
Financial Corruption in the Healthcare Sector of Bangladesh During Covid-19 Pandemic


Abstract
A global economic catastrophe brought on by the current COVID-19 pandemic in addition to a public health emergency. The disease mitigation financial measures are taken by most countries around the world because of dealing with the overwhelming pressure in the health sector. While countries experience significant falls in revenue with a drastic rise in unemployment, supply chain disruption, and interruption in the production and services sectors. On the other hand, the healthcare sector has been playing the most significant role during COVID-19 and governments also prioritize this sector in budget allocation. However, it has been revealed in the news that some parties have been misusing, mismanaging and embezzling funds from this sector. This paper aims to explore the corruption in the healthcare sector related to COVID-19 management of Bangladesh during the COVID-19 pandemic from March 2020 to June 2021 based on the formal news media report. The study observes the issue based on the case study as the methodology. The findings revealed that mismanagement relating to purchasing fake masks by hospitals, providing fake COVID-19 test certificates, and overcharging for COVID-19 tests were rampant during the primary stage of infection in Bangladesh which also motivated financial corruption in this sector. The study also identifies loopholes in managing the public funds of the healthcare sector during the pandemic crisis due to poor governance in the sector. The study will assist healthcare authorities in understanding the financial corruption and governance flaws that exist in this sector during the COVID-19 pandemic.
Keywords: Bangladesh, COVID-19, Corruption, Healthcare Corruption, Quality of Governance
Introduction
The World Health Organization (WHO) announced that COVID-19 was a pandemic on 11 March 2020. As of Johns Hopkins University, the Corona Virus Center reports that more than 109 million cases have been confirmed by February 18, 2021, and that 2.4 million deaths from COVID-19 have been reported worldwide. Most countries have been trying their best to fight against the pandemic by allocating a huge amount of government budget to assist citizens who are in need by providing financial and non-financial support. The budget allocation which is supposed to be distributed to the affected citizens was very much exposed to mismanagement in many countries especially in several developing countries (Ruiu, 2020).
At the same time, a large number of COVID-19 instances between the years 2020 and 2021 caused severe problems for many wealthy nations, like Italy, Spain, the United States, and European Union countries. Less developed nations, on the other hand, struggle severely to combat the crisis from various angles, such as inconsistent lockdown, food insecurity, an increase in unemployment, inadequate social safety fund distribution, corruption in benefit distribution, a fragile health care system, and even significant corruption in the health care sector during the pandemic (Chookajorn et al., 2021). The pandemic, however, draws attention to the inadequate healthcare systems of many developing nations, particularly Bangladesh, which is plagued by a variety of issues, including financial corruption in the healthcare industry. Bangladesh is one of the most densely populated countries in the world, with 1,115 people per square kilometre, and a poverty rate of 21.8%. The issues have a bigger impact on the COVID-19 pandemic.
The country will have 0.6367 doctors per 1,000 people in 2019 according to the World Development Indicator of the World Bank (Chowdhury et al., 2021). The fact that this country has one of the lowest per capita healthcare budgets means that people must pay out of pocket in order to access healthcare. Due to all of these factors, the healthcare sector is extremely vulnerable to crises like the COVID-19 pandemic. However, the nation's healthcare system is unreliable, responsive, and empathic, and it has repeatedly been demonstrated to be insufficient to offer people high-quality healthcare (Andaleeb et al., 2007; Mohiuddin, 2019). Meanwhile, COVID-19 hits the nation and reveals numerous flaws in the healthcare system that also encourage financial malfeasance.
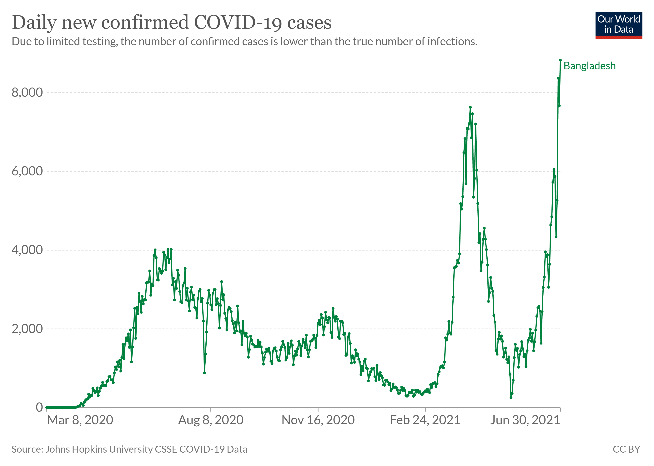
Bangladesh is currently one of the countries most severely affected by COVID-19, with 0.54 million total confirmed cases, 8329 total deaths, and more than 8,000 thousand confirmed cases reported each day by the Johns Hopkins University, Corona Virus Center by 18 February 2021, as shown in Figure 1. Early in 2020, the Bangladeshi government provided substantial funding to the healthcare industry in an effort to stop the spread of COVID-19. The Bangladeshi mainstream news media, however, has stated that a group of individuals mismanaged the COVID-19 budget allocation through a number of routes, utilising their power to steal and extract the funds.
