
Illness Beliefs Among Adolescents With Hiv


Abstract
This study investigated illness beliefs among adolescents with chronic illnesses. These beliefs were compared between adolescents with HIV (
Keywords: Adolescentscompliancecystic fibrosisHIVillness beliefs
Introduction
This study investigates cognitive beliefs about illness, worries of disease progression and patient compliance among HIV-infected adolescents. In this study patient compliance is defined as the degree to which patient’s behavior corresponds physician’s medical advice, including medications intake, diet and/or lifestyle changes (Moiseeva & Viktorova, 2018).
The topic of this study is highly relevant, since HIV is a global pandemic, despite the efforts of World Health Organization, UNAIDS and national health care systems to control it. According to UNAIDS, 37.9 million of people worldwide had HIV in 2018. 24.5 million of people received antiretroviral therapy treatment in July 2019. Every week 6000 young women from 15 to 24 years old are infected with HIV. 728.2 of 100.000 of people in Russia were infected with HIV in December 2019.
Problem Statement
Models explaining illness beliefs develop extensively in psychological research. Researchers emphasize the role of illness beliefs in adjustment and psychological well-being of patients (Beck et al., 1979; Leventhal et al., 1984). There are five key domains of illness perceptions according to Leventhal’s Self-Regulatory Model: identity (symptoms of the illness), cause (beliefs about the factors which cause the illness), consequences (expected results of the treatment and its consequences), timeline (beliefs about the duration of the illness) and control/cure (Weinman et al., 1996). This model allowed to reveal that beliefs about illness control are related to problem-oriented strategies, while avoidance strategies are related to beliefs about chronic timeline of the illness, lack of illness understanding and many clinical symptoms.
Researchers notice a similar structure of illness beliefs towards different chronic diseases (Schiaffino & Cea, 1995). The loss of disease control is related to helplessness, hopelessness, which in long-term perspective cause difficulties in patients’ adjustment. Positive cognitive constructs imply higher potential to adjust to the illness and more efficient coping strategies. Acceptance of chronic duration of the disease, together with the knowledge about the strategies to overcome its consequences, decrease negative impact of stress (Hayes et al., 1996).
In Russian psychology the model of worries about the disease progression was developed by Sirota and Moskovichenko (2014). This model describes worries about the disease progression as a construct which includes three levels. The first level is cognitive, it includes beliefs and thoughts about the disease progression. The second level is emotional, it includes emotional reactions, such as fear of autonomy loss, fears related to family functioning. The third level is behavioral, it includes preserving behavior. Perception of the threat of disease progression lies on two poles of the continuum: cognitive evaluation of disease progression control and cognitive evaluation of disease progression threat.
Research Questions
There is a lack of studies of cognitive beliefs about illness among adolescents with HIV in Russian clinical psychology. Studies of illness beliefs can contribute to our understanding of the intellectual level of illness perceptions, disease evaluation and coping processes.
Purpose of the Study
The aim of this study is to investigate the structure and content of worries of disease progression among adolescents with HIV. We test the following hypothesis: 1. Anxiety as a domain of illness perception is developed less among patients with HIV as opposed to patients with cystic fibrosis. 2. Worries about disease progression lie on a continuum of different illness beliefs among patients with HIV and cystic fibrosis. 3. Cognitive evaluation of the threat of disease progression is related to maladaptive illness beliefs.
Research Methods
Thirty-three adolescents with HIV and cystic fibrosis took part in the study. Adolescents aged 14-15 years old (mean age 14.6) were included in the clinical group. All participants are under the care of the charity foundation “Children +”. All adolescents were infected with HIV via the mother-to-child transmission; they received antiretroviral therapy more than 8 years. Because of the difficulties related to recruiting families with HIV-infected adolescents, we recruited only 19 participants from 13 to 17 years old (mean age 14.6 years old, 11 boys, 8 girls). Fourteen adolescents from 13 to 15 years old (9 boys, 5 girls, mean age 14.6 years old) were included in the control group. All these adolescents were diagnosed with cystic fibrosis – a genetic somatic disorder.
All adolescents were treated at the pediatric department at the RCCH the Russian children's clinical hospital. All participants completed the following questionnaires:
1. Semi structured interview which included questions about autobiographical information related to family situation, illness beliefs about HIV and its treatment in general.
2. To assess the types of illness beliefs we used clinical test Type of Person’s Attitude to the Disease (TAD) developed at the Bekhterev Psychoneurological Research Institute (Vasserman et al., 1987). In includes 12 types of illness attitudes, developed by A.E. Lychko and N.Y. Ivanov: harmonic, ergopathic, anosognostic, anxious, hypochondriac, neurasthenic, melancholic, apathic, sensitive, egocentric, paranoiac and dysphoric. These attitudes towards the illness are combined in three blocks. First block includes harmonic, ergopathic and anosognostic attitudes. Social and psychological adjustment to an illness is not gravely disturbed because of these attitudes. Second block includes attitudes towards illness which have intrapsychic direction of reaction towards an illness, which causes disturbances in social adjustment among patients: neurasthenic, anxious, hypochondriac, melancholic and apathic. The third block of attitudes is related to interpsychic direction of reaction towards an illness and is related to disturbances of social adjustment.
