
Research Of Hand Reflexology Stimulation In Children With Adhd


Abstract
Some children aged 6-9 years with ADHD have, among other things, motoric disorders, which may make it difficult for them to solve common practical tasks associated with the learning process. Is there a statistically significant difference between the results of the entry and exit tests and the control and the experimental group in practical tasks (children with ADHD)? The study should demonstrate the importance of knowledge related to human hand morphology and especially activation of fine motoric skills through a set of practical hand pressure exercises in selected individuals with ADHD. In the experimental group of children pressure exercises related to the knowledge of hand morphology were tested and in the control group were not. When comparing the groups using paired t-tests and the student's t-test, we intend to demonstrate that simple pressure stimulation can help to improve fine motoric skills in some individuals with ADHD. The pilot research carried out showed improvement in some individuals after 90 days of targeted pressure exercises in solving a set of practical tasks. The improvement depended on the extent, form of ADHD, type of task, task time, and other factors and became the basis for further and more extensive study. The study suggests that a higher rate of targeted practical exercises or other appropriate activities may lead to improved fine and gross motoric skills in selected individuals with ADHD.
Keywords: ReflexologyhandstimulationchildrenADHDexperimental research
Introduction
Reflexology is a natural holistic therapy using special techniques on the feet and hands to stimulate specific points and initiate a beneficial response in another area of the body. Reflexology is non-invasive therapy performed using special manipulations with varying degrees of pressure to provide benefits to the persons that are both physical and emotional. It is based on the principle that there are reflex zones which are linked by energy pathways to corresponding parts of the body and, when pressure is applied, it stimulates the movement of energy along these pathways (Cressy, 2003). Thus, the findings showed that reflexological stimulation induced a somatosensory process corresponding to the stimulated reflex area and that a neuroimaging approach can be used to examine the basis of reflexology effects (Nakamaru, Naoki, Fukushima, & Kawashima, 2008). The study of Taheri et al. (2019) showed that foot reflexology was more effective than hand reflexology in pain alleviation.
As a younger school age, we usually refer to the period from 6 -7 years, when the child enters school, to 11-12 years, when the first signs of sexual adolescence begin with accompanying psychological manifestations (Ptáček & Ptáčková, 2018). Indeed, the world of the school is decisively marking this period. Gross and fine motor skills improve significantly and continuously throughout the period. The movements are faster, the muscular strength is greater and the improved coordination of all movements of the whole body is especially noticeable. Improved performance in learning writing and drawing also depends on it (Langmeier & Krejčírová, 2006).
ADHD (Attention Deficit Hyperactivity Disorder) is frequently accompanied by motor coordination problems. However, the co-occurrence of poor motor performance has received less attention in research than other coexisting problems in ADHD. The underlying mechanisms of this association remain unclear. Therefore, it investigated the prevalence of motor coordination problems in a large sample of children with ADHD, and the relationship between motor coordination problems and inattentive and hyperactive/impulsive symptoms. Furthermore, it assessed whether the association between ADHD and motor coordination problems was comparable across ages and was similar for both genders. Parents and teachers reported motor coordination problems in about one third of children with ADHD. Problems of fine and gross motor skills, coordination skills and motor control were all related to inattentive rather than hyperactive/impulsive symptoms (Langmeier & Krejčírová, 2006). Relative to controls, motor coordination problems in ADHD were still present in teenagers according to parents, the prevalence diminished somewhat according to teachers. Boys and girls with ADHD were comparably affected, but motor performance in controls was better in girls than in boys. Motor coordination problems were reported in one third of children with ADHD and affected both boys and