
Programs Of Adventure Therapy And Drug Addiction Treatment In The Czech Republic


Abstract
Adventure therapy programmes are the activities which are included in the therapy programmes for the drug addicts in therapeutic communities in the Czech Republic. The paper presents the results of the specific university research focused on the self- efficacy rate, self-evaluation and perceived stress rate of the clients of six therapeutic communities before going through the adventure therapeutic programmes, after finishing it and 14 days after its ending. Both the experimental and control group were part of the research, the control group was made of the clients of the therapeutic communities which do not do the adventure therapy. Three psychological tests were used after gathering the data: General Self-Efficacy Scale, Rosenberg Self-Esteem Scale, Stress Test. The statistical significance was found in the areas of self-efficacy and self-evaluation of the clients before and after the programme. Statistical significance for the perceived stress rate was not proved. The control group unlike the experimental group did not show any statistically significant changes during the observation period.
Keywords: Adventure therapyclient of therapeutic communitydrug addictself-efficacyself esteemstress
Introduction
The situation in substance abuse in the Czech Republic has been in the long term stable (Mravčík, 2018). The system of services helping people with drug addiction is among well developed and covers field work, outpatients and inpatients services.
High rate of alcohol and tobacco use has been typical for the inhabitants of the Czech Republic. This trend has to do with the traditional production and consumption of beer, wine and spirits. The habit of overdue consumption of alcohol on social occasions has not changed even despite the society-wide edification. Almost 1.6 milion people in the Czech Republic are in a risk of problems arising from alcohol use, 900,000 of them are in a high risk of everyday use of alcohol (Mravčík, 2018). The most common illegal drug in the Czech Republic is marijuana. The number of problem users of meth and opiate reaches up to 48,000. Approximately one third of the population in the age 15-64 states they have had an experience with using an illegal drug in the past 10 years or so. It is mostly men in the age group 15-34 who state they have had an experience with using illegal drugs (Mravčík, 2018).
Stay in a therapeutic community is one of the possibilities of treatment one can chose when addicted to drugs. The first community was established at the beginning of the 90s (Radimecký, 2006; Kalina, 2008) and since then their number has risen to tens others run either by mental hospitals in health care or as social services. Therapeutic communities have gradually become an important part of the system of care of the drug addicts. (Doležalová, 2006). It offers a structured treatment programme in small groups. The final goal is a gradual re-socialization of the client and their re-integration into the major society. The client in therapeutic community goes through several follow up stages. Some treatments are used by all therapeutic groups such as: community meeting, work therapy, practical roles in community, work with rituals (Kalina, 2008), others use only some of them. One of them is adventure therapy which our research focuses on.
This paper describes the quantitative part of the specific university research of the Faculty of Education, University of Ostrava, Social Education Department. Both the students and academic workers took part in the research in the years 2017-2018. They were finding out a short-term impact of the adventure therapy in chosen areas on clients of six therapeutic communities for drug addicts in the Czech Republic. The research problem, research questions and hypotheses are defined in the paper. The psychological tests, which were used, are presented below. The results are interpreted and the discussion about the findings is in the conclusion.
Problem Statement
The adventure therapy programmes are part of the activities of some therapeutic communities for the drug addicts in the Czech Republic. We have noticed different views of the therapeutic communities´ workers on whether it is suitable or not to include this method. The strongest anti arguments were: time consumption of preparing and realizing the activities, high risk of an injury, negative attitude of some clients to this kind of activities, big demands as for the physical condition and mental resilience of the therapeutic communities´ workers, artificially induced stress and touch and go effect of the activities. The workers who supported this activity mentioned: bigger togetherness of the group, strengthening the relationship of the worker – client positive impact on overcoming one´s physical limits, new topics coming up for follow up therapeutic work and joy and satisfaction with coping not only by clients but also workers. We have found only two researches in the Czech environment which were carried out on this topic and that is the research of Romaněnková (2012) who analyses the opinions of the workers of these activities and Richterová, Štenclová and Červenková (2017) carried out a specific university research – project of the students grant competition of the University of Ostrava which focused on analysing the clients´ opinions of these programmes in one community in the years 2015–2016. Neither of these researches used standardized methods and the limited number of respondents made it impossible to generalize the findings (Šlachtová, Richterová, & Müller, 2019). On the other hand a number of researches focusing on the efficiency of the method have been found abroad. The adventure therapy programmes were carried out in groups of people with addictions and delinquent behaviour (Larson, 2007; Harper, Russell, Cooley, & Cupples, 2007; Lewis, 2013; Magle-Haberek, Tucker, & Gass, 2012; Paquette & Vitaro, 2014), unfortunately none of the published researches focused on the use of the programme in therapeutic community.
