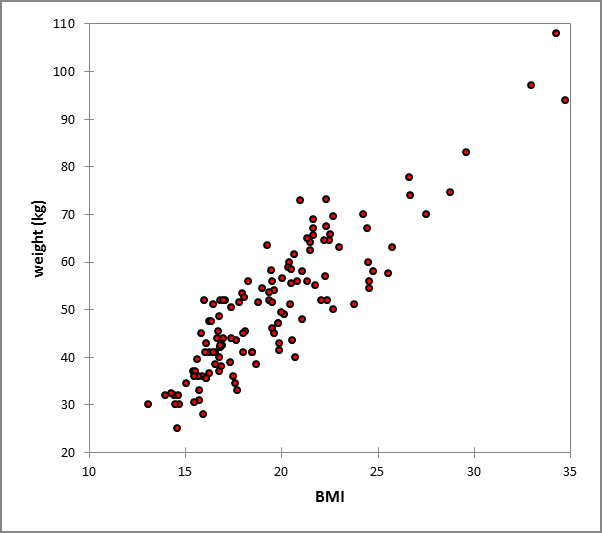
By evaluating the relationship between BMI and weight depending on gender, a direct, very high
correlation has resulted, girls (r = .90, p < 0.0001, R2 = .81) (Figure
= .78) (Figure
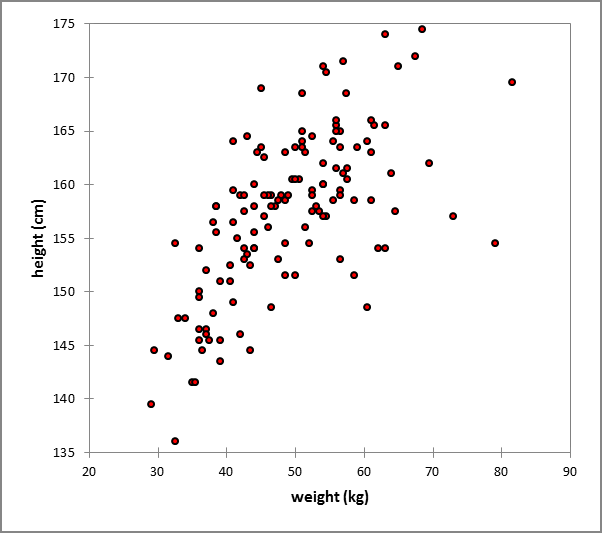
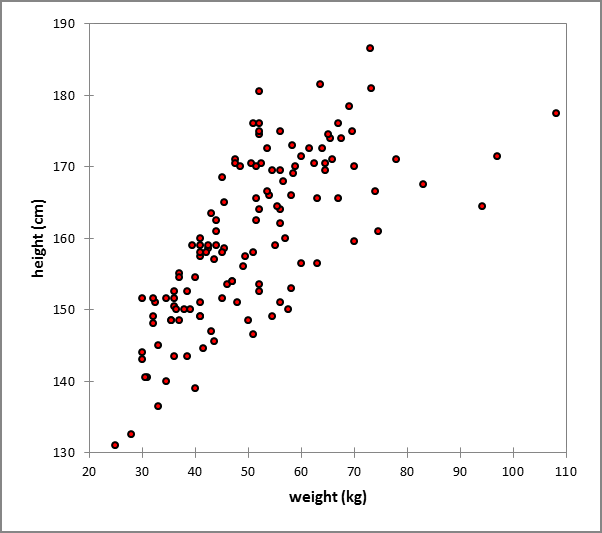
A high, direct correlation was identified between height and weight depending on gender, girls (r
= .65, p < 0.0001, R2 = .42) (Figure
Between BMI and the height of the measured subjects was identified a direct, weak correlation,
boys (r = .31, p < 0.001, R2 = .098), and, respectively girls (r = .26, p < 0.05, R2 = .066). No correlation
was identified between BMI and the age of the measured schoolchildren.
Discussions
Literature as well as the studies conducted in this field have signalled a doubling of worldwide
obesity prevalence in children populations over the last 30 years in both the developed, highly
industrialized world as well as the developing countries (Wang, 2006). According to a study conducted
across 79 countries, the WHO estimates a number of 250 million obese persons worldwide, of which 22
million are under-5 children emphasizing the idea that 50% of the obese children will become obese
adults (Barlow, 2007).