girls. These problems were also apparent in adolescents with ADHD. Clinicians treating children with ADHD should pay attention to co-occurring motor coordination problems because of the high prevalence and the negative impact of motor coordination problems on daily life (Fliers et al., 2008). The etiology and pathophysiology of ADHD is incompletely understood. There is evidence of a genetic basis for ADHD but it is likely to involve many genes of small individual effect. Differences in the dimensions of the frontal lobes, caudate nucleus, and cerebellar vermis have been demonstrated. Neuropsychological testing has revealed a number of well documented differences between children with and without ADHD (Tripp & Wickens, 2009). In study of Mokobane, Pillay, and Meyer (2019) children with ADHD (predominantly inattentive subtype) and ADHD (combined subtype) performed significantly more poorly than the control group on the Grooved Pegboard (p < 0.05) with both the dominant and non-dominant hand. No significant difference between the hyperactivity and impulsiveness subtype and the controls were found. There was no difference on the Maze Coordination Task (p > 0.05) between the ADHD subtypes and the controls. Difficulties in fine motor skills are prevalent in children with ADHD, particularly in the ADHD-PI and ADHD-C. Problems are encountered in distal, complex, speeded tasks. The effect may lead to poor handwriting and academic performance. In study of Fenollar-Cortés, Gallego-Martínez, and Fuentes (2017) children with ADHD performed worse than typically developing on all tasks (Fine motor tasks). After controlling for age and ADHD-HY (hyperactivity/impulsivity), higher scores on ADHD-IN (inattentiveness) predicted a larger number of mistakes among all psychomotricity tasks and conditions. The ADHD group showed poorer fine motor performance than controls across all fine motor coordination tasks. However, lower performance (more mistakes), was related to the inattention dimension but not to the hyperactivity/impulsivity dimensions.
ADHD populations exhibit various abnormalities in many motor components. Deficits exhibited in attention are reflected mainly in more omission errors and increased RTV (Response Time Variability). Further deficiencies are reflected in motion execution by deficits in fine and gross motor ability, less fluent and jerkier movements, and finally in motor monitoring in reduced post error slowing. The abnormalities may be related to cyclic pattern of attentional processes, deficits in the inhibitory process, or general slowness of information processing. Motor execution deficiencies may be related to a less optimal speed selection process, delayed maturation and to deficiencies in the dopaminergic fronto-striatal circuitry. Such evidence emerges from diverse research paradigms and relate to different aspects of movement. Some of these abnormalities have been shown to be reflected in abnormal oscillatory patterns. Beta and gamma bands, beta band synchronization and desynchronization have been suggested as a key factor in attentional processes. Abnormalities in beta band oscillations and in changes in SCP (Slow Cortical Potentials) as reflected by the CNV (Contingent Negative Variation) components have been shown to be related to motor preparation/planning, and to have abnormal patterns in ADHD individuals (Dahan, Ryder, & Reiner, 2018). Another study suggests that abnormalities in circuits important for motor response selection contribute to deficits in response inhibition in children with ADHD (Waldman & Faraone, 2002).
Problem Statement
Children with ADHD often show motor difficulties such as poor motor coordination or motor performance and balance. Evidences have been proven for problems in motor development, motor skills and abilities in children with ADHD. Simple pressure stimulation of reflexology points on the palm can help to improve fine motoric skills in some individuals with ADHD.
Research Questions
Is there a statistically significant difference between the results of the input and output tests?
Is there a statistically significant difference between the control and the experimental group in solving of practical tasks?
Purpose of the Study
The purpose of the study is experimental research of hand reflexology therapy with Stone Ball in children with ADHD. The main aim of the study was proved that experimental therapy can improve the fine motor skills in practical tasks (school activities, informative and technical technology, handiwork, practical needs of everyday life and playing on musical instrument).