Based on the literature and the analysis of the community workers´ expectations from these programmes three areas of efficiency were chosen: self-efficacy, self-evaluation and perceived stress rate of clients, they were tested with psychological tests before the programme, straight after the programme and to find out the longstanding effect also 14 days after the ending.
Research Questions
With regard to the above specified research goal the main research question is as follows: What are the statistically significant changes in chosen areas of self-concept of the clients of the therapeutic communities for the drug addicts who participated in the adventure therapy? Partial research questions find out what statistically significant changes occur in the area of self-efficacy, self-evaluation and perception of the stress rate of the clients of the therapeutic communities before the adventure therapy, after and 14 days after the programme.
Purpose of the Study
The therapeutic communities which include adventure therapy programmes in their activities expect a positive impact in several areas. First of them is expected change of clients´ self-efficacy. Bandura (1994) defines the self-efficacy concept in social learning theory (p. 71-78) as judging one´s own possibilities to organize and realize an activity required to deliver the given performance. He states there is a direct proportion between the expected efficiency and the changes in one´s behaviour. The synonym for self-efficacy may be e.g. perceived personal competence, perceived efficiency, belief about one´s potential or judgment about one´s abilities to initiate activities and reach the set goal. The values of self-efficacy scores apply to one´s belief to reach something regardless of their real competence. The judgment about one´s self-efficacy in a particular situation is a good performance predictor in a particular situation (Wiegerová et al., 2012). Self-efficacy influences person´s decision what they will do and how they will do it. If the individual has a good self-efficacy rate they will go for more demanding procedures, they will be more persistent and resistant when overcoming obstacles and will have a strenuous effort. People with high self-efficacy believe in themselves more, set more demanding goals and are successful in meeting them. Their high self-efficacy enables them to maximize their own abilities, knowledge and craftmanship (Pajares, 2007). High self-efficacy creates optimistic attitudes, demanding tasks sound as a challenge; the individuals are in good mood even in unfavourable situations. On the other hand, people with low self-efficacy doubt about themselves, feel hopeless and are more vulnerable which may lead to depression and stress. The individuals stops believing in themselves, blames themselves and gives in too soon (Hoskovcová & Ryntová, 2011). Hamanová (2015) describes the unmet needs from the childhood with the addicts. It is one of the factors, which increase the risk of addiction. She ranks there the need of positive relationships in family, unnatural development, pathological or devaluating communication in family, missing emphatic support of a close adult and absence of future perspectives (work, relationships).
According to Rataj (2007) the adventure therapy programmes participate in the individual´s integration into the society as they develop the social aspect of the individual. On one side the programmes stress independence and responsibility of individuals, on the other hand they stress relying on oneself. At the same time, it is important to be able to help the weaker in a crisis, tolerate other people and not to think only about myself. It is supposed that the programmes can have impact on self-efficacy increase. The clients can achieve their successes during and after the programmes.
Another area in which we can expect changes after the adventure therapy programmes is self-evaluation. Kalina (2007) regards: immaturity, low self-esteem, problems with the character, changed value system and life scenario to be the typical psychological features of the drug addicts. High self-esteem is not always the ideal state but self esteem should be balanced and stable which can be found with the individuals who are according to Blatný more mentally resistant and cope better with disturbing influence of the environment (as cited in Maierová, 2010). Self-evaluation influences building and maintaining relationships (Maierová, 2010). The level of self-evaluation depends on several factors such as life satisfaction, dominance, extraversion or hostility. Experiencing positive emotions towards oneself causes more active approach to reaching the set goals and it is then easier to cope with severe life situation (Paulík, 2012).
