
Reducing Vocal Self-Stimulation In Children With Autism Spectrum Disorders

Abstract
One of the most significant challenges related to the autism spectrum disorder (ASD) condition is the presence of vocal stereotypy which can interfere with learning, auditory processing and desirable social behaviours. Verbal self-stimulation is characterized by repetitive, non-contextual and apparently non-functional phrases, words or noises that are automatically reinforced by sensory auditory consequences. Delayed echolalia is one of the most frequent types of vocal self-stimulation in children with ASD. Although there is no evidence on studies to examine the influence of watching cartoons on verbal self-stimulation in children with ASD, there are few studies that show the negative effects that screen media has on the development of children with ASD. In this study, the authors investigated the effect of restricting access to cartoons and an intervention based on differential reinforcement of other behaviour (DRO) on vocal self-stimulation in a 6-year-old child with autism spectrum disorders. We chose to apply a DRO-based intervention because we think that any intervention that aims to reduce behaviour must contain a component to strengthen another functional behaviour that will replace it. The treatment was implemented in an ABAB design. The findings revealed that restricting access to cartoons and an intervention based on DRO reduced the vocal stereotypies.
Keywords: Autism spectrum disordersvocal self-stimulationcartoonsdifferential reinforcement of other behaviour
Introduction
The incidence of autism spectrum disorders (ASD) is on a massive increase. According to a study by Frye (2018), in the US the incidence was of 1 in 59 children.
ASD are a life-long condition characterized by limited or atypical communication, deficits in social interactions and stereotypical behaviour.
The stereotypical behaviour of children with ASD is characterized by repetitive, non-contextual and apparently non-functional nature. It can interfere with discrimination learning, auditory processing and typical social behaviours (Ahearn, Clark, DeBar, & Florentino, 2005). Many studies analysed different types of vocal stereotypy including echolalia (Ahearn et al., 2005), phrases, words or sounds that are non-contextual (Falcomata, Roane, Hovanetz, Kettering, & Keeney, 2004), repetitive sounds which are often unintelligible (Taylor, Hoch, & Weissman, 2005), or some combination. However, the frequency of vocal stereotypy in children with ASD has been a great concern to families and teachers because the effect that these behaviours have on learning and social interaction (Athens, Vollmer, & Sloman, & St. Peter Pipkin, 2008).
There has been relatively limited research focused on the treatment of vocal self-stimulation in children with ASD. It is very difficult to treat the vocal self-stimulation due to the self-reinforcing function of these behaviours (the automatic reinforcement) (Szu-Yin & Baker, 2011). Temple Grandin (Condrey, 2015) a famous author, inventor, lecturer and adult with ASD says most children with ASD feel very good when caught in these stereotypical behaviours.
These behaviours occur in all environments, including the school environment, and have a negative effect on the interaction between the child with ASD and the teacher and between him and his colleagues, and also on the teaching-learning process itself.
Due to the fact that these stereotypical behaviours are atypical, even strange, teachers often hesitate to include children with ASD in their classes. According to the literature, the level of comfort or discomfort that teachers feel about these behaviours is one of the most important factors in measuring self-efficacy. Teachers often consider that students with ASD will have a multitude of classroom behaviours, creating constraints and challenges beyond their ability to cope (Higginson & Chatfield, 2012; Horne & Timmons, 2009; Maccini & Gagnon, 2006).
Self-stimulation has always been a challenge for all specialists working with students with ASD (teachers, psychologists, special educators, speech therapists and others). This leads to the urgent need to find effective ways of reducing these behaviours, to facilitate interaction with these children and to help them become more receptive and improve learning.
Screen Media and Autism Spectrum Disorders
Psychiatric disorders are often associated with problematic use of screen media (Slobodin, Heffler, & Davidovitch, 2019). Several studies support the view that children and adolescents with ASD are exposed to more screen time than other clinical groups and their typically developing peers (Slobodin et al., 2019). Also, these studies suggest that the exposure to screen time starts at a younger age in children with ASD (Slobodin et al., 2019).
Other studies have reported adverse effects of using media on children’s development: reduced cognitive development, hyperactivity and attention disorders (Numata-Uematsu et al., 2018). Evidence suggests that children with ASD use media differently than typically developing peers. These differences place them at greater risk for negative health outcomes that include physiologic, cognitive, social, emotional and legal problems (Gwynette, Sidhu, & Ceranoglu, 2018).