3. Model of worries of disease progression developed by Sirota and Moskovchenko (2014). This model describes worries about disease progression as a construct which includes several levels. First level is cognitive, it includes thoughts about disease progression. Second level is emotional, it includes emotional reactions, fear of autonomy loss, fears related to family functioning. Behavioral level includes preserving behaviors. Disease progression threat perception includes two poles of a continuum: cognitive evaluation of disease progression control and cognitive evaluation of disease progression threat.
4. Morisky-Green Scale (Morisky et al., 1986) is a widely spread scale to measure compliance to different somatic and mental disorders.
Data analysis was conducted in SPSS 23.0 and included factor analysis, between-participants comparisons (the Mann–Whitney test). Significance level was set to p = 0.05.
Findings
Attitudes towards illness among adolescents with HIV
Factor analysis (principal components analysis) with normalized varimax revealed several types of illness attitudes among adolescents. Among adolescents with HIV we found four semantic categories, while among adolescents with cystic fibrosis – three (see Table
We compared types of illness attitudes among adolescents with HIV and cystic fibrosis. Significant differences were found in anxious attitude type, according to Mann–Whitney test (p < 0.05). Results of comparisons are illustrated in Table
Adolescents with HIV are less inclined to experience continuous worry because of their illness progression and their treatment, as opposed to adolescents with cystic fibrosis. Adolescents with HIV are less included to continuously search for new types of treatment and new information about their illness, as opposed to adolescents with cystic fibrosis. Adolescents with cystic fibrosis are more interested in objective information about illness progression: medial test results, medical specialists’ opinions. They prefer to listen others telling them about their symptoms, rather than demonstrate their own symptoms.
Worries about HIV progression
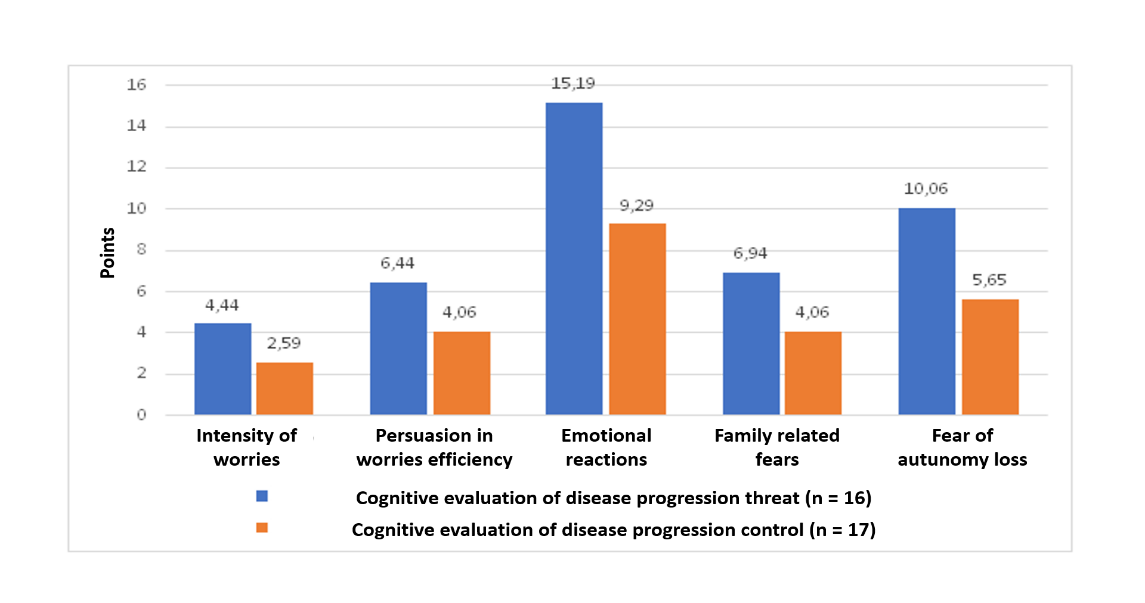
We conducted cluster analysis in order to define types of cognitive evaluation of disease progression among patients with HIV and cystic fibrosis. The number of clusters was based on the model which includes two poles of cognitive evaluation. We conducted cluster analysis using K-means clustering. The results are illustrated in Figure
First cluster of “cognitive evaluation of the threat of disease progression” included 16 patients. The second cluster of “cognitive evaluation of the control of disease progression” included 19 patients.