If a client participates in the adventure therapy programme we expect the increase in their self-evaluation. If the client has the space to make decisions and act which is one of the important aspects of the adventure therapy programme, then they feel more satisfied when assessing their performance and take pride in their personalities. Clients are awarded by a group and achieve success before themselves and before others, their self-confidence rises and so does their self-evaluation (Kraska-Lüdekce, 2007).
The last of the areas we chose where we can expect changes in connection with the clients´ participation in adventure therapy programmes is stress perception. Stress can be defined as tension. According to Schreiber (2000, as cited in Kirchner, 2009) it is “a demand on an individual which exceeds their abilities to cope and face the demand without problems. It is any kind of an environment impact (physical, chemical, social, psychological, political), which endangers the health of some sensitive individuals” (p. 36). A stressor is a subject which recalls this state of tension. If the client is exposed to stress factors repeatedly they cannot achieve optimal performance. People choose the most secure solution in a stress situation, one that they have already had some experience with. With repeated stress situations people make mistakes and their quality of work, concentration and motivation decline (Kraska-Lüdekce, 2007). Resilience is important for successful progress of the adaptation process. Resilience can be defined as a range of subjects that a person is able to cope with without suffering severe mental damage. Thanks to the resilience we can better cope with the strain. One of other research suppositions is the verification whether bigger strain increases the individual´s resilience and therefore decreases the stress level.
Research Methods
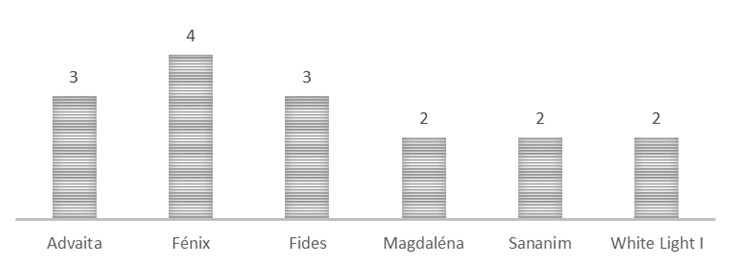
The experimental group was made of clients older than 15 years from six therapeutic communities for the drug addicts in the Czech Republic in which there are the adventure therapy programmes. The following therapeutic communities were involved - TC: TC Fides in Bílá Voda, TC Fénix in Bílá Voda, TC Němčice in Heřman, TC White Light I. in Mukařov, TC Advaita in Nová Ves u Liberce and TC Magdaléna in Mníšek pod Brdy. 277 clients, 164 men (72%) and 63 women (28%) took part in the research (see Table
According to the Table
In each of the above mentioned communities of the experimental groups there are adventure therapy programmes on programme. The programmes are based on the relationship of a person to the nature and civilization. They contain activities in nature, teach clients to save resources. The adventure therapy programmes are usually connected with sport activities which improves clients´ condition and performance. Clients overcome their limits – tiredness, insecurity, exhaustion, climactic discomfort etc. Coping with burden inspires clients to do sports in free time. Thanks to unexpected situations, the need to improvise during the programme and to adapt to unplanned situations there occur stresses and conflicts which the clients must solve. Some situations must be solved in cooperation, in mutual support, tolerance and taking over the responsibility. The age differences are not important any more. New members of the community adopt quicker in small social groups and informal relationships deepen.
The activities which correspond with basic definition of the adventure therapy programmes were put on the research: “The adventure therapy programmes as a part of the treatment process are mentally and physically demanding activities which are realized as several-day long excursions of sport touristic character“ (Richterová et al., 2015, p. 92). The length of the programme was also one condition for putting it on the programme. The clients had to spend two and more nights away from the community. 16 programmes were put on the research. The activities which did not compel with the above mentioned definition had to be discarded (e.g. one day activities and cultural activities). One activity had to be discarded because a community did not test the clients before the activity but only after it ended. The number of realized programmes in the research is shown in Figure
Table
Testing in the control group went according to the schedule of the adventure therapy programmes in randomly chosen TC Fides. At this time there was a normal community schedule on, which included group therapy, relaxation, arte therapy and work therapy in workshops.
