
The Importance of the Physical Therapy for Flat Head Syndrome in Infants


Abstract
Flat head syndrome is a disorder that affects the shape of a skull, defined by an asymmetrical conformation/contour/layout of the baby’s head. It can be synostotic (caused by premature fusion of one or more of the cranial sutures) or non-synostotic (caused by the moulding forces which perform on the developingskullinside the utero or after birth). Flat head syndrome, or plagiocephaly, because the condition is medically known, occurs when a flat spot develops on the back part or lateral side of a child's head. Positional plagiocephaly occurs whenexternal forces acts unevenly on the developing child's skull. This can occur during fetal life, but most of the cases of positional plagiocephaly develops after birth/delivery. Its incidence and prevalence among the population has increased considerably in recent years, and its repercussions can extend to the medium-long term, implying that, every day, there is more research on its approach and the effectiveness of different treatment modalities. Kinetic treatment has also been shown to be effective in the treatment of plagiocephaly, especially since neck stiffness is often the primary cause of plagiocephaly, whether it is related to birth or uterine position, early treatment may be fundamental.
Keywords: Facialasymmetry, kinetictreatment, plagiocephaly
Introduction
Flat head syndrome is a disorder that affects the shape of a skull, defined by an asymmetrical conformation/contour/layout of the baby’s head . It can be synostotic (caused by premature fusion of one or more of the cranial sutures) or non-synostotic (caused by the moulding forces which performon the developingskullinside the utero or after birth)
Congenital plagiocephaly is thought to occur accidentally caused by fetal head constraint. According to a review published in the Indian Journal of Human Genetics Trusted Source, more than 180 syndromes, including Apert syndrome and Crouzon syndrome, may be associated with congenital plagiocephaly.
Congenital plagiocephaly, also known as craniosynostosis, is a rare condition. The variety of the abnormal head shapes at children with this condition is caused by premature fusion of the fibrous spaces between the bones of the skull, known as sutures (Panigrahi, 2011).
Problem Statement
Flat head syndrome at the newborn occurs one in 2000 to 2,500 births.
In most cases, the asymmetry is not caused by the synostosis of unilateral coronal or lambdoid sutures, but rather a deformation caused by intrauterine and / or postnatal deforming forces. The classify and diagnosis of plagiocephaly as synostotic or deformational is performed reliably by physical examination and CT scan. Its differential diagnosis is extremely important, as immediate surgical correction is usually indicated for the synostotic type. On the other hand, infants with frontal or occipital deforming plagiocephaly generally respond to classic treatment (Mawji et al., 2013).
The awareness of deforming plagiocephaly allows a more accurate diagnosis and appropriate treatment, avoiding unnecessary surgery in patients with positional modelling.
This research was developed to investigate the effectiveness of kinetic programs in reducing asymmetry in the head and maybe avoidance of other less pleasant measures such as wearing orthopaedic correction tools.
The skull protects the brain, but it is also malleable because of connective tissue between the skull bones known as sutures. This is the reason why the brain can grow/develop and also allow the head to be shaped during delivery, but also make the baby's skull to be vulnerable to deformation.
Mechanical forces are a significant role in both normal and abnormal anthropology.
Unlike malformations, which mean a tissue problem, asymmetries are deviations from normal that result from a response applied by mechanical forces. One of this anomalies is deformational plagiocephaly; it is an asymmetric head’s shape resulting from external pressure acting on the infant's skull. Plagiocephaly usually consists of unilateral occipital flattening, which may be accompanied by anterior displacement of the ipsilateral ear area and frontal humps, and contralateral with occipital involvement. Isolates anterior plagiocephaly, on the other hand, is unusual (Argenta, 2004).
Plagiocephaly usually develops in the first months of life due to the positioning of the child on the abdomen during sleep coupled with a preferential orientation of the head (de Chalain & Park, 2005).
Consequently the baby's head looks asymmetrical. It is described the parallelogram-shaped head at a glance from above.
Acquired deformational plagiocephaly is the main reason for facial asymmetry. It presents as an asymmetric shape of the skull, due to some external factors that press on the baby's head. Plagiocephaly usually develops in the first months of life and its highest prevalence is seen in the first six months of life. (Launonen et al., 2019).