As an immediate measure to limit infection, the Bangladeshi government invests an extensive fund for the healthcare industry as well as financial and non-financial support for individuals who are in need. Despite the positive gesture from the government, the country has faced some COVID-19-linked financial corruption, i.e., purchasing fake masks in cheap, providing fake COVID-19 test certificates, imposing a high charge on COVID-19 tests, and so on during the primary stage of infection to misappropriate the allocated fund from the health care sector (Al-Zaman, 2020).
To stop the COVID-19 infection from spreading, the Bangladeshi government enacts laws that are approved by the WHO. In order to provide individuals with access to affordable COVID-19-related healthcare, the government has also designated a number of public hospitals as well as a number of independent institutions for COVID-19 testing and treatment. However, as the number of daily infected patients increased, the state hospital was no longer able to meet the demand for services, as the government now permits some strategically selected private hospitals to offer COVID-19-related services (BBC Bangla, 2020c). The price of the COVID-19 test has reportedly been set by the government at BDT 200 (about USD 2.5, as of July 2021) in order to protect citizens' right to affordable health care (BanglaNews24.com, 2020). However, the country's sudden spike in COVID-19 cases has managers in the healthcare system completely baffled.
According to Transparency International, Bangladesh's healthcare management system is becoming more difficult to control as a result of the sudden increase in COVID-19 cases (Transparency International Bangladesh, 2020a). Due to the panic in the administrative body, the healthcare sector is currently experiencing an increasing number of financial corruption instances connected to the COVID-19 issue, which are also exposed by Bangladesh's official news media (print and electronic). It's important to note that the abrupt, unanticipated lockout and the absence of digitalization in the nation's general administrative system both contribute to the disruption in the healthcare sector. Additionally, the healthcare industry has been dealing with significant levels of corruption for a number of decades (Joarder, 2022; Zafarullah & Huque, 2021).
Bangladesh is a developing nation with numerous problems in every area of the government body, including being disorganised, traditional institutional settings, lacking in digitization, insufficient, and even heavily corrupted (Zafarullah & Huque, 2021). The healthcare sector of the country is one of the affected sectors by the above-mentioned issues. Despite these issues, the healthcare sector has the primary duty to care for the enormous number of COVID-19 patients in the context of Bangladesh (Naher et al., 2020). Basu et al. (2023) state that as a great initiative, the government quickly announced 19 incentive packages totalling USD 12.13 billion to help people cope with the pandemic's effects.
However, it is a great dilemma that with the growing national corruption, it is unclear how successful the packages would work (Al-Zaman, 2020). On the other hand, inefficiency had paralyzed the health system, and growing corruption has exacerbated the problem in the sector as well (Basu et al., 2023). Some studies also acknowledge the corruption in the healthcare sector of Bangladesh i.e., the strong presence of corruption in the private and public healthcare sectors of Bangladesh (Shah, 2020), uncontrolled corruption in the pharmaceutical and health care sector (Martinez et al., 2017) and bureaucratic corruption in different sector of Bangladesh including health care sector (Islam & Lee, 2016).
Many studies report that old-fashioned governance systems, lack of digitalization, and poor quality of governance are closely associated with financial corruption in the healthcare sector during COVID-19 (Al-Zaman, 2020). The medical sector is one of the greatest sufferers of the chronic corruption that Bangladeshi institutions have been dealing with for a long time, according to anecdotal evidence, and the situation becomes unstable during the crisis (Alam & Teicher, 2012; Asadullah & Chakravorty, 2019; Abdallah et al., 2022; Zafarullah & Siddiquee, 2001). On the other side, this industry is crucial to the effort to contain the COVID-19 pandemic. Following the COVID-19 attacks around the world, this sector is therefore given a considerably higher priority in budgetary allocation, including Bangladesh (Mohiuddin, 2021).
However, this budgetary prioritization and COVID-19-linked financial activities create new opportunities for corruption as well. Moreover, primary lockdown panic, consequent mismanagement, existing corruption including nepotism and bribery in the sector, and extreme profiting psychology aggravate the situation and ultimately open the door of financial corruption during the primary stage of COVID-19 in Bangladesh. However, these financial activities connected to COVID-19 and the budgetary priorities also open up new chances for corruption. Additionally, the initial lockdown panic, the subsequent poor management, the sector's inherent corruption, including nepotism and bribery, and extreme profit-driven psychology exacerbated the situation and ultimately paved the way for financial corruption during the initial stage of COVID-19 in Bangladesh.
Therefore, news disclosure by mainstream news media on the issue as well as the existing corruption in the healthcare sector inspires us to conduct the current study. The study aims to explore the financial corruption in the healthcare sector related to COVID-19 management during the COVID-19 pandemic in the context of Bangladesh. Besides, the study also explores the relevant causes of financial corruption in the healthcare sector of the country.