Quantitative design of work was chosen with the main method of data collection – questionnaires. The questionnaires were carried out in three time periods: right before the programme, right after the programme and 14 days after the programme.
The following psychological tests were chosen: “General Self-Efficacy Scale" (GSES), Rosenberg Self-Esteem Scale, Stress Test. “General Self-Efficacy Scale“ was made in Germany in 1979. Its authors are Ralf Schwarzer and Matthias Jerusalem. It originally contained 20 items. They were reduced to half two years later (1981). Ten- statement questionnaire was translated into 28 languages (Scholz, Gutiérrez-Doña, Sud, & Schwarzer, 2002). The Czech version was translated by Jaro Křivohlavý in 1993 (Křivohlavý, Schwarzer, & Jerusalem, 1993). The clients respond to 10 statements on a four scale of Likkert type (strongly disagree (1), disagree (2), agree (3) strongly agree (4)). The average score usually has the value 2.9. GSES finds real rate of optimistic self-concept, self-efficacy and perceived ability to cope with problems.
Rosenberg Self-Esteem Scale was created in 1965 by Morris Rosenberg. The clients respond to 10 statements on a four-rating scale of Likert type, positively formed questions (n. 1, 2, 4, 6, 7) are scored as follows: strongly disagree (0), partially disagree (1), partially agree (2) and strongly disagree (3). The questions formed negatively (n. 3, 5, 8, 9, 10) score vice versa. Rosenberg Self-Esteem Scale is a widely used method for its good reliability although there is not a Czech standardization. It was not critical for use in different testing in different periods. The test examines the level of global self-evaluation, the value of “self” with focus on self-esteem (positive questions) and auto depreciation (negative questions).
The stress test is adjusted Arnd Stein questionnaire which assesses the rate of strain. It consists of 20 YES/NO items whether the burden with each client did not exceed the bearable limit behind which there is the potential mental or physical disease risk.
The responsible therapeutic community workers were trained before the data collection. Clients were informed about the research goals and research methods. The community clients signed the informed consent and confirmed their participation in the research. The questionnaires were marked with a code for statistical purposes, the code was the abbreviation of the therapeutic community name and client´s serial number.
The data were collected from January 2018 to September 2018. Moreover, two testing from 2017 were added to the research. 681 GSES questionnaires were gained, 543 RSES questionnaires and 543 Stress Tests questionnaires were administered. 132 GSES questionnaires, 129 RSES questionnaires and 156 Stress Test questionnaires were discarded from further processing. The most common reason was incorrect completing (marking responses only on one side of the scale, marking more than one response, incomplete filling in and other). There were several reasons for gaining lower number of questionnaires after 14 days: the client finished their treatment (properly, upon request, for breaking the rules etc.), the client was not present at the time of testing (release, illness etc.). The questionnaires which were not responded in all the tree testing stages could not be included in the testing (before, after and 14 days after the adventure therapy programme). The research data were processed from 549 GSES questionnaires, 414 RSES questionnaires and 387 Stress Test questionnaires.
First the questionnaires collection was made after that the responses were transformed into numbers in Microsoft Excel. The data were statistically tested by Friedman non-parametric test and at the same time by parametric test ANOVA – 2. Friedman test enables to analyze the data gained by repeated measurement of a group of individuals. The advantage of the chosen statistical test is the speed and non-parametric character and resistant result (Hendl, 2015). Both used tests are suitable for the situation of more dependent selections. “Dependent selection” means that from each subject more measurements are gradually gained, in our case three measurements in times 1,2,3 (before, after and 14 days after the programme). All the measurements come from the same subject. In case of Analysis of variance ANOVA sometimes called two factor ANOVA when one factor are subjects and the second factor is the administration time.
Null hypotheses H0 was tested by Friedman test on the significance level α = 0.05 (5 %). When it was rejected the differences between pairs of all the time measurements were tested using the so-called simultaneous tests which were carried out on a common level of significance α = 0.05 (5 %).
Findings
The Tables
GSES test provides the most stable image. It proves significant difference in scores both for all the data in total and for men and women separately, both for the first stay in a therapeutic community and for repeated stays.