A number of studies are dealing with childhood obesity trends in Europe. These trends vary with
time, depending on age, gender, and geographic area, the highest prevalence levels being observed in
southern European countries. A recent study showed that 36% of the 9-year-old children across mainland
Italy and Sicily were found to be overweight or obese (by IOTF criteria) (Perra et al., 2002). In Greece,
the prevalence was 26% in boys and 19% in girls aged 6-17 (by IOTF criteria) (Krassas et al., 2001). In
Spain, 27% of the children and adolescents were found to be overweight or obese (by IOTF criteria)
(Majem et al., 2001), while data acquired from Crete showed that 39% of the children aged 12 were
overweight or obese (by IOTF criteria) (Manios et al., 2002). Northern European countries showed lower
overweight or obesity prevalence rates: e.g. in the UK, around 20% of the children were found to be
overweight or obese, in 1998 (Lobstein, James and Cole, 2003). In Sweden, the prevalence rate was 18%
in 10-year-old children (Kautiainen, 2002).
According to an IASO estimate, at present, 10% of the children worldwide are overweight, i.e.
around 120 de million children. The WHO warns that, in 2009, obesity was more prevalent than under-
nutrition, 15-18% of the children worldwide being overweight.
According to a study conducted across 79 countries, the WHO estimates a number of 250 million
obese persons worldwide, of which around 22 million are under-5 children.
The prevalence of excess weight in children showed alarmingly high growth rates across North
America, Europe, and recently also in Australia, China, South America, and Northern Africa. This
phenomenon varies among different regions and countries from <5% in Africa and some parts of Asia, to
>20% in Europe and >30% in America and some countries in the Middle East (Lobstein, 2003).
According to the data provided by NHANES, over the last 30 years, the prevalence of obesity has
tripled: in children aged 6-11, from 6,5% in 1980, to 19,6% in 2008, in adolescents aged 12-19, from 5%
to 18,1%, and in preschoolers aged 2-5, from 5% in 1980, to 10,4% in 2008.
In Europe, childhood obesity tripled over the last 20 years (European Commission 2007). In most
Western Europe countries obesity rates are 10-25%, in contrast to Eastern Europe and the Mediterranean
countries which show much higher rates in women, of up to 40% 9 (Popa, 2001). In Northern European
countries, overweight prevalence in children is 10-20%, compared to 20 - 35% in Southern Europe, with
a trend of increase (OMS, 2000, James, 2004).
A study (1980) conducted in the western part of Romania involving 5250 children aged between 3
months and 16 years, showed a prevalence of obesity of 14,7%, 18,6% in breastfed babies, 15% in
preschoolers, and 14,2% schoolchildren, predominantly in female subjects (Popa, 2001).
The first HBSC research in Romania was conducted between 2005 and 2006 (the study was
published in an IASO report, London, 2009), involving children aged 1-11. The results showed
overweight prevalences of 14,7% in girls, and 8,7% in boys.
According to a study conducted by the Institute of Public Health Bucharest shows the increase of
prevalence rate of non-endocrine obesity in 4th grade schoolchildren from 1,6 %, in 2001 to 3,6% 2008.
Analogously, an increase from 1,7% to 3,4% was observed in 8th graders. A lower obesity prevalence
variation was measured among 12th grade students, from 1,4% in 2001, to 2,8% in 2008.
In Cluj-Napoca, Romania, a study conducted in 2008 involving 7904 1st to 12th grade
schoolchildren from 20 de schools and high schools, showed 12,8% overweight and 8,2% obesity
prevalence rates. The highest prevalence rate was measured in the 6-10 year age group for both
overweight (15,9%), as well as obesity (13,3%), while the lowest rate was measured in adolescents (7,6%
overweight and 3,8% obesity) (Văleanu, 2009).
According to the data provided by the National Centre For Health Evaluation And Promotion
Romania (CNEPSS), obesity prevalence in children aged 3-16 years increased, between 2004 and 2010,
from 0,7%, in rural areas and 1,6% in urban zones, to 1,5% and 3,1% respectively.
The global increase of excess weight prevalence rates is caused by the increase of dietary energy
intake, especially high calorie foods rich in fats and sugars as well as due to reduced physical activity as a
consequence of increased sedentarism. In the case of children with excess weight, during their first years
of life, the risks of becoming obese adults is 80% if both parents are obese and 40% for the children with
only one of the parents with obesity (Arion, 1983 and Nader, 2006).