Individuals with ASD are often preoccupied with the internet, television and video games (screen-based media) (Mazurek, Shattuck, Wagner, & Cooper, 2011). They have strong preferences for cartoons, media ads, movies and video games. There are patterns of use of technologies that can be correlated to behavioural manifestations of autism (Alarcon-Licona & Loke, 2017). The correlation between problematic video game use and inattention and oppositional behaviour has been investigated and the findings suggested that problematic game use and Role-Playing game were significant predictors of oppositional behaviour in children with ASD (Mazurek & Engelhardt, 2013).
The content and context of media screen use was also investigated and the effect they have on children’s behaviours (Slobodin et al., 2019). A thematic analysis of some in-depth interviews found that children with ASD preferred media content with features aimed at younger audiences (Martins, King, & Beights, 2019). Parents also reported that children often imitate the cartoons content, occasionally with observable benefits (e.g., verbalizing words and phrases). Parents also use media as a way to calm their children (Numata-Uematsu et al., 2018).
Many parents observe only the benefits of watching cartoons, telling therapists that their child with ASD uses new words or phrases in foreign languages, they have learned from cartoons. But often these words and phrases are repeated by the child with no function, outside the context, being a common theme of their delayed echolalia. The imitation of verbal or motric behaviours seen on the screen could be useful when the purpose is learning and when a specialist has control over media content. But for a child with delayed echolalia who is allowed to watch whatever cartoons he likes, they can become harmful.
Although problematic use of media has been associated with behaviour problems among typically developing children, there has been very little research reported on this relation among children with ASD. The present paper extends this literature by focusing on the influence of cartoons on vocal self-stimulation, a relation that has not been studied so far.
Differential reinforcement of other behaviour
Any treatment that aims to reduce a target behaviour must contain a reinforcement strategy of an alternative response, to be efficient. Different techniques of applied behavioural analysis have proven to be effective in reducing problematic behaviours in children with ASD.
Differential reinforcement of other behaviour (DRO) is a widely used technique for reducing undesirable behaviour in individuals who are developmentally disabled (Lennox, Miltenberger, Spengler, & Erfanian, 1988) and, also, in typically developed individuals. DRO is a non-punitive procedure where the strengthening is contingent on the absence of problem behaviour after a fixed time or at certain moments. In general, the DRO technique is used in combination with other reductive procedures.
However, this technique is appealing because reinforcers are presented contingent on other or alternative responses (Vollmer, Iwata, Zarcone, Smith, & Mazaleski, 1993). It can be used to strengthen appropriate communication (e.g., request, commentaries) and to encourage adaptive behaviour.
We have not yet found studies to test the effectiveness of DRO in reducing vocal self-stimulation in children with ASD. Due to the fact that vocal self-stimulations are hard to reduce, there are very few studies to focus on techniques that can reduce this type of stereotypy.
Problem Statement
Vocal self-stimulation had a negative influence upon active participation in activities, communication, compliance, joint attention, interaction with adults and colleagues from the school, where the 6-year-old child, the subject of this study, is included. These behaviours are present at school, in one-to-one therapy, at home and in any environment.