It is interesting that Rosenberg´s scale (RSES) shows progress in a similar way as GSES but only in all the data and in women but not in men. The progress is rather convincing in women (p=0.0008), but only after 14 days (contrast 1-3 is significant, while contrast 1-2 is only significant with the Analysis of Variance not with Friedman). Something else could have been at stake which subsequently increased the women´s self-confidence. On the other hand the insignificance of the contrast 1-2 in women could be caused by a low number (n=40).
We did not notice any progress in the control group as we expected in the score level (see Table
Self-efficacy
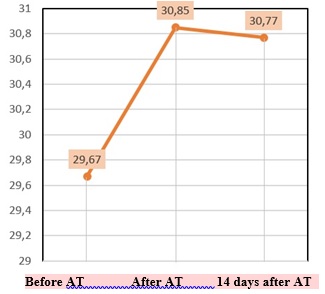
The minimal GSES points scored is 10 and maximal 40. Is it obvious from Fig.
H10 – The value of the self-efficacy score with therapeutic community clients before, after and
14 days after the adventure therapy does not differ.
H1A – The value of the self-efficacy score with therapeutic community clients before, after and
14 days after the adventure therapy differs.
Based on the results of the Freidman non-parametric test (p = 0.0000) the null hypotheses is rejected in favour of the alternative hypotheses H1A. Statistically significant difference was between time 1 (just before the programme) vs. 2 (right after the programme) and between times 1 (just before the programme) vs. 3 (14 days after the programme). The null hypotheses H10 is not rejected for the time measurement 2 vs. 3, where a statistically significant change was not proved.
Self-efficacy that is perceived personal efficacy and persuasion of one´s potentials proved to be statistically insignificant after the research. The clients of the therapeutic community for drug addicts are convinced about their own efficacy after going through the programme and they show trust in their abilities. The clients have these feeling right after the programme and they last even after 14 days.
Self-evaluation
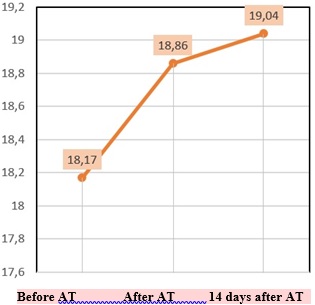
Each of the RS questionnaires´ scales enables gaining the points scored from 0 to 30. The minimal score spanned from 2 to 5 before, right after and 14 days after the adventure therapy programme.
There were no changes in the individual measurement stages in maximal point scored. The average measured point score spanned from 18.17 to 19.04.
Figure
H20 – Self-evaluation point score does not differ before, after and 14 days after the adventure therapy.
H2A - Self-evaluation point score differs before, after and 14 days after the adventure therapy.
Based on the results of the Friedman non-parametric test (p = 0.0005) the null hypotheses is rejected in favour of the alternative hypotheses H2A. Statistically significant difference is between times 1 (just before the programme) vs. 2 (right after the programme) and between times 1 (right before the programme) vs. 3 (14 days after the programme). The null hypotheses H20 is not rejected for the time measurement 2 vs. 3, where statistically significant change was not proved.
Self-evaluation or emotional relationship to one´s self proved to be statistically significant after the research. The clients of the therapeutic community for the drug addicts are mentally balanced after the load activity. Clients have these feelings right after the programme and they last even after 14 days.
The perceived stress rate
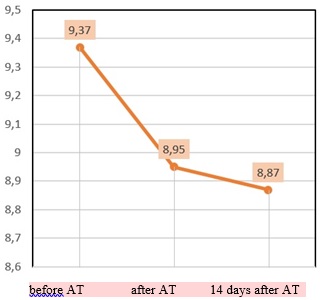
Each TPS questionnaire´s scale enables to gain point score between 0 to 20. Fig. 04 shows that there were no changes in the minimal and maximal scores in the individual measurement stages. The lowest score was 0 and the maximal score was 19. The average measured value spanned from 8.87 to 9.37. The diagram 4 shows that the progress happens in an unwanted direction (score decrease) in all the measurement times (between times 1 and 2, 1 and 3, 2 and 3).