Research Methods
The basic group of respondents to the research survey consisted of children with ADHD - mild brain dysfunction with attention deficit syndrome aged 6 - 11 years (Langmeier & Krejčířová, 2006). The sample included individuals with the following manifestations of ADHD: difficulties in the child's motor restlessness (increased need for movement), impulsivity (accelerated reactions without judgment), inattention (selection of essentials), social incompetence (socialization in the team, keeping rules), organizational problems (time management), impaired coordination and fine motor skills (elementary skill), school or work failure. The total group consisted of 20 respondents (12 girls and 8 boys) (Table
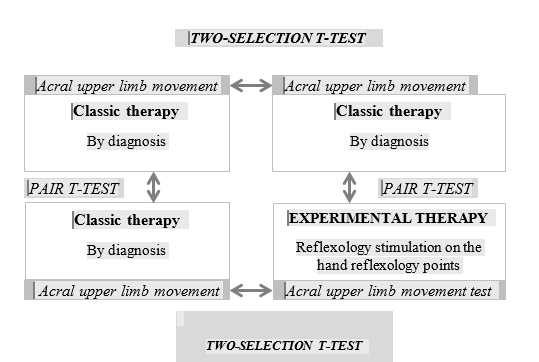
The control group continued for 2 months using conventional methods of approaching ADHD. For the experimental group, we included techniques based on activities affecting the stimulation of nerve endings of reflexological points on the palm of the hand and fingertips. The experimental group did exercises with Stone Ball (series 5 times a day): a) passing Stone Ball from left hand to right hand and vice versa (2 minutes); b) rolling the Stone Ball with both hands and palms on the mat (2 minutes); c) throwing the Stone Ball from hand to hand (2 minutes); d) strong squeezing of Stone Ball (pressure) (2 minutes); e) Rotate the Stone Ball in the centre of the palms (2 minutes), (Lavrinčík & Skutka, 2016).
Findings
Differences between input tests
To successfully implement a two-sample t-test for input tests, we first proceeded to verify the normality of the data, which showed that the data set according to the calculated values of the K-S Lilliefors´s test and Shapiro-Wilk´s test of data normality reached standard values. In the case of using a two-sample t-test, the Statistica application offers two different methodological approaches, so the comparison of independent samples according to variables or according to groups (Gavora, 2010). The variant according to the variables is better suited for our data set. To verify the result (p values), we also chose the Leven´s test and the Brown Forsyth´s test, which test the homogeneity of the data variance. The results in the table
Differences between output tests
For the successful implementation of a two-sample t-test for output tests, we first proceeded to verify the normality of the data, which showed that the data set according to the calculated values of the K-S Lilliefors´s test and Shapiro-Wilk´s test of data normality reached standard values. In the case of using a two-sample t-test, the Statistica application offers two different methodological approaches, namely the comparison of independent samples according to variables or according to groups. The variant according to the variables is better suited for our data set. To verify the result (p values), we also chose the Leven´s test and the Brown Forsyth´s test, which test the homogeneity of the data variance. The results shown in Table
Differences between input and output tests of control group
Based on the performed partial analyzes in the form of testing the normality of the data, it was possible to proceed to the testing of the partial hypotheses, as the above-mentioned results showed satisfactory values (Gavora, 2010). For testing purposes, the analysis was performed using the paired t-test method, the results of which are summarized in the tables below (Table
For the implementation of the pre-research survey in the control group, we had 10 identical students (n = 10) for the entrance test and the same 10 students (n = 10) for the exit test. The test score per student ranged from 1 point to 5 points maximum, the average number of points from 1.7 to 2.1 according to the measurement, the confidence interval (95%) in the case of the entrance test ranged from 0.80 to 2, 59, for output 1.24 to 2.95. Thus, the average ninety-five percent probability lay within the calculated interval (Chráska, 2016).
Based on the results of the t-test for the dependent samples, it was possible to state that the difference between the averages was 0.4 points. We calculated the statistic t for 10 degrees of freedom. According to the value at the level of significance α = 0.05, the observed level of frequency reached the value p <0.103888. By comparing p < α at the 5% level of significance, it was possible to reject the claim that the students of the control group (conventional method of teaching) did not achieve a higher score. The achieved score of the same input and output test does not differ after completing the standard method of teaching. The results show that the students of the control group achieved the same score on average (they did not improve) when solving the tasks of the input and output test, the difference was only 0.4 points. The average score of 2.1 points out of a total of 5 points is only about 19% success. Tasks focused on playing a musical instrument and working with paper, wood, textiles, and other small materials had the greatest impact on the overall low score. We believe that this fact is mainly because the current teaching does not develop feeling in the fingers and fine motor skills, and students do not have difficulty approaching tasks for which mechanical memory is insufficient.