An important characteristic of the baby's skull is that the cranian constitutive bones do not fuse and ossify completely until a quite long period after birth. The soft and foldable skullbones ensure an easier passage through the birth canal and give the little brain enough room to grow.
Soft bones also allow to mould easily a child's head, therefore this is a common cause for occuring flat head syndrome when the baby is sleeping or lying in the same position.
Unintentional cranial deformity is generally less extreme than intentional deformity, but definitive signs of unintentional induced deformity have been found also in archaeological studies.
The aim of developing a treatment for plagiocephaly and other head’s deformities have begun to appear at Johns Hopkins Hospital in the late 1950 (Lekovic et al., 2007).
Deformational plagiocephaly is caused by the pressure even of gentle external forces on soft and malleable bones of developing child's skull. This can occur consequently to the position into the womb, but more often develops postnatal. The Campaign to Prevent the Risk of Sudden Infant Death Syndrome aims to educate parents and health professionals about how babies sleep, so they are advised to use back- sleeping. According to statistics, the incidence of sudden death syndrome has decreased significantly since the launch of the campaign.
Positional plagiocephaly is a common cranial asymmetry among children and means that the shape of the head is flattened and asymmetrical. Most of the time, the flat head is associated with the time when the child is in the supine position and is associated with congenital muscular torticollis (Pastor-Pons et al., 2021).
Congenital torticollis represents an ipsilateral deviation and contralateral postural cervical rotation, through the shortening of the sternocleidomastoid muscle observed immediately after birth and affects approximately 16% of newborns (Sargent et al., 2019). Torticollis and head deformity has seen an increase in recent years, requiring greater attention from specialists to manage the conditions. (Limpaphayom et al., 2019).
The association between torticollis and cephalic deformation is somewhat incomprehensible, because the causality differs from child to child, they suffer from both conditions at the same time. The recovery program can be similar in some places for torticollis, but also for plagiocephaly, there being no relevant studies in this regard. No recovery protocols are available that take into account the severity of the condition and the age of the infant. The most serious problem is when they are associated with other conditions and anomalies of the locomotor system or even the delay in motor development (Ellwood et al., 2020).
Regarding recovery, the results show that the sooner infants are diagnosed and treated, the better the results, the recommendation is to start physiotherapy treatment in the first month of life. If treated after the age of 3 months, the pathology can cause craniofacial deformations, dysmorphism, conditions that require more invasive interventions (González-Villén & Carmona-Espejo, 2020).
Research Questions
The working hypotheses of this paper were:
If a patient with a deviation from the normal appearance of the cranial box gets through a program that include physical therapy, complementary therapeutic techniques, well dosed, combined with stretching exercises, then he/she will experience a faster improvement of the aesthetic condition of the head.
The success of physical therapy in the recovery of cranial deficiencies depends on the initial clinical form of the disease.
In order to assess the child's evolution, we took into account several criteria:
Examination that consists in palpating the bony prominence at the level of the synostosis suture. Measurements of the occipital-frontal circumference (cranial perimeter) may be normal, even in the presence of cranial box deformities.
Somatic development
All measurements made for the assessment of growth must be related to the average age of the child; the average of the group to which the child belongs; the previous value of those measurements.
The increase is appreciated by: the correct attitude of the body and the deviations from the normal; coincidence of the chronological and biological age; the coincidence of the child’s gender and his physical growth.
To assess the size of the head we used a graduated anthropometer, classical, fitteded with sliding arms and rounded ends and covering the range from 0 to 430 mm. Therefore, the instrument can be used to measure not only the size of the head, but also the selected dimensions of lateral and antero-posterior diameters at children up to the age of about 15 years (biacromial diameter, bitrohanterian diameter, transverse diameter of the chest, etc.).
Usually, the diagnosis of positional cranial asymmetry is possible only through a clinical medical examination.