H30 – The values of the stress score of the clients of a therapeutic community before, after and 14 days after does not change.
H3A – The values of the stress score of the clients of a therapeutic community before, after and 14 days after changes.
TPS does not show any significant changes when using the Friedman test (p = 0.13) see Tab. 10. On the other hand the parametric ANOVA-2 shows significant difference even though only in men. But even this difference vanishes with the stricter level 1 %. We can see the results of the ANOVA test in Table
The stress rate or negative emotional tension proved to be statistically insignificant after the research. As for the perception of one ´s own abilities such as coping with the strain, adapting or being resistant to outer influences there was no statistical significance found with clients right after the programme and not even 14 days after.
Conclusion
The research carried out shows several limitations. The first is the choice of the tests which focus on clients´ own evaluations or opinions. With regards to the characteristics of the drug addicts we can assume certain level of instability and moods which could distort the results into some extent. To include a client into testing they had to complete three series of questionnaires. Some clients´ motivation to enter the research was to learn about their results. In our case of three testing the clients could see the results only after a year. This decreased the motivation to complete the tests carefully.
Another limiting factor was different approach of therapeutic communities to testing. Although the selected community workers were trained it was not always them who did the testing but sometimes a worker on shift. The data reading was made with slight deviations, in the second testing there was sometimes am interval of a day or more.
The limit of the control group was the clientele with a different addiction than the experimental group. Another limitation was average higher age. The therapeutic community Harmony had clients mainly with alcohol or mixed addiction. The therapeutic community Tao had clients with dual diagnosis and psychiatric diagnosis. Despite the mentioned research limitations the results show the meaningfulness of including the adventure therapy to treatment programmes of the therapeutic communities for the drug addicts.
Based on the Friedman test it was possible to reject the null hypotheses H10 a H20 in favour of the alternative hypotheses H1A a H2A. This confirmed our assumption that the values of the self-efficacy scores and self-evaluation of the clients of therapeutic communities will differ before, after and 14 days after the programme. The GSES test shows significant difference in scores both for all the data in total and for men and women separately for the first as well as repeated stay. The progress is in a wanted direction (score increase), both in time of the programme impact (between times 1 and 2), as well as with ongoing effect 14 days after the programme (significant difference between times 1 and 3, insignificant between times 2 and 3). We can say that the adventure therapy programmes have positive impact on the clients´ belief in their own success and on trust in their own abilities. The Rosenberg´s self-evaluation scale (RSES) showed the progress in a similar way as GSES but only in all the data and in women, not in men. This progress is rather convincing with women (p=0.0008) but only 14 days after the programme (contrast 1-3 is significant while the contrast 1-2 is significant only with the Analysis of Variance not with Freidman test). Simultaneous tests showed that the programmes have positive impact on clients´ mental balance and emotional relationship to one´s self. On the other hand our assumption that the stress rate score values will change before, after and 14 days after did not prove. It was not possible to reject the tested null hypotheses H30. No statistically significant change was proved between times 1 (just before the programme) vs. 2 (right after the programme) and times 2 (right after the programme) vs. 3 (14 days after the programme). There was statistically significant difference only between times 1 (just before the programme) vs. 3 (14 days after the programme). TPS does not show any significant differences when using the Friedman test. On the contrary the parametric ANOVA shows a significant difference but only in men. Even this difference vanished with a stricter level 1 %. We can say that the adventure therapy does not have any impact on the therapeutic community clients as for their emotional tension, coping with strain, ability to adapt and be resistant to outer influences.
Control group testing was a part of the research too. The measurement was made in two therapeutic communities, TC Tao and TC Harmonie it was done according to the adventure therapy programme schedules in TC Fides. The data collection was done from January to September 2018 and it was done just before and right after the programme But there were no statistically significant personal changes found (that is not in self-efficacy, self-evaluation and not even in the stress rate). It follows from this that personal progress in groups doing the adventure therapy can really be credited to the adventure therapy programmes influence.