Differences between input and output tests of experimental group
Based on the performed partial analyzes in the form of testing the normality of the data, it was possible to proceed to the testing of the partial hypotheses, as the above-mentioned results showed satisfactory values. For testing purposes, an analysis was performed using the paired t-test method, the results of which are summarized in tables below (Table
For the implementation of the pre-research survey in the control group, we had 10 identical students (n = 10) for the input test and the same 10 students (n = 10) for the output test. The obtained test score per student ranged from 1 point to 5 points (maximum). The average number of points from 1.5 to 3.0 according to the measurement. The confidence interval (95%) in the case of the input test ranged from 0.89 to 2,10 at the output 1.78 to 4.21. Thus, the average ninety-five percent probability lay within the calculated interval.
Based on the results of the t-test for the dependent samples, it was possible to state that the difference between the averages was 0.4 points. We calculated the statistic t for 10 degrees of freedom. According to the value at the level of significance α = 0.05, the observed level of frequency reached the value p <0.001742. By comparing p < α at the 5% level of significance, it was possible to accept the statement that the students of the experimental group (unconventional way of teaching) achieved a higher score. The achieved score of the same input and output test differs after completing the teaching focused on hand reflexology. The results show that the students of the control group achieved the same score on average (they did not improve) when solving the tasks of the input and output test, the difference was only 1.5 points (which is exactly double). The average score of 3.0 points out of a total of 5 points is only about 50% success. The greatest influence on the overall increase in the score had the tasks focused on playing with touch tablets, drawing with a pencil / coloured pencil focusing on the details of objects / people and animals and turning on the button, tying shoelaces. We believe that this fact is mainly because children with ADHD respond well to a combination of teaching interspersed with practical tasks, the inclusion of touch tablets in teaching.
Conclusion
Based on the used research methods and techniques, we now summarize the achieved results of the research survey. After randomly dividing the students into a control group (10 students) and an experimental group (10 students), we proceeded to the processing using a statistical method for the analysis of metric data - paired t-test and two-sample t-test. Our task was to test the research question whether there is a statistically significant difference between the achieved results of the input and output test? Furthermore, is there a difference between the control and experimental groups in the practical solution of practical tasks in children with ADHD? Overall, thanks to the Student's t-test method and the two-sample test, it was confirmed that there was a significant improvement in the test score in the final test of the experimental group. From the measured and calculated results, it is worth mentioning the worse average achieved score in the entrance test of the experimental group than in the entrance test of the control group. However, the control group was unable to take advantage of the entry advantage. Between the outcome tests, the scores of the students in the experimental group more than doubled. We can therefore state that our established and implemented teaching system focused on a set of activities focused on the therapy of nerve endings of reflexological points at the ends of the hand significantly helped to increase the score in the output test of the experimental group, especially in activities related to common competencies for the 21st century. Furthermore, the research showed that our proposed model was successfully verified. With his help, we presented the students of the experimental group with educational content primarily intended for teaching with more severe forms of ADHD to support and develop fine motor skills. The increase in the score was noticeable. The task of possible follow-up research will be to confirm the universality of the one proposed for other disadvantages, such as cerebral palsy, developmental dyspraxia, and others. Although it is possible to consider the presented results as partial, they provided us the necessary methodological basis for the implementation of further research. In the future, we will try to transfer the methodology used above to follow-up research, but to supplement it with other factors and disadvantages that we did not anticipate at the time of preparing this research.
Acknowledgments
We thank to M.D. Ivan Krupa for his advice and cooperation during the experimental research.