To analyse the frequency of vocal self-stimulation compared to other types of self-stimulation and in different environments, three types of stereotypical behaviours were measured in school settings and in one-to-one therapy settings: the vocal stereotypy, the motor stereotypy and the combined vocal and motor stereotypy. We calculated the rate of these behaviours per hour, taking data every time the boy engaged in the target behaviours. Data taken is presented in the figures below (Figure
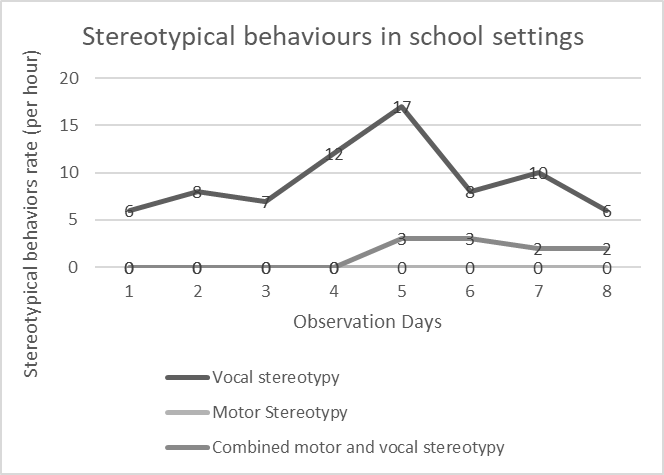
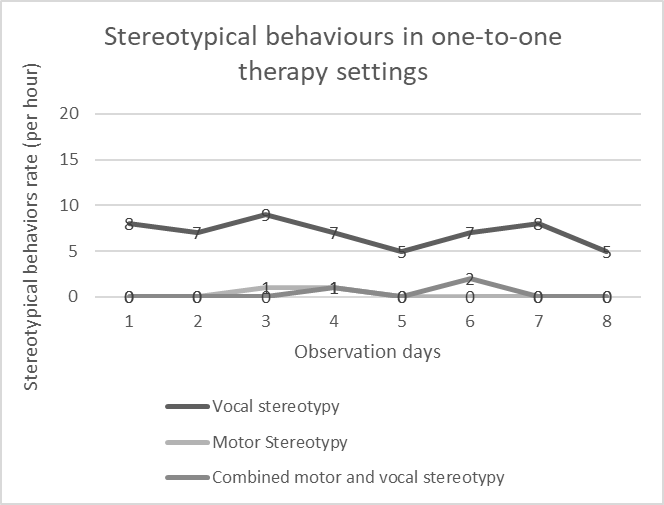
As can be seen in the figures above, vocal self-stimulation/stereotypy occurs more frequently than motor stereotypy and combined stereotypy (motor plus vocal stereotypy). It can also be observed that in the school context they are more common. Although it would have been better the data for this study to be taken in the school context, this could not be possible due to video recording policies in schools.
However, the therapists considered it is important to find out what is the source of these self-stereotypies due to the fact that they could not be reduced by ABA classical methods of self-stimulation reduction: response interruption, redirection or overcorrection.
Following the systematic observation of the child’s behaviour, the functional analysis of verbal self-stimulation, and the topographic behavioural analysis (the theme of self-stimulation), the team of specialists with training in applied behavioural analysis concluded that watching cartoons might maintain the verbal self-stimulation in this subject.
Research Questions
Regarding vocal stereotypy, most of the studies focus on behaviours which are maintained by automatic reinforcement without analysing the external factors in the antecedent which could maintain the self-stimulation (Rehfeldt & Chambers, 2003; Dixon, Benedict, & Larson, 2001). None of them evaluate the effect of cartoons on maintaining vocal-stereotypy. On the other hand, we consider that every intervention that aims to reduce problematic behaviours has to reinforce an alternative behaviour that can replace it.
Therefore, the question of this research is:
What is the impact of restricting access to cartoons and an intervention based on differential reinforcement of other behaviour upon vocal self-stimulation?
Purpose of the Study
The current study investigates the effect of restricting access to cartoons and the implementation of an intervention based on DRO on vocal self-stimulations in a 6-year-old boy diagnosed with autism spectrum disorder. Therefore, this study aims to test the hypothesis that restricting access to cartoons and an intervention based on differential reinforcement of other behaviour (DRO) can reduce vocal self-stimulation.
Research Methods
Participant, response definition and setting
The child is a six-year-old boy who had been diagnosed with autism spectrum disorder. He lives with his parents in Cluj-Napoca, Romania, and is included in a mainstream school, where he participates in two classes per school day, with a “shadow” – a therapist with training in behavioural applied analysis. He is attending behavioural therapy sessions 6 hours/day in a Behavioural Applied Analysis Centre in the same city.
He’s target behaviour was “vocal self-stimulation”, defined as repeating phrases, words and noises or singing (not appropriate in the context).
He has been referred by his parents, therapists and “shadow” as exhibiting vocal self-stimulation that occurred at unacceptable levels at home, school or therapy centre. His school teacher also reported that his vocal self-stimulation interfered with his participation in educational activities.
The “other behaviours” reinforced through DRO method were appropriate and contextual vocalizations, word or phrases including requests and commentaries, and playing quietly.