The results of our research confirmed the therapists´ opinions that Romaněnková (2012) wrote about. Based on the qualitative analyses of the therapists´ experience she found that after the adventure therapy programme positive evaluation of the activity as well as positive self-evaluation prevail. According to Gass, Gillis and Russell (2012) the adventure therapy has significant benefits in gaining experience which help clients to form new views of the world and values. Clients get the opportunity for their own decision making and take over responsibility for their decisions. Coping with these activities raises clients´ self-confidence. Chytilová (2005) regards the risk which is an inherent part of the adventure therapy to be very important for these days when many people crave for adrenaline. Clients who are not sensitive to dopamine response require adrenaline activities regardless of possible risk and hazard. And just the adventure therapy programmes can replace their craving for drug and the following experience by an adrenaline activity which increases their self-efficacy. After coping with the crises situations which are an inherent part of the adventure therapy programme relationships quality improvement and better mutual communication follow (Gass, Gillis, & Russell, 2012). The mentioned social skills are closely connected to the studied personal characteristics.
Acknowledgments
This research was conducted within a specific university research SGS. Aneta Žilinská and Julia Sladkowská, the students of the University of Ostrava participated in the published part of the research, Ivo Muller compiled the statistics, Silvie Quisová is the psychological testing guarantee. The author of this paper is Bohdana Richterová, the main researcher of this project.
References
- Bandura, A. (1994). Self-efficacy. In V. S. Ramachandran (Ed.), Encyclopedia of human behaviour (pp. 71-81). New York, NY: Academic Press.
- Chytilová, L. (2005). Dobrodružné aktivity ve výchově a vzdělávání [Adventure activities in education]. Gymnasion: časopis pro zážitkovou pedagogiku, 2(3), 9-18.
- Doležalová, P. (2006). Kvalita života drogově závislých v terapeutických komunitách [Quality of life of drug addicts in therapeutic communities]. Adiktologie, 6(1),12–25.
- Gass, M. A., Gillis, H. L., Russell, K. C. (2012). Adventure therapy: theory, research, and practice. New York, NY: Routledge.
- Hamanová, J. (2015). Dospívání a některé jeho zdravotní problémy [Adolescence and some of its health problems]. In J. Machová, D. Kubátová (Eds.), Výchova ke zdraví. Praha: Grada.
- Harper, N., Russell, K., Cooley, R., & Cupples, J. (2007). Catherine Freer Wilderness Therapy Expeditions: An Exploratory Case Study of Adolescent Wilderness Therapy, Family Functioning, and the Maintenance of Change. Child Youth Care Forum, 36, 111-129.
- Hendl, J. (2015). Přehled statistických metod: analýza a metaanalýza dat [Overview of statistical methods: data analysis and meta-analysis]. Praha: Portál.
- Hoskovcová, S., & Ryntová, L. (2011). Výchova k psychické odolnosti dítěte [Education for mental resistance of a child] Praha: Grada Publishing.
- Kalina, K. (2007). Psychoterapeutický proces v terapeutické komunitě. [Psychoteraputic process in therapeutic commuity] In P. Nevšímal (Ed.), Terapeutická komunita pro drogově závislé II: česká praxe (pp. 72-83). Praha: Středočeský kraj.
- Kalina, K. (2008). Terapeutická komunita. Obecný model a jeho aplikace v léčbě závislostí. [Therapeutic community. General model and its applications in addiction treatment] Praha: Grada Publishing.
- Kirchner, J. (2009). Psychologie prožitku a dobrodružství: pro pedagogiku a psychoterapii. [Experience and adventure psychology: for an education and a psychotherapy] Brno: Computer Press.
- Kraska-Lüdecke, K. (2007). Nejlepší techniky proti stresu. [The best techniques against stress] Praha: Grada.
- Křivohlavý, J., Schwarzer, R., & Jerusalem, M. (1993). Czech adaptation of the General Self-Efficacy Scale. Československá psychologie, 52(1), 1-19.
- Larson, B. (2007). Adventure Camp Programs, Self-Concept, and Their Effects on Behavioral Problem Adolescents. Journal of Experiential Education, 29(3), 313-330.
- Lewis, S. (2013). Examining changes in substance use and conduct problems among treatment-seeking adolescents. Child and Adolescent Mental Health, 18(1), 33-38.