As seen in Image 1, patients which were included in the first cluster were characterized by a higher level of intensity of thoughts about the disease progression. They were persuaded in effectiveness of worrying about disease progression, which was related to their need to control the disease.
Emotional component of worries about disease progression was significantly higher among patients from the first cluster. When receiving prescriptions about medical consultations and exams these patients experienced intensive emotional reactions, which expressed themselves in fear of pain, vegetative reactions of anxiety and anxiety that treatment might cause irreversible consequences. Moreover, patients from this cluster experienced higher level of fear of autonomy loss, which expressed itself in worries about potential independence loss and not being able to perform daily activities. Patients included in the first cluster had more intensive fears for their families, which were expressed in their worries to transfer the disease to their children, as well as worries for their close ones.
Patients from the first cluster were characterized by low level of worries about the HIV or cystic fibrosis progression. They are also characterized by not being persuaded that their worrying is effective. These patients have low level of emotional reactivity about the disease and its treatment. There were no statistically significant differences in behavioural component.
Analysis of types of attitudes towards illness showed that the group of patients with cognitive evaluation of disease progression threat includes patients with the following continuum of attitudes: anxious, neurasthenic, sensitive and egocentric. The second cluster includes patients with less intensive anxiety and neurasthenia, as well as sensitivity and egocentricity. These results are illustrated in Table
Thus, adolescents with more intensive cognitive evaluation of disease progression threat more often have the anxious, depressive and phobic attitudes towards the disease. They are also characterized by intrapsychic direction of reactions about the disease and neurasthenic attitude type. Interpsychic direction of their reactions about the disease is mostly characterized by sensitive and egocentric attitude types.
Morisky-Green Scale Interpretation
We used multiple regression analysis to study the impact of compliance on cognitive evaluation of disease progression as a threat. Regression model was built for negative thinking as dependent variable. We included the data of Morisky-Green Scale in a sample of adolescents with HIV. Results are presented in Table
Multiple regression analysis showed that compliance predicts negative thinking. This model explains 41% of variance of dependent variable (R2 = 0.417).
Conclusion
Attitudes towards illness among adolescents with HIV
We found several semantic categories of attitudes towards illness among adolescents with HIV and adolescents with cystic fibrosis. First category included patients with paranoiac and dysphoric types of attitudes towards illness. They are inclined to accuse people around them in their illness and demonstrate aggressive reactions. Importantly, having a similar interpsychic reaction type patients with HIV and patients with cystic fibrosis have different intrapsychic reaction on their diseases. Patients with HIV are worried about the opinion of people around them, sensitive and anxious, prone to neurasthenia. While patients with cystic fibrosis are more inclined to apathy and melancholy.
The second category included patients with interpsychic reaction of egocentric attitude type and hypochondriac reactions. In this case, there were differences in intrapsychic reaction type among adolescents in two groups. Adolescents with HIV avoided thoughts about their disease, distracted themselves with thoughts about working and studying. They have depressive thoughts, including suicidal thoughts. To the contrary, adolescents with cystic fibrosis have signs of anxiety and neurasthenia. The third category included adolescents with harmonic reaction type. Among adolescents with HIV, harmonic reaction type is related to apathic type of attitudes towards the illness. Which means that they are passive, often rely on their parents, accept all medical prescriptions. While adolescents with cystic fibrosis do not overestimate the severity of their health impairments and are inclined to participate actively in their treatment in order to make it easier for others to take care of them. Often, they can avoid thoughts about the disease and try to keep their social status at all cost, continue succeeding in their school and professional activities. The fourth category included adolescents with anosognosic type of reaction to their disease. It is important to mention that anxious component of disease progression evaluation among adolescents with HIV was less intensive, as opposed to patients with cystic fibrosis.
Worries about HIV progression
Cognitive evaluation of disease progression control was characterized by weakly expressed emotional reaction on treatment and possible loss of autonomy, low intensity of worries about disease progression. Patients with cognitive evaluation of disease progression control had few worries about the way others perceive information about their illness, low level of intensity of anxious, depressive and phobic reactions. Moreover, these patients were not inclined to interpret their illness as a strategy to receive social benefits. Cognitive evaluation of disease progression control was characterized by emotional stability and predictability.
Cognitive evaluation of the threat of disease progression was related to high level of worries intensity and maladaptive stress coping strategies (for instance, persuasion in the efficiency of worrying). They also demonstrated intensive emotional reactions, high level of anxiety, increased interest to objective information about their disease progression, “irritated weakness” behavior type, fear of independence loss and excessive worries about possible negative impressions which others might have because of their illness.
We shall describe a case of an adolescent with HIV who was included in cognitive evaluation of disease progression threat category.