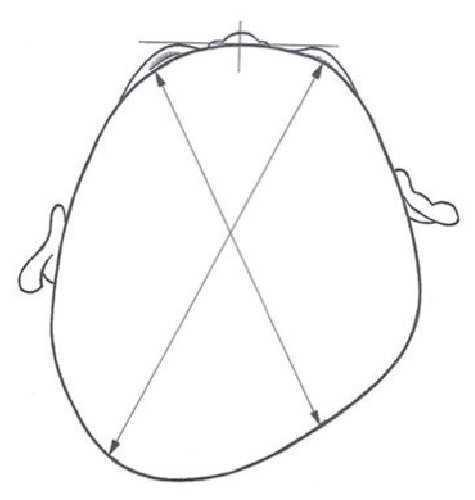
In addition to the clinical description, diagonal diameters (figure 1), head’s position, width and circumference are captured by applying standard cephalometric measurements using an anthropometer. Such measurements performed directly on the head, of landmarks anthropometrically established, are reliable, being the difference between the largest and smallest diagonal diameter of the skull. An index CVA <3 mm is considered physiological, a deviation between 3 mm and 12 mm is considered a mild to moderate asymmetry and a deviation over 12 mm is considered a moderate to severe asymmetry (Mortenson & Steinbok, 2006).
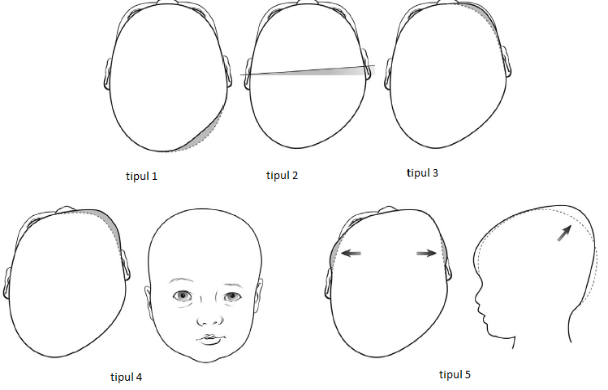
Branch performed a classification based on clinical features. A categorization system is useful in deformational plagiocephaly to help classify patients and develop a treatment strategy. The Argenta classification represents a 5-point clinical (figure 2) scale for unilateral plagiocephaly (Branch et al., 2015).
It does not require additional instruments for measuring and classifying asymmetry and is divided into 5 categories: (Neumann, 1942).
posterior asymmetry only.
posterior asymmetry and ipsilateral ear with incorrect alignment.
involves the two previous categories, as well as the asymmetry of the forehead
includes facial asymmetry
in addition to the above features, there is also temporal protuberance or posterior vertical cranial growth.
Purpose of the Study
The aim of the paper is to show the importance and usefulness of using recovery methods, respectively medical recovery programs, in order to control the flat head appearance of the skull.
Research Methods
The theoretical objective of this paper is to define the general framework of the cranial deformations’ forms. The theoretical substantiation chapter includes elements of descriptive anatomy of the skull, its biomechanics, clinical, etio-pathogenic and anatomy-pathological description of various forms of plagiocephaly, methods of joint testing of the cervical spine, also the general principles of treatment for various forms of flat head.
The applicative objective of the paper aims to compile programs for the recovery of plagiocephaly based on physical therapy, complementary therapeutic techniques, combined with stretching exercises, and to assess their effectiveness for various clinical forms of manifestation.
The tasks that underlay achievement of these described objectives were the following:
The specialized bibliographic study on the anatomy and biomechanics of the skull, the delimitation of the characteristics of the head and face, the functional evaluation’s methods of the development of the skull and the therapeutic means used for the treatment and recovery of various clinical forms.
Studying the references related to the research methodology in the corporal activities in general and in the particular context of the application of the recovery means to the patients with skull’s pathological development conditions ensured capturing the ways the physio pathological evolution of the child's head, being preserved the evaluation tools that are suitable for use in the imposed conditions.
Proposals for recovery’ programs.
Formulation of conclusions and proposals.
Experimental design
In the experimental part, I will present a complementary techniques’ program for the recovery of plagiocephaly in a 6-month-old baby. Before starting the program, an evaluation of the patient's condition was performed, and at the end of the program the evaluation will be performed again, which aims to highlight the effectiveness of combining recovery techniques to improve the shape of the skull.