The number of existing study gaps on the issue in the context of Bangladesh motivates us to conduct the current study. Reportedly, studies mostly focus on the COVID-19 issues of Bangladesh, i.e. socio-economic crisis due to COVID-19 in Bangladesh (Bodrud-Doza et al., 2020); mental health of children during the lockdown (Yeasmin et al., 2020); mental health of the adult citizen in Bangladesh during COVID-19 (Banna et al., 2022); lockdown scenario in Bangladesh (Shammi et al., 2021), medical service and COVID-19 in Bangladesh (Ahmed et al., 2022; Hossain et al., 2020; Islam et al., 2020) and so on. However, these studies mostly overlooked the financial corruption issue during COVID-19 in the context of Bangladesh. Besides, the mentioned studies also ignore the causes of financial corruption in the healthcare sector of Bangladesh. Therefore, this current study sheds light on the financial corruption that happened during the COVID-19 pandemic in the healthcare sector of Bangladesh. Besides, the study also highlights the relevant causes of financial corruption in the healthcare sector of the country.
The remainder of our paper is structured as follows. Section 2 contains the methodology of the study. Section 3 demonstrates the cases related to the issue published by the mainstream news media. Section 4 provides a discussion of the study and section 5 concludes the study along with some policy implications and several recommendations for further research.
Methodology
Cases for this study were gathered from the news articles published in Bangladesh's major newspapers between March 2020 and June 2021 using content analysis as a methodology. Additionally, a few cases were also gathered from the disclosure made by international organizations operating in Bangladesh. The selected newspapers, however, are Bangladesh's leading news agencies, and they are all well-known throughout the country because of their substantial internet presence. the majority of news media, nevertheless, typically published news in the Bengali language, as the study translates the notions of the relevant news in English as the cases.
In addition, we initially looked through the news media's web version to gather relevant cases. Then, the cases were chosen after being subjected to a reliability check in several well-known Bangladeshi newspapers about the same topic. Although the study mainly references one newspaper for each specific instance. Moreover, the selected cases were the talk of the topic in the country at the time, and the stories were reported by many Bangladeshi mainstream news outlets.
Cases
Due to generating thousands of fake COVID-19 negative test results, law enforcement agencies in Bangladesh shut down two branches of Regent Hospital on July 8, 2020, and arrested the proprietor. Reportedly, only 4,200 of the 10,500 tests performed by both hospitals were genuine, and 6,300 of the test results were fraudulent. According to the news, the hospital charged 3,500 BDT, or $41, for each test and made a profit of over 3.5 crore BDT (($0.41 million).41 million) till the investigation date. Nevertheless, the government and the hospital had a deal in place for the hospital to provide COVID-19 tests free of charge. On the other side, the hospital's license also ran out in 2014 and was never renewed. Additionally, a number of expats used this false certificate to enter a number of countries, and some of them tested positive when they arrived at their destinations (The Daily Star, 2020a).
: On July 13, 2020, the Directorate General of Health Services (DGHS) of Bangladesh revoked JKG Health Care, the sister concern of the OVAL group, from providing the COVID-19 test due to test fraud. They had been gathering samples of COVID-19 and issuing fake certificates at exorbitant prices. While denying the allegations in large part, the organization's chairman and the OVAL group's chairman were found to have provided false information to authorities throughout the course of their thorough interrogation. Interestingly, the chairman of JKG is also a government-registered doctor who is legitimately unable to be a chairman of a private organization by the government officials' law of the country. Furthermore, police arrested several JKG technicians red-handed with the fake COVID-19 certificate creating types of machinery and duplicate official pads of the DGHS. The organization had been charging 5,000 BDT ($59) for each test from the local people and $100 from the international (The Daily Star, 2020b). According to the police file, the organization has issued 27,000 COVID-19 certificates and misappropriated BDT 80 million (almost $1 million) (about USD1 million) (New Age, 2020a; UNB, 2020).
: On July 19, 2020, a law enforcement agency conducted a raid at Shahabuddin Medical College Hospital in the diplomatic area of Bangladesh's capital as part of routine COVID-19 test scrutiny in hospitals. The police discovered a number of blatant discrepancies in the COVID-19 test throughout the raid. First, the hospital had been utilizing an unapproved kit for antibody testing while charging patients 10,000 BDT (about USD 118). Second, they had been purposefully providing positive test results and administering unneeded ICU care in order to take advantage of the COVID-19 scare and make quick profits. Lastly, issuing fake test certificates without really administering a COVID-19 test. Moreover, the hospital treats patients with outdated medical and pharmaceutical equipment (New Age, 2020b; Shothik Shongbad, 2020). As a result, police detained the hospital's owner and closed it down. In addition, they moved the patients to a different hospital right away. Additionally, according to the article, the hospital generates a sizable profit from offering such unsuitable COVID-19 health services, though the newspaper doesn't provide a specific amount of this corruption.