Obesity, in both childhood as well as in adolescence, represents a risk factor for the occurrence of
cardiovascular diseases (Ogden, 2002), depressions (Hedley et al., 2004) arterial hypertension
(Summerbell, 2005, Bar-Or et al., 1998, Daniels et al., 2005), several forms of cancer (Kelishadi, 2006),
type 2 sugar diabetes (Kelishadi, 2007), hypercholesterolemia, hyperinsulinemia (Freedman et al., 1999),
of the metabolic síndrome (Kimm and Obarzanek, 2002,Daniels et al., 2005),and sleep apnea syndrome
(Papandreou et al., 2008, Summerbell, 2005 and Hedley, 1999-2002). Obesity is also correlated with
reduced GnRH release, respiratory, and orthopaedic diseases (Daniels et al., 2005 and Fulton et al., 2004).
In conclusion, as regards the studied population, important levels of excess weight can be
observed. This emphasizes the need of monitoring this phenomenon for early identification of the young
people who move away from healthy lifestyles as well as those with low physical fitness in order to adopt
the necessary measures for preserving health and prevent chronical diseases that relate to excess weight.
Conclusions
Both girls and boys percentage of overweight is significant.
BMI values obtained indicate that a significant percentage of overweight children are obese
(BMI> 95% ile).
The percentage of boys overweight/obese is higher than girls.
The percentage of overweight/obese decreases with age, the measured sample fits within a normal
BMI.
The results show significant differences in body mass index, by age and gender.
The results obtained by assessing the relationship between BMI and weight on gender, indicates a
direct correlation, very high.
The results obtained by assessing the relationship between height and weight on gender, indicates
a direct correlation, high.
References
- Arion, C., Dragomir, D. & Popescu, V. (1983). Obezitatea la sugar, copil şi adolescent, Edit. Medicală Bucureşti.
- Barlow, S. E. (2007). Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report, Pediatrics; 120:S164-S192.
- Bar-Or, O., Foreyt, J., Bouchard, C., Brownell, K.D., Dietz, W.H., Ravussin, E., Salbe, A.D., Schwenger, S., St. Jeor, S. & Torun, B. (1998). Physical activity, genetic, and nutritional considerations in childhood weight management. Medicine & Science in Sports & Exercise. Jan;30(1):2-10.
- Beers M.H. & coord. (2006). Manualul Merk de diagnostic şi tratament, Edit. a XVIII-a, Ed. All, Bucureşti.
- Daniels, S.R., Arnett, D.K., Eckel, R.H., Gidding, S.S., Hayman, L.L., Kumanyika, S., Robinson, T.N., Scott, B.J., St. Jeor, S. & Williams, C.L. (2005). Overweight in children and adolescents: pathophysiology, consequences, prevention, and treatment. Circulation. Apr 19;111(15):1999-2012.
- Freedman, D.S., Dietz, W.H., Srinivasan, S.R. & Berenson, G.S. (1999). The relation of overweight to cardiovascular risk factors among children and adolescents: the Bogalusa Heart Study. Pediatrics. Jun;103(6 Pt 1):1175-82.
- Fulton, J.E., Garg, M., Galuska, D.A., Rattay, K.T. & Caspersen, C.J. (2004). Public health and clinical recommendations for physical activity and physical fitness: special focus on overweight youth. Sports Medicine;34(9):581-99.
- Hedley, A.A., Ogden, C.L., Johnson, C.L., Carroll, M.D. & Curtin, L.R. (2004). Prevalence of overweight and obesity among US children, adolescents, and adults, 1999-2002. Journal of the American Medical Association; 291:2847-2850.
- International Obesity TaskForce with the European Childhood Obesity Group. Obesity in Europe. (2002) IOTF: Copenhagen, available online on http://www.iotf.org/media/euobesity.pdf.
- James, P. (2004). IOTF Chilhood Obesity Report.
- Kautiainen, S., Rimpela, A., Vikat, A. & Virtanen, S.M. (2002) Secular trends in overweight and obesity among Finnish adolescents in 1977–1999. International Journal of Obesity; 26: 544–552.
- Kelishadi, R. (2006). Childhood obesity in the Eastern Mediterranean region. In: Flamenbaum RK.
- Global dimensions of childhood obesity. 1st ed. New York, NY: NOVA Science Publishers, 71–89.