At each examination, the anthropometric measurements’ results of head *(table 1), Argenta scale and motor development were centralized.
Case presentation
A. M-D, 6 months old, male, domiciled in Bucharest, is brought by his parents to the crania-sacral therapy office, with the diagnosis of positional plagiocephaly, grade 2 and with a cranial perimeter of 42 cm.
General data on pregnancy, childbirth and subsequent hospitalizations were collected from maternal and infant medical records. Clinical examinations were performed in the maternity ward at birth and in an ambulatory clinic at each visit to the paediatrician.
The recovery program will include medical recovery sessions, performed 3 times a week, followed by daily osteopathic exercises.
The program will run for a period of 6 months.
Recovery program objectives:
Correction of cranial asymmetry;
maintaining corrective and hyper corrective postures of the head;
Toning and lengthening the potentially affected muscles of the neck;
Formation of the reflex of correct posture of the child's head and neck in static and dynamic situations of the body;
Exercise program:
Working time 45 - 50 minutes.
Official data also confirm that manipulative treatment is effective in treating plagiocephaly.
Passive mobilizations in order to stretch the affected muscles,
Passive mobilizations will be performed by the physiotherapist and will consist of:
Head and neck extensions;
Lateral tilts of the head and neck;
Rear head’s circumduction;
Stretching in the vertical axis of the spine.
Findings
After the rigorous recovery program that the patient followed at the final evaluation were registered the following results:
Cranial perimeter 41 cm 48 cm.
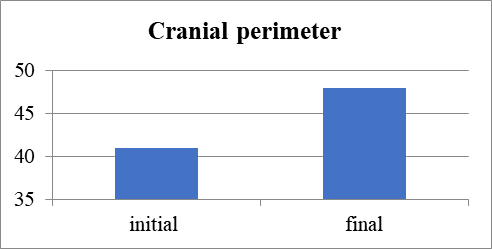
It is observed in the evaluation of the cranial perimeter (fig. 3) that the infant registered normal values, 48 cm (table 1) at the age of 12 months, thus the suspicion of craniostenosis was removed.
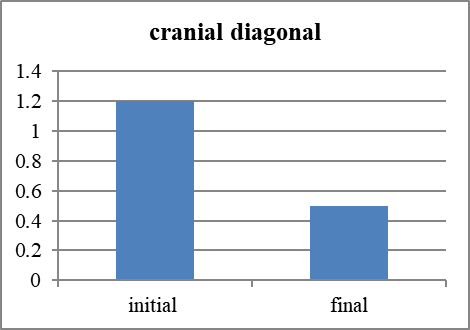
It is observed in the evaluation of the cranial oblique diameters (figure 4) that lower values were registered at the final evaluation (table 2), so we can say that the evolution is satisfactory, the level of asymmetry going from moderate to slight.
Conclusions
Its incidence and prevalence in the population has increased considerably in recent years, and its repercussions can go to medium-long term, implying that, every day, there is more research on its approach and the effectiveness of different ways of treatment.
In terms of evidence, the degree of recommendation and methodological quality are low in most studies.
Flat head syndrome does not affect brain growth, but may later affect the child's development. Physical therapy for torticollis should include checking the child's progress and additional exercises to treat any delays.
The most commonly used physiotherapy techniques are exercises to improve motor development, active and passive mobilization of the cervical spine, flexion and stretching, and manual therapy techniques in joints that have some limitations.
In response to the main objective of this study and the research question on which it is based, physiotherapy would be an effective method of treatment in cranial asymmetry, especially in less severe degrees of pathology (mild to moderate).
If this change early diagnosed, the use of physical therapy as the only method of treatment would be sufficient in most cases to obtain optimal results, because in this field the objectives are to normalize the child's motor development and serve as a strong preventive measure, so that the disease does not progress.
The child is stimulated to sit on his stomach on a colourful rug. It starts with a few minutes per session that repeats several times during a day. As the baby develops and neck’s control occurs, the amount of time for a session may increase.