The intervention was implemented by the current study’s first author and conducted in a particular therapy room, at the therapy centre. Although the frequency of vocal stereotypy was higher in school settings, we chose the one-to-one therapy setting for implementing the intervention due to the fact that the therapy room is equipped with a camera that allowed data to be taken by two therapists.
The room furniture consisted in one table, two chairs, one mattress, and some toys.
Variables and measurement
The vocal-self stimulation was measured following an ABAB design, in two baseline and intervention phases.
The dependent variable (DV) was the percentage calculated with momentary time sampling method of 1-minute partial intervals at the end of which the boy was engaged in a vocal-self stimulation. Every experimental session lasted for 60 minutes.
A treatment based on the restricting access to cartoons and the implementation of an intervention based on DRO was the independent variable (IV) for this study.
Interobserver Agreement
35% of the sessions were filmed and scored by two therapists in order to assess inter-agreement data on the occurrence or non-occurrence of target behaviour in baseline and experimental sessions. Some sessions were not filmed due to the fact that two observers were present and able to collect data simultaneously. Two observers, the first author and another person (a therapist with training in applied behavioural analysis and over 3 years of working with children with ASD), independently collected data on the target behaviour (including both baseline and experimental phases). The first author taught the second observer the operational definition of the target behaviour and gave him examples. They compared data collected. An agreement was scored if the data taken by both the observers was identical, for each interval. Every discrepancy was counted as a disagreement. The interobserver agreement was calculated on an interval-by-interval basis by dividing the sum of agreed data with the sum of the agreed and disagreed data, all multiplied by 100. The average of agreement was 89.69 % (range from 84.90% to 95%). The interobserver agreement scores are presented in Table
Research design
The ABAB design was chosen for this single-subject study. A - phases represented baseline conditions and B - phases represented intervention conditions (restricted access to cartoons plus DRO). All sessions were conducted in the same therapy room from the therapy centre where the subject is included.
Procedures
All data were collected on vocal self-stimulation. The therapy room is equipped with a camera, so each session was recorded, and then two observers took independent data over the same therapy period. The session consisted in specific therapeutic activities (Discrete trial teaching, incidental teaching, etc.) developed by two therapists (the first author and another therapist having three years of experience in working with children with ASD), following the objectives of the intervention plan. During the intervention there were also free breaks (maximum 5 minutes), 2 or 3 times in 60 minutes, during which the subject received no instruction.
Baseline (phase A). During the baseline, the subject's parents gave him access to cartoons as a reward for desirable behaviours (accepting routine changes or unpleasant stimuli), or to prevent behavioural problems in public contexts (for example, at the barber or at the restaurant). The subject had access to cartoons about 30 minutes a day, but not every day. There were no consequences for engaging in vocal self-stimulation during baseline. In the therapy session, the therapists delivered reinforcement for instruction, answering questions, spontaneous comments or completing the activity. A token system was used as reinforcing method, consisting in receiving a token after every completed task and choosing a reward, after having 10 tokens, from several rewards chosen in preference assessment. Baseline sessions lasted 60 minutes each and were repeated for 5 or 6 sessions.
Intervention condition (phase B). In the intervention phase data was taken after two weeks from restricting access to cartoons due to the delayed echolalia of the subject, who was repeating phrases or words from cartoons several days after watching them. In this phase, the DRO-based intervention was introduced during the therapy sessions. This consisted in positive reinforcement (through token system and social reinforcement) of verbal requests, contextual comments and moments in which he was playing quietly without verbal self-stimulation. For example, if the subject independently vocalized something related to the context or if he had been playing for approximately one minute quietly, the therapist delivered one token and praise.