: According to reports, the proprietor of Aparajita International, a provider of medical equipment, was detained on July 25, 2020, for allegedly providing a duplicate N95 mask to Bangabandhu Sheikh Mujib Medical University (BSMMU). On May 27, COVID-19 testing was initially initiated by this public hospital. As a result, the hospital administration came to an arrangement with Aparajita International to buy the N-95 mask in order to ensure that hospital staff have proper protection from infection. 11,000 N95 masks were periodically given by the provider starting on June 30th. The hospital's administration claims via newspaper that they have detected a discrepancy in the quality of masks from the first two batches of deliveries. The authority then formed an investigating committee to conduct a quality check, which revealed that the masks were of poor quality and even had the brand name of the mask misspelt on them. Additionally, they confirm distinguishable discrepancies between the delivered product and the ordered product on the websites of the producers. Therefore, the issue has been handed over to the law enforcement agency for further investigation. However, the remaining masks were counterfeit, with the exception of the initial two deliveries, which totalled 1760 (New Nations, 2020).
On 30 June 2020 the Doinik Ittefaq, reports that Dhaka Medical College Hospital is accused of obtaining BDT 200 million (USD 2.38 million) from the COVID-19 budget allotment. The hospital authority discloses that the budget has been spent on food supplies for the doctors, nurses, and workers in the COVID-19 units of the hospital for the last two months. The hospital authority confirms that around 2000 doctors, nurses, and workers have been working in the units. However, the expenditure is highly disproportionate in the context of Bangladesh and the Prime Minister of the country herself has raised questions about this expenditure and expressed concern about the issue. According to experts via newspapers, the hospital authorities and other administrative entities within the healthcare industry would have been linked to the accusation. However, the story is covered by the majority of the nation's mainstream news outlets. As a result, after the incident, the Bangladesh Anti-Corruption Commission was selected to conduct an inquiry (Daily Ittefaq, 2020).
Discussion
Similar to other nations in the early stages of infection, the Bangladesh government has put strict measures in place to minimize the spread of the COVID-19 virus through prevention and detection methods. To halt or delay the spread, a significant amount of funds, approximately BDT330 billion (about USD4 billion) has been allocated to the health sectors in Bangladesh alone. Through electronic and print media, the government started educating the populace about the COVID-19 guidelines and requirements that the World Health Organization (WHO) had suggested (Shomoy News, 2020a; Transparency International Bangladesh, 2020a). At the same time, the government announced a significant budget to fight the COVID-19 epidemic with the assistance of its development partners despite having a weak economy (BBC Bangla, 2020a; Transparency International Bangladesh, 2020a; US Embassy BD, 2020).
In Bangladesh, the highly contagious COVID-19 pandemic was under control until the end of March 2020 (BBC Bangla, 2020b). Primarily the government only allows public hospitals to provide COVID-19-related healthcare services (Chatterjee & Hazarika, 2020; Chowdhury et al., 2021). In the meantime, the number of cases was increasing rapidly, and it was hard to provide health services only by the public hospitals. Therefore, the government came to a consensus that allowing private hospitals for COVID-19 tests and treatment without taking any charge from the patients to increase the number of tests as well as to expand the accessibility of COVID-19 tests and treatment (Shomoy News, 2020b). Reportedly, as a highly populated country with relatively weak healthcare service, the government turned private hospitals into the COVID-19 service hospitals list, so that people can avail of the service quickly.
In spite of this, the government had pledged to generously compensate private hospitals for the support they had given throughout the pandemic (BBC Bangla, 2020c). According to prior studies, greater government projects reportedly have greater budgets, which also raises the likelihood of significant corruption (Magtulis & Poquiz, 2017). Therefore, unethical individuals and organizations involved in the projects take advantage of this chance to use their expertise in rent-seeking to reroute the flow of this fund to their own pockets. However, the current study is able to connect the corruption that occurred in the healthcare industry during the COVID-19 epidemic with the country's overall corruption culture as shown by earlier studies.
Additionally, studies affirm that poor quality of governance facilitates corruption and interrupts the effectiveness of institutions, where institutions of Bangladesh have been experiencing these issues for the past several decades (Knox, 2009). The Worldwide Governance Indicators (WGI) displays the worldwide quality of governance index where Bangladesh scores only 0.417 one of the lowest in the world and Finland scored 0.973 as highest in 2018 (Baniamin, 2019). Ahmed et al. (2017) find that the healthcare sector of Bangladesh is highly corrupt, and patients are barely satisfied with the service. Similarly, Chaudhury et al. (2006) acknowledge that corruption and patient harassment are usual issues in the healthcare sector of Bangladesh. Al-Zaman (2020) states that the Bangladesh government announced a huge budget for the healthcare sector to fight against the COVID-19 pandemic but existing corruption in this sector would be the prime challenge to utilising this fund efficiently. The study also identifies financial corruption intensifying in the healthcare sector because of poor governance during COVID-19 and supports fund leakage from the allocation.