References
Argenta, L. (2004). Clinical Classification of Positional Plagiocephaly. Journal of Craniofacial Surgery, 15(3), 368-372. DOI:
Branch, L. G., Kesty, K., Krebs, E., Wright, L., Leger, S., & David, L. R. (2015). Argenta Clinical Classification of Deformational Plagiocephaly. Journal of Craniofacial Surgery, 26(3), 606-610. DOI:
de Chalain, T. M. B., & Park, S. (2005). Torticollis Associated with Positional Plagiocephaly: A Growing Epidemic. Journal of Craniofacial Surgery, 16(3), 411-418. DOI:
Ellwood, J., Draper-Rodi, J., & Carnes, D. (2020). The effectiveness and safety of conservative interventions for positional plagiocephaly and congenital muscular torticollis: a synthesis of systematic reviews and guidance. Chiropractic & Manual Therapies, 28(1). DOI:
González-Villén, R., & Carmona-Espejo, A. (2020). Tortícolis muscular congénita. Actualización en terapias. Revista Mexicana de Medicina Física y Rehabilitación, 32(3-4), 52-61. DOI:
Launonen, A. M., Vuollo, V., Aarnivala, H., Heikkinen, T., Pirttiniemi, P., Valkama, A. M., & Harila, V. (2019). Craniofacial Asymmetry from One to Three Years of Age: A Prospective Cohort Study with 3D Imaging. Journal of Clinical Medicine, 9(1), 70. DOI:
Lekovic, G. P., Baker, B. J., Lekovic, J. M., & Preul, M. C. (2007). New World Cranial Deformation Practices: Historical Implications For Pathophysiology Of Cognitive Impairment In Deformational Plagiocephaly. Neurosurgery, 60(6), 1137-1147. DOI:
Limpaphayom, N., Kohan, E., Huser, A., Michalska-Flynn, M., Stewart, S., & Dobbs, M. B. (2019). Use of Combined Botulinum Toxin and Physical Therapy for Treatment Resistant Congenital Muscular Torticollis. Journal of Pediatric Orthopaedics, 39(5), e343-e348. DOI:
Mawji, A., Vollman, A. R., Hatfield, J., McNeil, D. A., & Sauvé, R. (2013). The Incidence of Positional Plagiocephaly: A Cohort Study. Pediatrics, 132(2), 298-304. DOI:
Mortenson, P. A., & Steinbok, P. (2006). Quantifying Positional Plagiocephaly: Reliability and Validity of Anthropometric Measurements. Journal of Craniofacial Surgery, 17(3), 413-419. DOI:
Neumann, G. K. (1942). Types of Artificial Cranial Deformation in the Eastern United States. American Antiquity, 7(3), 306-310. DOI:
Panigrahi, I. (2011). Craniosynostosis genetics: The mystery unfolds. Indian Journal of Human Genetics, 17(2), 48. DOI:
Pastor-Pons, I., Hidalgo-García, C., Lucha-López, M. O., Barrau-Lalmolda, M., Rodes-Pastor, I., Rodríguez-Fernández, Á. L., & Tricás-Moreno, J. M. (2021). Effectiveness of pediatric integrative manual therapy in cervical movement limitation in infants with positional plagiocephaly: a randomized controlled trial. Italian Journal of Pediatrics, 47(1). DOI:
Sargent, B., Kaplan, S. L., Coulter, C., & Baker, C. (2019). Congenital Muscular Torticollis: Bridging the Gap Between Research and Clinical Practice. Pediatrics, 144(2). DOI:
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
10 April 2023
Article Doi
eBook ISBN
978-1-80296-961-0
Publisher
European Publisher
Volume
5
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-1463
Subjects
Education sciences, teacher education, curriculum development, educational policies and management
Cite this article as:
Andrei, D. (2023). The Importance of the Physical Therapy for Flat Head Syndrome in Infants. In E. Soare, & C. Langa (Eds.), Education Facing Contemporary World Issues - EDU WORLD 2022, vol 5. European Proceedings of Educational Sciences (pp. 1044-1052). European Publisher. https://doi.org/10.15405/epes.23045.105