Findings
Figure
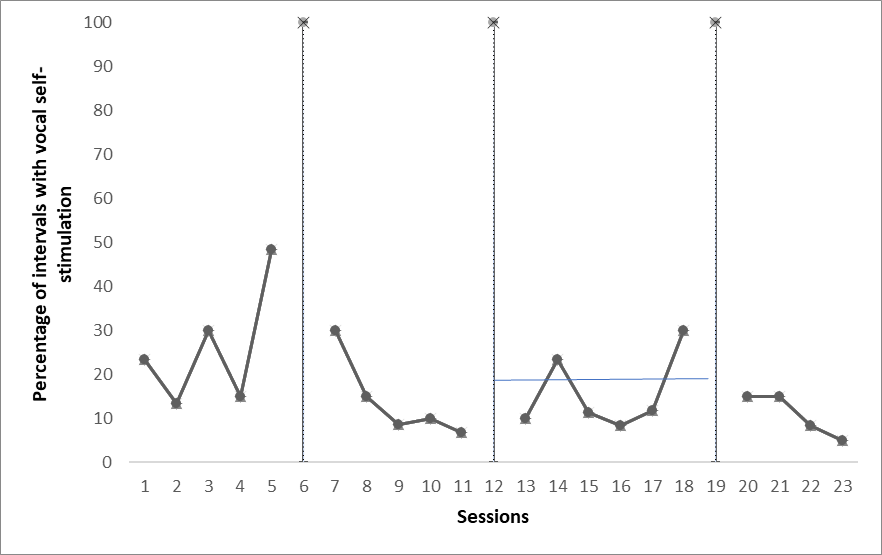
The ABAB reversal design was used to confirm that the intervention resulted in a change in behaviour. In our study, the percentage of intervals the subject was engaged in vocal self-stimulation was high during the first baseline phase, decreased during the first intervention phase, increased again during the second baseline phase and again decreased during second intervention phase. Due to the fact that the dependent variable (the frequency of vocal self-stimulation) changes with the introduction of the intervention (restricted access to cartoons plus DRO) and then changes back with the removal of the treatment, it is much clearer that the intervention (and removal of the intervention) is the cause of decreasing the frequency of vocal self-stimulation. In other words, the reversal greatly increases the internal validity of this study.
Conclusion
Limitations of the study
Several limitation are important to be presented. First, as in every single subject designs, findings cannot be generalized to all children with ASD who have delayed echolalia or vocal stereotypy. Therefore, this study’s external validity is limited because of including only one child and one setting. The findings are based on the subject’s characteristics. Although this limitation in the generalizability of the findings, the rigor of a single-subject design, including the reversal design, establishes a functional relation between the two variables (the intervention and vocal self-stimulation) (Cooper, Heron, & Heward, 2016). Moreover, the quality indicators (the detailed description of the subject and setting, the precise definition of the variables, the justification of the intervention chosen, based on the systematic observation of the behaviour in multiple settings and the functional analysis of the behaviour) established the consideration of the importance of social validity, proposed by Horner et al. (2005). Due to the fact that this study met the quality indicators, future research replicates are made possible to determine the generalization on different subjects. The replication of the experimental effects across participants, settings or materials could establish external validity (Horner et al., 2005).
A second limitation of the study was the limited number of data points within each phase. The time allocated for this study was limited and it is possible that the intervention effects would have been more visible with a greater number of sessions. Thirdly, the numbers of sessions for which we had the interobserver agreement was limited, due to the fact that the second observer was a volunteer, who also had a schedule of therapy sessions with other children with ASD, included in the therapy centre.
Fourthly, to ensure that the effects of the delayed echolalia after watching cartoons has diminished, we began to take data for the intervention phase two weeks after restricting access to cartoons, which means that the sessions in which data were taken in the intervention phase are not consecutive to the data taken in the baseline. This may raise questions about the direct effect of restricting access to cartoons to reducing behaviour. Also, during the second baseline phase, the subject had significantly less time access to cartoons than in the first baseline phase. For ethical reasons, we did not want to extend the period of access to cartoons, knowing that fact that they have a negative effect on the behaviour of the subject.
Another important limit is that data may underestimate the frequency of occurrence of the behaviour. Because most of the data was taken from the video recording of therapy sessions, the observers may not have heard all of the vocal self-stimulations, especially as the subject often whispers. Also, the momentary time sampling method is known to underestimate the frequency of occurrence of the behaviour because data is taken only at specific time points (1:00 minute).
In conclusion, interpretations of this study’s results should be cautious.
Conclusion and implications
The findings showed that restricting access to cartoons and introducing an intervention based on differential reinforcement of other behaviour reduces vocal self-stimulation in a subject with autism spectrum disorders.