- Magle-Habarek, N., Tucker, A., & Gass, M. (2012). Effects of Program Differences with Wilderness Therapy and Residential Treatment Center (RTC) Programs. Residential Treatment for Children & Youth, 29(3), 202-218.
- Maierová, E. (2010). Sebehodnocení klientů doléčovacího programu pro uživatele návykových látek. [Self-evaluation of clients of the aftertreatment program for drug users] Adiktologie, 10(1), 46-55.
- Mravčík, V. (Ed.) (2018). Annual Report on Drug Situation 2017 – Czech Republic. Praha: Úřad vlády České republiky.
- Pajares, F. (2007). Motivational Role of Self-Efficacy Beliefs in Self-Regulated Learning. In B. J. Zimmerman, & D. H. Schunk (Eds.). Motivation and Self-Regulated Learning: Theory, Research, and Applications (pp. 111-140). New York, NY: Erlbaum.
- Paquette, J., & Vitaro, F. (2014). Wilderness Therapy, Interpersonal Skills and Accomplishment Motivation: Impact Analysis on Antisocial Behavior and SocioProfessional Status. Residential Treatment for Children & Youth, 31(3), 230-252.
- Paulík, K. (2012). Psychologické aspekty zvládání zátěže muži a ženami. [Psychological aspects of the stress management of men and women] Ostrava: Ostravská univerzita.
- Radimecký, J. (2006). Očekávání pracovníků terapeutických komunit vs. proces změny chování klientů. [Expectations of therapeutic community workers versus clients´behaviour change process] Adiktologie, 6(1), 43–53.
- Rataj, M. (2007). Zátěžové programy. In P. Nevšímal (Ed.), Terapeutická komunita pro drogově závislé II: česká praxe (pp. 167-170). [Therapeutic community for drug addicts II: Czech practise] Praha: Středočeský kraj.
- Richterová, B., Štenclová, V., & Červenková, K. (2017). Adventure Therapy in therapeutic community Fides – Quantitative Outcomes of the research. AD ALTA: Journal of Interdisciplinary Research, 2(11), 181-184.
- Richterová, B., Takács, O., Pinďáková, J., Slivková, M., Tešnarová, D., Polášková, D., & Fešarová, V. (2015). Zátěžové aktivity a léčba drogově závislých. [Adventure therapy and drug addicts treatment] GRANT Journal, 4(1), 92–97.
- Romaněnková, E. (2012). Využití terapie dobrodružstvím v terapeutických komunitách v České republice. [Adventure therapy use in therapeutic communities in the Czech Republic] Praha: Univerzita Karlova v Praze. p.77. Available at: https://is.cuni.cz/webapps/zzp/detail /120219/?lang=en
- Scholz, U., Gutiérrez-Doña, B., Sud, S., & Schwarzer, R. (2002). Is general self-efficacy a universal construct? Psychometric findings from 25 countries. European Journal of Psychological Assessment, 18(3), 242–251.
- Šlachtová, A., Richterová, B., & Müller, I. (2019). Změny sebepojetí klientů terapeutickcýh komunit pro drogově závislé prostřednictvím terapie dobrodružstvím. [Changes in self-concept of therapeutic communities´clients addicted to drugs using the adventure therapy] Sociální pedagogika [Social Education], 7(1), 21–35.
- Wiegerová, A., Svatoš, T., Pavelková, I., Mareš, J., Hrabal, V., Ficová, L., & Gavora, P. (2012). Self efficacy v edukačných súvislostiach. [Self-efficacy in educational context] Bratislava: SPN–Mladé letá.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
07 November 2019
Article Doi
eBook ISBN
978-1-80296-071-6
Publisher
Future Academy
Volume
72
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-794
Subjects
Psychology, educational psychology, counseling psychology
Cite this article as:
Richterová, B. (2019). Programs Of Adventure Therapy And Drug Addiction Treatment In The Czech Republic. In P. Besedová, N. Heinrichová, & J. Ondráková (Eds.), ICEEPSY 2019: Education and Educational Psychology, vol 72. European Proceedings of Social and Behavioural Sciences (pp. 438-452). Future Academy. https://doi.org/10.15405/epsbs.2019.11.42