A, 16. “I stopped taking my medications and did not take them for three months. I was tired of taking them. Now I know, that it is important, and never miss my medications. I know the results of my medical tests; I have zero virus load. My condition depends a lot from the way others treat me. I try to make my illness invisible, so others will not mention it. Even me, I am afraid of my diagnosis and try avoid thinking of it. On one side, my disease does not prevent me from having friends, if I won’t tell them about my illness, but on the other side – it dooms me to be lonely. Because of my disease I worry a lot about my future. However, even in the most desperate situations, I always hope for happiness in the future. As a rule, my mood is often good, I don’t let myself to drown in melancholy. I try to ease my family’s efforts to take care of me because of my disease.”
Worries about disease progression lie on a continuum of different attitudes towards disease. Psychological factors which precede cognitive evaluation of disease progression threat are maladaptive attitudes. Our results are in line with Russian studies which find that process of negative evaluation of adjustment is related to the fact the patient perceive their illness as not controllable and unpredictable (Sirota & Moskovichenko, 2014).
The role of compliance in cognitive evaluation of disease progression as a threat
Patients with HIV who have high compliance are inclined to think about their disease progression. Multiple regression analysis showed that the higher is the degree of compliance, the higher are negative, catastrophic mental scenarios among patients.
Our results are in line with Russian and international studies which showed that compliance among men and women is related to their personality traits. These findings are also in line with the hypochondriacal discourse approach which states that excessive valuation of health induces catastrophizing of bodily sensations. Health value is related to different self-preserving behaviors, but also with increased attention towards one’s bodily sensations (Rasskazova et al., 2016).
References
- Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive Therapy of Depression. Guilford Press.
- Hayes, S. C., Wilson, K. W., Gifford, E. V., Follette, V. M., & Strosahl, K. (1996). Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64(6), 1152-1168.
- Leventhal, H., Nerenz, D. R., Steele, D. J. (1984). Illness representation and coping with health treats. In A. Baum, & J. Singers (Eds.), Handbook of psychology and health. (pp. 219-252). Erlbaum.
- Moiseeva, M. V., & Viktorova, I. A. (2018). The Prognosis of Low Adherence to Therapy of Patients with Arterial Hypertension in the Primary Health Care Stage. https://cyberleninka.ru/article/n/prognoz-nizkoy-priverzhennosti-k-terapii-u-patsientov-s-arterialnoy-gipertoniey-na-etape-okazaniya-pervichnoy-mediko-sanitarnoy-pomoschi/viewer
- Morisky, D., Green, L. W., & Levine, D. M. (1986). Concurrent and predictive validity of a self-reported measure of medication adhernce. Med Care, 67-74.
- Rasskazova, E. I., Thostov, A. S., & Gul'dan, V. V. (2016). Sposoby zaboty o zdorov'e i somaticheskie zhaloby v norme: rol' predstavlenij i rol' dejstvij [Health protection and somatic complaints]. Zhurnal Psihologicheskie issledovaniya, 9(50), 1-12.
- Schiaffino, K. M., & Cea, C. D. (1995). Assessing chronic illness representations: The implicit models of illness questionnaire. Journal of Behavioral Medicine, 18(6), 531–548
- Sirota, N. A., Moskovichenko, D. V. (2014). Psihodiagnostika straha progressirovaniya zabolevaniya: -rezul'taty aprobacii russkoyazychnoj versii oprosnika straha progressirovaniya zabolevaniya [Psychodiagnostics of fear of disease progression]. Obozrenie psihiatrii i medicinskoj psihologii imeni V.M. Bekhtereva, 4, 86–91.
- Vasserman, L. I., Iovlev, B. V., Karpova, E. B., Vuks, A. Y. (1987). Type of Person’s Attitude tot he Disease (TAD): a guide for doctors. http://bekhterev.spb.ru/content/42/2005_pdati.pdf
- Weinman, J., Petrie, K. J., Moss-Morris, R., & Horne, R. (1996). The Illness Perception Questionnaire: A new method for assessing the cognitive representation of illness. Psychology & Health, 11(3), 431–445.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
15 November 2020
Article Doi
eBook ISBN
978-1-80296-093-8
Publisher
European Publisher
Volume
94
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-890
Subjects
Psychology, personality, virtual, personality psychology, identity, virtual identity, digital space
Cite this article as:
Pechnikova, L. S., Tokareva, E. D., Zhujkova, E. B., Sirota, N. A., Moscovichenko, D. V., & Gal'cova, P. S. (2020). Illness Beliefs Among Adolescents With Hiv. In T. Martsinkovskaya, & V. Orestova (Eds.), Psychology of Personality: Real and Virtual Context, vol 94. European Proceedings of Social and Behavioural Sciences (pp. 583-590). European Publisher. https://doi.org/10.15405/epsbs.2020.11.02.71