These results of the study highlight the importance of examining the influence of watching cartoons among children with ASD, the effect of restricted access to cartoons and the importance of replacing the verbal self-stimulation with another behaviour which is functional and suitable in the context. They also indicate a need for future experimental and longitudinal research in this area. Future research should strengthen the internal and external validity of this study by replicating the procedures.
In addition, to promote long-term meaningful change and reduce limitation of external validity, the intervention should be implemented across different settings (e.g. in the classroom, at home, in free play time) and people (e.g. school teacher, parents). Another investigation would be to implement the DRO intervention on a full-day basis within a natural setting. Because this study was only implemented at a certain time per day, in the same controlled setting, the results were unable to reveal whether the parents or the school teacher would continue the reinforcing of other behaviours or whether they would encounter any difficulties.
One other implication would be to see the effectiveness of each of the independent variables, separately, in an alternating treatments design. It would also be interesting to see if the proposed intervention increases the number of desirable behaviours (e.g. requests, comments, functional play).
Children with ASD are unique, each having different characteristics and different history of each learned behaviour. These differences represent the biggest challenges for specialists and, in most of the cases, require an individual approach.
The vocal self-stimulations represent one of the most difficult to treat behaviours in children with ASD, which affect the quality of their life and deprive them of important environmental stimulation. Therefore, the reduction of these behaviours is very important and necessary in order to facilitate and optimize the learning and the social interaction. In order to find and implement an effective intervention, the external factors from the antecedent that could maintain the behaviour should be taken into consideration, as well as, the reinforcing of other alternative behaviours that can replace the problematic behaviour.
Our study could be an example for the implementation of an intervention that can reduce vocal self-stimulation in children with ASD.
References
- Ahearn, W., Clark, K., DeBar, R., & Florentino, C. (2005). On the Role of Preference in Response Competition. Journal Of Applied Behavior Analysis, 38(2), 247-250. https://doi.org/10.1901/jaba.2005.36-04
- Alarcon-Licona, S., & Loke, L. (2017). Autistic Children's Use of Technology and Media. In Proceedings Of The 2017 Conference On Interaction Design And Children - IDC '17. https://doi.org/10.1145/3078072.3084338
- Athens, E., Vollmer, T., Sloman, K., & St. Peter Pipkin, C. (2008). An Analysis of Vocal Stereotypy and Therapist Fading. Journal Of Applied Behavior Analysis, 41(2), 291-297. https://doi.org/10.1901/jaba.2008.41-291
- Condrey, J. H. (2015). General Education Teacher Perceptions of Self-Efficacy Regarding Teaching Students with Autism in Inclusion Settings. Education Dissertations and Projects, 148. https://digitalcommons.gardner-webb.edu/education_etd/148
- Cooper, J. O., Heron, T. E., & Heward, W. L. (2016). Analiza aplicată a comportamentului. Cartea Albă, ATCA. București: Alpha MDN
- Dixon, M. R., Benedict, H., & Larson, T. (2001). Functional analysis and treatment of inappropriate verbal behavior. Journal of applied behavior analysis, 34(3), 361–363. https://doi.org/10.1901/jaba.2001.34-361
- Falcomata, T., Roane, H., Hovanetz, A., Kettering, T., & Keeney, K. (2004). An evaluation of response cost in the treatment of inappropriate vocalizations maintained by automatic reinforcement. Journal Of Applied Behavior Analysis, 37(1), 83-87. https://doi.org/10.1901/jaba.2004.37-83
- Frye, R. (2018). Social Skills Deficits in Autism Spectrum Disorder: Potential Biological Origins and Progress in Developing Therapeutic Agents. CNS Drugs, 32(8), 713-734. https://doi.org/10.1007/s40263-018-0556-y