According to Desh Rupantor (2020), dishonest healthcare officials in the nation cultivate patron-client relationships both inside and outside for the purpose of obtaining illicit reciprocal benefits from the sector. Additionally, law enforcement agencies frequently fail to take appropriate action against these persistent corruptions in the health sector. On the other hand, if a government official engages in this wrongdoing, the law only imposes mild penalties, such as temporary expulsion or transfer to another office, which indirectly contributes to swelling the corruption in this sector as well (Desh Rupantor, 2020).
According to Naher et al. (2020), there are a number of variables, such as inadequate management, a lax accountability system, nepotism, syndicates, bribery, and gaps in the legal and justice systems, that contribute to the healthcare sector's brittleness and recurrent financial mismanagement. The study also acknowledges that these issues in the healthcare system are mostly similar in South Asian countries and some countries are overcoming the problem, but Bangladesh is still struggling.
According to a group of research, the people of Bangladesh are heavily reliant on privately owned medical services (Ahmed et al., 2017; Rahman, 2020). In order to increase their revenue, the private healthcare industry acts as a pressure-creating organization and manipulates government medical policy (Rahman, 2020). The study also acknowledges that the government's ongoing indifference to public hospitals and inadequate funding over the years has strengthened the influence of the syndicate of private hospitals in the health care system of the country. The mismanagement and financial fraud of the COVID-19 fund during the first stage of the pandemic, however, was a result of the aforementioned problems in Bangladesh's healthcare system.
The discussed studies confirm that private healthcare facilities are getting rainless day by day. Even during a pandemic, the discussed cases mostly occur in privately owned hospitals and healthcare-related organizations. However, it implies that myopia in the public health sector, low health budget, high out-of-pocket expenditure, and influential private health sector mutually contribute to aggravating such mismanagement and financial corruption in the healthcare sector of the country during COVID-19. Besides, weak national governance history, sluggish bureaucracy, un-digitalized healthcare governance and the sudden COVID-19 spikes and panic also contribute to the stated cases in the healthcare sector of Bangladesh.
Mietzner (2020) discovers an identical response to COVID-19 management from the Indonesian healthcare sector. The study shows the pandemic has opened the door to huge corruption in the healthcare sector of Indonesia through embezzlement from the COVID-19 social assistance packages and medical assistance packages. The corruption scenarios in the healthcare sector are almost identical in most developing countries (Bhuiyan et al., 2021; Mietzner, 2020; Ruiz Estrada, 2020). Transparency International Bangladesh (TIB) reports that every component of good governance is directly linked to the COVID-19 battle, in which Bangladesh is performing poorly from the perspectives of the rule of law, government effectiveness, control of corruption, and accountability perspective (Transparency International Bangladesh, 2020b). Furthermore, the report also indicates that this situation might facilitate huge corruption in the healthcare sector of the country amid COVID-19.
The communication gap among inter-departments of the government also inspires corruption and mismanagement in the health sector of Bangladesh during COVID-19 (Al-Zaman, 2020). The study also notes that during the early COVID-19 strikes, there were widespread rumours, pandemic-related uncertainty, weak information security, and a dearth of trustworthy information sources on the matter, all of which fuelled healthcare mismanagement and helped spark corruption in the healthcare sector. Alam (2020) states that a lack of digital skills in the health sector administration, inadequate logistics and old-fashioned administration contribute to healthcare sector mismanagement.
The existing laws of the country consider this type of conduct stated in the cases, but old laws had some loopholes to punish the corrupt (Naher et al., 2020). Therefore, the country amended the laws in 2014 to control the reins of corruption, i.e., the Whistle Blower Protection Act, the Ombudsman Act, and the Prevention of Corruption Act, which guaranteed the security of informants about corruption and determined the punishment for professional misconducts and embezzlement of money through different illegal channels. The cases of the current study demonstrate that there are still many incidents of corruption in the public sector of Bangladesh despite the existence of robust laws against it. Naher et al. (2020) also imply that the implementation of the existing laws has some limitations due to the insufficient ability of law-enforcement authorities to investigate complaints against government officials. Moreover, Additionally, it is challenging to conduct an investigation against influential political figures, who frequently own the majority of private hospitals. So, these issues might be the reasons for the mismanagement and high corruption in the healthcare sector discussed in the cases of this study.
The Bangladeshi government made a positive effort to address COVID-19 concerns, according to the current study, but this effort has been waning as a result of the prevalence of corruption in the healthcare sector. The discussed cases are closely related to overall poor governance in the country, existing corruption in the health sector, limitations on the law and justice process, shaky system of punishment due to corruption, lack of digitization in healthcare administration, and preponderance of reliance on private hospitals. A number of previous studies on the issue also confirm the findings of the current study (Khemani, 2020; Mietzner, 2020; Ruiz Estrada, 2020).