References
- Cressy, S. (2003). Reflexology. Heinemann: Portsmouth.
- Dahan, A., Ryder, C. H., & Reiner, M. (2018). Components of motor deficiencies in ADHD and possible interventions. Neuroscience, 15(378), 34–53.
- Fenollar-Cortés, J., Gallego-Martínez, A., & Fuentes, L. J. (2017). The role of inattention and hyperactivity/impulsivity in the fine motor coordination in children with ADHD. Research in Developmental Disabilities, 69, 77-84. https://doi.org/10.1016/j.ridd.2017.08.003.
- Fliers, E., Rommelse, N., Vermeulen, S. H. H. M., Altink, M., Buschgens, C. J. M., Faraone, S. V., ... & Buitelaar, J. K. (2008). Motor coordination problems in children and adolescents with ADHD rated by parents and teachers: effects of age and gender. Journal of neural transmission, 115(2), 211-220. https://doi.org/10.1007/s00702-007-0827-0
- Gavora, P. (2010). Úvod do pedagogického výzkumu. [Introduction to pedagogical research]. Brno: Paido.
- Chráska, M. (2016). Metody pedagogického výzkumu: základy kvantitativního výzkumu. [Methods of pedagogical research: basics of quantitative research]. Praha: Grada.
- Chráska, M., & Kočvarová, I. (2015). Kvantitativní metody sběru dat v pedagogických výzkumech. [Quantitative methods of data collection in pedagogical research]. Zlín: Univerzita Tomáše Bati ve Zlíně, Fakulta humanitních studií.
- Langmeier, J., & Krejčířová, D. (2006). Vývojová psychologie. [Developmental Psychology]. Praha: Grada.
- Lavrinčík, J., & Skutka, K. (2016). Reflexologický válec a koule. [Reflexological cylinder and ball]. Czech Republic.
- Mokobane, M., Pillay, B. J., & Meyer, A. (2019). Fine motor deficits and attention deficit hyperactivity disorder in primary school children. South African Journal of Psychiatry, 25(1).
- Nakamaru, T., Naoki, M., Fukushima, R., & Kawashima, R. (2008). Somatotopical relationships between cortical activity and reflex areas inreflexology: A functional magnetic resonance imaging study. Neuroscience Letters, 448, 6–9.
- Ptáček, R., & Ptáčková, H. (2018). ADHD - variabilita v dětství a dospělosti. [ADHD - variability in childhood and adulthood]. Praha: Karolinum.
- Taheri, H., Naseri-Salahshour, V., Abedi, A., & Sajadi, M. (2019). Comparing the Effect of Foot and Hand Reflexology on Pain Severity after Appendectomy: A Randomized Clinical Trial. Iranian journal of nursing and midwifery research, 24(6), 451–456. https://doi.org/10.4103/ijnmr.IJNMR_85_18
- Tripp, G., & Wickens, J. R. (2009). Neurobiology of ADHD. Neuropharmacology, 57(7-8), 579-589. https://doi.org/10.1016/j.neuropharm.2009.07.026
- Waldman, I., & Faraone, S. V. (2002). A meta-analysis of linkage and association between the dopamine transporter gene (DAT1) and childhood ADHD. Behavior Genetics. 32, 487-487.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
25 December 2020
Article Doi
eBook ISBN
978-1-80296-951-1
Publisher
European Publisher
Volume
1
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-322
Subjects
Cognitive psychology, education, educational psychology, teacher training, social psychology, group psychology,
Cite this article as:
Lavrinčík, J., & Tománková, K. (2020). Research Of Hand Reflexology Stimulation In Children With Adhd. In I. Elkina, & S. Ivanova (Eds.), Cognitive - Social, and Behavioural Sciences - icCSBs 2020, vol 1. European Proceedings of Educational Sciences (pp. 143-152). European Publisher. https://doi.org/10.15405/epes.20121.17