- Gwynette, M., Sidhu, S., & Ceranoglu, T. (2018). Electronic Screen Media Use in Youth With Autism Spectrum Disorder. Child And Adolescent Psychiatric Clinics Of North America, 27(2), 203-219. https://doi.org/10.1016/j.chc.2017.11.013
- Higginson, R., & Chatfield, M. (2012). Together we can do it: A professional development project for regular teachers’ of children with autism spectrul disorder. Kairaranga, 13(2), 29-40. Retrieved from https://eric.ed.gov/?id=EJ994983
- Horne, P., & Timmons, V. (2009). Making it work: teachers’ perspectives on inclusion. International Journal Of Inclusive Education, 13(3), 273-286. https://doi.org/10.1080/13603110701433964
- Horner, R. H., Carr, E. G., Halle, J., McGee, G., Odom, S., & Wolery, M. (2005). The Use of Single-Subject Research to Identify Evidence-Based Practice in Special Education. Exceptional Children, 71(2), 165–179. https://doi.org/10.1177/001440290507100203
- Lennox, D. B., Miltenberger, R. D., Spengler, P., & Erfanian, N. (1988). Decelerative Treatment Practices With Persons Who Have Mental Retardation: A Review of Five Years of Literature. American Journal on Mental Retardation, 92(6), 492-501. Retrieved from https://www.researchgate.net/publication/322896323_Revision_de_las_conductas_problematicas_Enginy
- Maccini, P., & Gagnon, J. (2006). Mathematics Instructional Practices and Assessment Accommodations by Secondary Special and General Educators. Exceptional Children, 72(2), 217-234. https://doi.org/10.1177/001440290607200206
- Martins, N., King, A., & Beights, R. (2019). Audiovisual Media Content Preferences of Children with Autism Spectrum Disorders: Insights from Parental Interviews. Journal Of Autism And Developmental Disorders. https://doi.org/10.1007/s10803-019-03987-1
- Mazurek, M., & Engelhardt, C. (2013). Video Game Use in Boys With Autism Spectrum Disorder, ADHD, or Typical Development. PEDIATRICS, 132(2), 260-266. https://doi.org/10.1542/peds.2012-3956
- Mazurek, M., Shattuck, P., Wagner, M., & Cooper, B. (2011). Prevalence and Correlates of Screen-Based Media Use Among Youths with Autism Spectrum Disorders. Journal Of Autism And Developmental Disorders, 42(8), 1757-1767. https://doi.org/10.1007/s10803-011-1413-8
- Numata‐Uematsu, Y., Yokoyama, H., Sato, H., Endo, W., Uematsu, M., Nara, C., & Kure, S. (2018). Attachment Disorder and Early Media Exposure: Neurobehavioral symptoms mimicking autism spectrum disorder. The Journal Of Medical Investigation, 65(3.4), 280-282. https://doi.org/10.2152/jmi.65.280
- Rehfeldt, R. A., & Chambers, M. R. (2003). Functional analysis and treatment of verbal perseverations displayed by an adult with autism. Journal of Applied Behavior Analysis, 36(2), 259-261. https://doi.org/10.1901/jaba.2003.36-259
- Slobodin, O., Heffler, K. F., & Davidovitch, M. (2019). Screen Media and Autism Spectrum Disorder: A Systematic Literature Review. Journal of developmental and behavioral pediatrics: JDBP, 40(4,1), 303-311. https://doi.org/10.1097/DBP.0000000000000654
- Szu-Yin, C., & Baker, S. (2011). Effects of noncontingent reinforcement and response interruption and redirection on a child’s vocal stereotype maintained by automatic reinforcement. Bulletin of Special Education, 36(1), 109-127.
- Taylor, B., Hoch, H., & Weissman, M. (2005). The analysis and treatment of vocal stereotypy in a child with autism. Behavioral Interventions, 20(4), 239-253. https://doi.org/10.1002/bin.200
- Vollmer, T., Iwata, B., Zarcone, J., Smith, R., & Mazaleski, J. (1993). The role of attention in the treatment of attention-maintained self-injurious behavior: noncontingent reinforcement and differential reinforcement of other behavior. Journal Of Applied Behavior Analysis, 26(1), 9-21. https://doi.org/10.1901/jaba.1993.26-9
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
17 June 2020
Article Doi
eBook ISBN
978-1-80296-084-6
Publisher
European Publisher
Volume
85
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-814
Subjects
Teacher, teacher training, teaching skills, teaching techniques, special education, children with special needs
Cite this article as:
Sălăgean, C. S., & Stan, C. N. (2020). Reducing Vocal Self-Stimulation In Children With Autism Spectrum Disorders. In V. Chis (Ed.), Education, Reflection, Development – ERD 2019, vol 85. European Proceedings of Social and Behavioural Sciences (pp. 19-30). European Publisher. https://doi.org/10.15405/epsbs.2020.06.3