Conclusion
The study explores the financial corruption in the healthcare sector of Bangladesh during COVID-19 based on the case studies published in the mainstream news media of the country. Primarily Bangladesh, like most countries, has provided a significant amount of fund allocation to its health care sector, a total of BDT330 billion equivalent to USD4 billion to fight against the pandemic. Besides, the dishonest individuals in this industry are also given some significant possibilities by this large expenditure. Mainstream news media of the country disclose several events on financial corruption in COVID-19 management in the healthcare sector of the country, i.e., purchasing fake masks in cheap for misappropriation of allocated money, providing fake COVID-19 test certificates, imposing a high charge on COVID-19 tests, and so on during the primary stage of infection.
The study finds that the discussed corruption in the healthcare sector of Bangladesh is highly associated with poor quality of governance, traditional administrative structure, overall weak law and justice system, a weak punishment system due to corruption, poor digitalization in the administration in healthcare management contributes for the corruption during the COVID-19 pandemic. Furthermore, the study also finds that the panic during the initial COVID-19 outbreak in Bangladesh degraded the country's entire administration, especially the administration of the health care system, which encourages corruption by unethical actors.
According to the report, there are still many corruption loopholes in the healthcare service of the country, and the pandemic is far from being over and even another pandemic or crisis might strike in the near future. Therefore, policymakers could identify how to address financial misconduct in the healthcare industry through the study. Besides, policymakers can benefit from this study in order to close the corruptive loopholes in the healthcare sector and strengthen the current administration or future policymaking.
Reportedly, Bangladesh's healthcare sector has been dealing with various forms of corruption for a while, but this study only considers the primary stage of the COVID-19 pandemic into account. Therefore, additional research can focus on case studies, surveys, or secondary data to examine the impact of other corruption, sluggish digitalization, and administrative structure in this sector over the long and short term.
References
Abdallah, W., Chowdhury, S., & Iqbal, K. (2022). Access and fees in public health care services for the poor: Bangladesh as a case study. Oxford Development Studies, 50(3), 209-224. DOI:
Ahmed, O., Ahmed, M. Z., Alim, S. M. A. H. M., Khan, M. D. A. U., & Jobe, M. C. (2022). COVID-19 outbreak in Bangladesh and associated psychological problems: An online survey. Death Studies, 46(5), 1080-1089. DOI:
Ahmed, S., Tarique, K. M., & Arif, I. (2017). Service quality, patient satisfaction and loyalty in the Bangladesh healthcare sector. International Journal of Health Care Quality Assurance, 30(5), 477-488. DOI:
Alam, M. A. (2020). Leading in the shadows: understanding administrative leadership in the context of COVID-19 pandemic management in Bangladesh. International Journal of Public Leadership, 17(1), 95-107. DOI:
Alam, Q., & Teicher, J. (2012). The state of governance in Bangladesh: The capture of state institutions. South Asia: Journal of South Asian Studies, 35(4), 858-884. https://www.tandfonline.com/doi/abs/
Al-Zaman, M. S. (2020). Healthcare Crisis in Bangladesh during the COVID-19 Pandemic. The American Journal of Tropical Medicine and Hygiene, 103(4), 1357-1359. DOI:
Andaleeb, S. S., Siddiqui, N., & Khandakar, S. (2007). Patient satisfaction with health services in Bangladesh. Health Policy and Planning, 22(4), 263-273. DOI:
Asadullah, M. N., & Chakravorty, N. N. T. (2019). Growth, governance and corruption in Bangladesh: a re-assessment. Third World Quarterly, 40(5), 947-965. DOI:
BanglaNews24.com. (2020). Corona test fee of 200 BDT (In Bangla). Retrieved on February 14, 2021, from https://www.banglanews24.com/national/news/bd/796967.details
Baniamin, H. M. (2019). Linking socio-economic performance, quality of governance, and trust in the civil service: does culture intercede in the perceived relationships? Evidence from and beyond Bangladesh, Nepal and Sri Lanka. Asia Pacific Journal of Public Administration, 41(3), 127-141. DOI:
Banna, M. H. A., Sayeed, A., Kundu, S., Christopher, E., Hasan, M. T., Begum, M. R., Kormoker, T., Dola, S. T. I., Hassan, M. M., Chowdhury, S., & Khan, M. S. I. (2022). The impact of the COVID-19 pandemic on the mental health of the adult population in Bangladesh: a nationwide cross-sectional study. International Journal of Environmental Health Research, 32(4), 850-861. DOI:
Basu, A. M., Basu, K., & Tapia, J. M. U. (2023). The complexity of managing COVID-19: How important is good governance?. In Managing Pandemic and Correcting Development Fundamentals: India’s Great Challenge. Singapore: Springer Nature Singapore. DOI:
BBC Bangla. (2020a). Coronavirus: What does Bangladesh have to take from the countries that can deal with it (In Bangla). Retrieved on September 21, 2020, from https://www.bbc.com/bengali/news-51877284
BBC Bangla. (2020b). Coronavirus: One month after the first patient was identified, where does Bangladesh stand? (In Bangla). Retrieved on September 21, 2020, from https://www.bbc.com/bengali/news-52207223
BBC Bangla. (2020c). Coronavirus: Experts say to include private hospitals for coronavirus treatment (In Bangla). Retrieved on September 21, 2020, from https://www.bbc.com/bengali/news-52700041
Bhuiyan, A. K. M. I., Sakib, N., Pakpour, A. H., Griffiths, M. D., & Mamun, M. A. (2021). COVID-19-Related Suicides in Bangladesh Due to Lockdown and Economic Factors: Case Study Evidence from Media Reports. International Journal of Mental Health and Addiction, 19(6), 2110-2115. DOI:
Bodrud-Doza, M., Shammi, M., Bahlman, L., Islam, A. R. M. T., & Rahman, M. M. (2020). Psychosocial and Socio-Economic Crisis in Bangladesh Due to COVID-19 Pandemic: A Perception-Based Assessment. Frontiers in Public Health, 8. DOI: 10.3389/fpubh.2020.00341
Chatterjee, A., & Hazarika, D. D. (2020). Corporate Governance Deviance: A Case Study of Infosys. South Asian Journal of Business and Management Cases, 9(2), 247-258. DOI:
Chaudhury, H., Mahmood, A., & Valente, M. (2006). Nurses' perception of single-occupancy versus multioccupancy rooms in acute care environments: An exploratory comparative assessment. Applied Nursing Research, 19(3), 118-125. DOI:
Chookajorn, T., Kochakarn, T., Wilasang, C., Kotanan, N., & Modchang, C. (2021). Southeast Asia is an emerging hotspot for COVID-19. Nature Medicine, 27(9), 1495-1496. DOI:
Chowdhury, S. R., Sunna, T. C., & Ahmed, S. (2021). Telemedicine is an important aspect of healthcare services amid COVID-19 outbreak: Its barriers in Bangladesh and strategies to overcome. The International Journal of Health Planning and Management, 36(1), 4-12. DOI:
Daily Ittefaq. (2020). How only food bill can be 20 crores in Dhaka Medical: Prime Minister (In Bangla). Retrieved on April 08, 2021, from https://www.ittefaq.com.bd/national/162316/%E0%A6%A2%E0%A6%BE%E0%A6%95%E0%A6%BE-
Desh Rupantor. (2020). Where is the corruption in the health sector driving us (In Bangla). Retrieved on September 21, 2020, from https://www.deshrupantor.com/editorial-news/2020/07/20/233272
Hossain, M. M., Mazumder, H., Tasnim, S., Nuzhath, T., & Sultana, A. (2020). Geriatric Health in Bangladesh during COVID-19: Challenges and Recommendations. Journal of Gerontological Social Work, 63(6-7), 724-727. DOI:
Islam, A., & Lee, W.-S. (2016). Bureaucratic Corruption and Income: Evidence from the Land Sector in Bangladesh. The Journal of Development Studies, 52(10), 1499-1516. DOI:
Islam, M. S., Sujan, M. S. H., Tasnim, R., Sikder, M. T., Potenza, M. N., & van Os, J. (2020). Psychological responses during the COVID-19 outbreak among university students in Bangladesh. PLOS ONE, 15(12), e0245083. DOI:
Joarder, T. (2022). Everyday Life in a Hybrid Regime: The Case of Health Sector in Bangladesh with a Focus on COVID-19 Pandemic. Masks of Authoritarianism. DOI:
Khemani, S. (2020). An Opportunity to Build Legitimacy and Trust in Public Institutions in the Time of COVID-19. DOI:
Knox, C. (2009). Dealing with sectoral corruption in Bangladesh: Developing citizen involvement. Public Administration and Development, 29(2), 117-132. DOI:
Magtulis, P. P., & Poquiz, J. L. (2017). Big Government, Big Corruption? Examining the Relationship between Government Size and Public Corruption in the Philippines. International Journal of Public Administration, 40(11), 954-967. DOI:
Martinez, M. G., Kohler, J. C., & McAlister, H. (2017). Corruption in the Pharmaceutical Sector. The Handbook of Business and Corruption. DOI:
Mietzner, M. (2020). Populist Anti-Scientism, Religious Polarisation, and Institutionalised Corruption: How Indonesia's Democratic Decline Shaped Its COVID-19 Response. Journal of Current Southeast Asian Affairs, 39(2), 227-249. DOI:
Mohiuddin, A. K. (2019). Diabetes fact: Bangladesh perspective. International Journal of Diabetes Research, 2(1), 14-20.