- Kelishadi, R. (2007). Childhood Overweight, Obesity, and the Metabolic Syndrome in Developing Countries, Epidemiological Reviews;29:62–7, Vol. 29.
- Kimm, S.Y. & Obarzanek, E. (2002). Childhood obesity: a new pandemic of the new millennium. Pediatrics. Nov;110(5):1003-7.
- Krassas GE, Tzotzas T, Tsametis C, Konstantinidis T. (2001). Prevalence and trends in overweight and obesity among children and adolescents in Thessaloniki, Greece. Journal of Pediatric Endocrinology and Metabolism; 14 (Suppl. 5): 1319–1326, discussion 1365.
- Lobstein, T. & Frelut, M.L. (2003). Prevalence of overweight among children in Europe. Obesity Reviews, 4(4):195-200;
- Lobstein, T.J., James, W.P.T. & Cole, T.J. (2003). Increasing levels of excess weight among children in England. International Journal of Obesity; 27: 1136–1138.
- Majem, L.S., Barba, L.S., Bartrina, J.A., Rodrigo, C.P. & Santana, P.S. (2001). Epidemiología de la obesidad infantil y juvenil en España. Resultados del estudio enKid (1998–2000). In: Majem LS, Bartrina JA (eds). Obesidad infantil y juvenil: Estudio enKid (Child and Adolescent Obesity: the Enkid Study). Masson: Barcelona; pp 81–108.
- Manios,Y., Moschandreas, J., Hatzis, C. & Kafatos, A. (2002). Health and nutrition education in primary schools of Crete: changes in chronic disease risk factors following a 6-year intervention programme. British Journal of Nutrition; 88: 315–324.
- Nader, P.R., O'Brien, M., Houts, R., Bradley, R., Belsky, J., Crosnoe, R., Friedman, S., Mei, Z. & Susman E.J. (2006). Identifying risk for obesity in early childhood. Pediatrics; 118: e594–e601.
- Ogden, C.L., Flegal, K.M., Carroll, M.D. & Johnson, C.L. (2002). Prevalence and trends in overweight among US children and adolescents, 1999-2000. Journal of the American Medical Association; 288(14):1728-1732.
- Papandreou, C., Abu Mourad. T., Jildeh, C., Abdeen, Z., Philalithis, A. & Tzanakis, N. (2008). Obesity in Mediterranean region (1997–2007): a systematic review. Obesity Reviews. Volume 9, Issue 5: 389–399.
- Perra, A., Bella, A., Kodra, Y. & Cuccia, M. (2002). Nutritional status, dietary habitus, physical activity and self-perceived body image of pre-adolescents in Catalonia, Sicily. Bollettino Epidemiologico Nazionale; 15: 1–5.
- Popa, I., Brega, D. & Alexa, A. (2001). Obezitatea copilului şi ţesutului adipos, Edit. Mirton, Timişoara.
- Ranga, V. (1990). Tratat de anatomia omului, Editura Medicală, Bucureşti.
- Summerbell, C.D., Waters, E., Edmunds, L.D., Kelly, S., Brown, T. & Campbell, K.J. (2005). Interventions for preventing obesity in children. The Cochrane Database of Systematic Reviews; Suppl 3, No. CD001871.
- Văleanu, C., Tătar, S., Nanulescu, M., Leucuta, A. & Ichim, G. (2009) Prevalence of obesity and overweight among school children in Cluj Napoca, Acta Endocrinologica, Vol. V, No.2, p.213-219.
- Wang Y. & Lobstein T. (2006) Worldwide trends in childhood overweight and obesity. International Journal of Pediatric Obesity; 1:11-25.;
- World Health Organization,Obesity: preventing and managing the global epidemic. (2000) Report of a WHO Consultation, Geneva, available online at http://www.who.int/child-adolescent health.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
25 May 2017
Article Doi
eBook ISBN
978-1-80296-022-8
Publisher
Future Academy
Volume
23
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-2032
Subjects
Educational strategies, educational policy, organization of education, management of education, teacher, teacher training
Cite this article as:
Scurt, M. D., Balint, L., Rogozea, L., & Scurt, C. (2017). Body Mass Index at Puberty Schoolchildren in Romania, Urban Areas. In E. Soare, & C. Langa (Eds.), Education Facing Contemporary World Issues, vol 23. European Proceedings of Social and Behavioural Sciences (pp. 1676-1685). Future Academy. https://doi.org/10.15405/epsbs.2017.05.02.205