Mohiuddin, A. K. (2021). An Extensive Review of Health and Economy of Bangladesh Amid Covid-19 Pandemic. IJHCM (International Journal of Human Capital Management), 5(1), 12-27. DOI:
Naher, N., Hoque, R., Hassan, M. S., Balabanova, D., Adams, A. M., & Ahmed, S. M. (2020). The influence of corruption and governance in the delivery of frontline health care services in the public sector: a scoping review of current and future prospects in low and middle-income countries of south and south-east Asia. BMC Public Health, 20(1). DOI:
New Age. (2020a). Sabrina lands in jail, ACC seeks her info from 4 authorities. Retrieved on September 26, 2020, from https://www.newagebd.net/article/111636
New Age. (2020b). Shahabuddin hospital to be sealed off: RAB. Retrieved on September 20, 2020, from https://www.newagebd.net/article/111563/shahabuddin-hospital-to-be-sealed-off-rab
New Nations. (2020). DU assistant registrar Sharmin detained over supplying fake N95 masks. Retrieved on September 20, 2020, from http://m.thedailynewnation.com/news/258797
Rahman, R. (2020). Shrinking the state: the rise of private sector healthcare in Bangladesh. Journal of International Development, 32(5), 717-726. DOI:
Ruiu, M. L. (2020). Mismanagement of COVID-19: lessons learned from Italy. Journal of Risk Research, 23(7-8), 1007-1020. DOI:
Ruiz Estrada, M. A. (2020). Can COVID-19 Generate a Massive Corruption in Developing Countries and Least Developed Countries?. DOI:
Shah, M. F. (2020). Private health care, quality and corruption. In Biomedicine, healing and modernity in rural Bangladesh (pp. 125-165). Palgrave Macmillan, Singapore. DOI:
Shammi, M., Bodrud-Doza, M., Islam, A. R. M. T., & Rahman, M. M. (2021). Strategic assessment of COVID-19 pandemic in Bangladesh: comparative lockdown scenario analysis, public perception, and management for sustainability. Environment, Development and Sustainability, 23(4), 6148-6191. DOI:
Shomoy News. (2020a). What is Bangladesh doing to deal with Corona (In Bangla). Retrieved on September 20, 2020, from https://www.somoynews.tv/pages/details/211089
Shomoy News. (2020b). Corona can be tested in 17 private hospitals (In Bangla). Retrieved on September 21, 2020, from https://www.somoynews.tv/pages/details/215159
Shothik Shongbad. (2020). Coronavirus test fraud: Case against Sahabuddin Medical College, three arrested (In Bangla). Retrieved on September 20, 2020, from https://www.benarnews.org/bengali/news/coronavirus-07202020162903.html
The Daily Star. (2020a). DGHS orders shutdown of pvt hospital. Retrieved on September 20, 2020, from https://www.thedailystar.net/frontpage/news/dghs-orders-shutdown-pvt-hospital-1926733
The Daily Star. (2020b). JKG Health Care: Dr Sabrina held over fake Covid certificates. Retrieved on September 20, 2020, from https://www.thedailystar.net/frontpage/news/jkg-health-care-dr-sabrina-held-over-fake-covid-certificates-1929433
Transparency International Bangladesh. (2020a). Lack of planning and coordination worsen Corona Virus situation in Bangladesh, finds study. Retrieved on September 21, 2020, from https://www.ti-bangladesh.org/beta3/index.php/en/activities/6096
Transparency International Bangladesh. (2020b). COVID-19 crisis response and recovery: TIB calls upon international donors to provide unprecedented level of support to Bangladesh and ensure highest standards of transparency and accountability. Retrieved on September 21, 2020, from https://www.ti-bangladesh.org/beta3/index.php/en/activities/6061
UNB. (2020). Fake COVID-19 certificates: Charges framed against Sabrina, 7 others. Retrieved on September 26, 2020, from https://unb.com.bd/category/bangladesh/fake-COVID-19-certificates-charges-framed-against-sabrina-7-others/56270
Yeasmin, S., Banik, R., Hossain, S., Hossain, M. N., Mahumud, R., Salma, N., & Hossain, M. M. (2020). Impact of COVID-19 pandemic on the mental health of children in Bangladesh: A cross-sectional study. Children and youth services review, 117, 105277. DOI:
Zafarullah, H., & Huque, A. S. (2021). Corruption and its Control: The Pursuit of Probity in Bangladesh. In Corruption in the Public Sector: An International Perspective. Emerald Publishing Limited. DOI:
Zafarullah, H., & Siddiquee, N. A. (2001). Dissecting public sector corruption in Bangladesh: issues and problems of control. Public Organization Review, 1(4), 465-486. DOI:
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
15 November 2023
Article Doi
eBook ISBN
978-1-80296-130-0
Publisher
European Publisher
Volume
131
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-1281
Subjects
Technology advancement, humanities, management, sustainability, business
Cite this article as:
Musa, K., Said, J., Zakaria, N. B., Begum, F., & Jamaluddin, A. (2023). Financial Corruption in the Healthcare Sector of Bangladesh During Covid-19 Pandemic. In J. Said, D. Daud, N. Erum, N. B. Zakaria, S. Zolkaflil, & N. Yahya (Eds.), Building a Sustainable Future: Fostering Synergy Between Technology, Business and Humanity, vol 131. European Proceedings of Social and Behavioural Sciences (pp. 59-71). European Publisher. https://doi.org/10.15405/epsbs.2023.11.5