
Correlations Between Health, Occupational Stress Factors And General Attitudes In Primary Education

Abstract
240 questionnaires were administered during periodic medical checkup in a kindergarten, and four secondary schools. The questionnaires assessed the workers’ occupational stress factors and individual variables, health status (using ShortForm 36 questionnaire), irrational cognitions (General attitudes and beliefs Scale short version), positive as well as negative functional and difunctional emotions (Profile of Mood Disorders Short version-Romanian adaptation). In all the surveyed schools, age correlates significantly negatively only with positive emotions (p=0.001 for the whole group). In each school unit, the following variables are positively correlated as follows: social role functioning with physical role functioning (p = 0.00 for the whole lot), emotional role functioning (p = 0.00; whole lot) and general health perceptions (p = 0.00 for the whole group), whereas perceived vitality correlates with emotional role functioning (p = 0.00 for the whole group).The concordant results in all four school units show that perception of Quality of Life in terms of health refers primarily to emotional, social and physical components that are intercorrelated. Irrational cognitions as well as emotions (positive and negative) do not associate significantly with perceptions of health or occupational stressors. Functional negative emotions are more common in women than males (p = 0.016). Among the surveyed variables there are many correlations that are different according to the school unit, which underlines the importance of the organizational context and differentiated association of individual factors, and which entitles us to entertain the importance of organizational and individual approach for programs of stress reduction in the workplace.
Keywords: Anxietystress factorshealth statusagegeneral attitudes
Introduction
Currently, in Europe, 50-60% of work-related morbidity is attributable to work-related stress and this proportion is expected to increase in the future (International Labor Office, n.d.). This is a synthetic percentage, resulting from reports and evidence of occupational health and workplace services. However, this is the reported part, "the tip of the iceberg" but represents in fact an understatement of the real complex psychosocial phenomenon represented by the stress at the workplace. Identification of both individual or socio-occupational factors and organizational, protective or predisposing factors can help to identify and effectively combat sources of occupational stresses, identify and diagnose early dysfunctions and adaptive diseases, and also outline and apply methods of strengthening individual cognitive resources of prevention and / or resistance to stress.
Problem Statement
Perceived stress is one of the individual-environment transactions that can trigger or accentuate anxiety with contributing factors such as dysfunctional features of personality: anxiety, low self-esteem, cognition of individual achievement and comfort. The cognitive pattern of both anxiety and depression implies the presence of particular cognitive biases associated with dysfunctional coping and attention deficit disorders. Cognitive biases by overestimating the risk of occurrence of an event and by overestimating the severity of the event, associating the underestimation of the individual's ability to cope with the event, further associates stress side-effects. Depending on the intensity of perceived stress, behavioral reactions that occur in stressful situations are similar to those that highlight anxiety or some manifestations of depressive states: restless sleep, diminished appetite, diminished physical activity, attention-deficit disorders, sadness, loss of interest for things that are usually sources of pleasure. These behavioral responses are usually transient, attenuating or disappearing when stress stimuli no longer work. Chronic stress can, however, foster a regular dysfunctional response on a background of anxiety or depressive experiences, and these states - through a circular reaction - emphasize the intensity of the perceived stress. Functional emotions (positive or negative) reflect the presence of rational cognitions with adaptive consequences whereas dysfunctional (positive or negative) emotions reflect the presence of irrational cognitions, with disadaptive consequences. Contextual stress associated with dysfunctional emotions has an interdependence that emphasizes negative affective experiences and the individual’s stress perception, with health consequences (Ellis, & DiGiuseppe, 1993). The stressor associated with individual vulnerability factors (irrational cognitions) leads to dysfunctional affective states, symptoms or signs and / or behaviors that in turn increase or diminish the perceived level of the stressor (David, 2012). Further studies are needed to investigate the extent to which the organizational context can significantly influence different perception of levels of occupational stressors as well as the health status of employees or, on the contrary, the individual variability is the main element to be observed in the perception of occupational stressors in terms of affective experiences and complex cognitive structures of each employee.
Research Questions
The main research question is if perception of the health status correlates negatively with the perception of occupational stress factors, anxiety and general attitudes in primary education in all the surveyed school units. We also hypothesize that individual variables (age, residence, education) are likely not to correlate with perception of health, stressors or functional and dysfunctional emotions.
Purpose of the Study
The paper makes a comparative evaluation of the workers’ perception of occupational stressors by gender, type of residence, in five education units in Maramures county: i.e. a kindergarten and four secondary schools. An important point of interest of the present study was the assessment of the correlations between the workers’ perceptions of health status, occupational stress factors, anxiety and general attitudes of the participants in the surveyed educational units.
Research Methods
The questionnaires assessed the workers’ health status perceptions in terms of occupational stress factors, individual characteristics, anxiety and general attitudes. During the occupational medical check-up, performed at the units for 5 days in September 2017, the workers were asked to volunteer answering a questionnaire consisting of 5 parts:
A. The individual characteristics of the worker including: age, sex, type of residence (rural or urban).
B. Stressors present at the workplace were evaluated by a questionnaire with a 13-item four-point Likert scale indicating the perceived frequency of the respective stressor: 1 (absent), 2 (rare), 3 (sometimes) 4 (frequent). The questionnaire was based on data from the European Agency for Safety and Health at Work (EU-OSHA) for 7 groups of workplace stressors, namely: leadership, organization duties, career, role of decision-making and control, interpersonal relationships at work, job design, tasks and pace of work, work program (EU-OSHA, n.d.). Four more groups of frequent stressors encountered in education were added (Preda, 2010): daily completion of documents, difficulties in collaboration with pupils, difficulties in collaboration with parents, the need for extra work (Table
C. The SF-36 questionnaire used in evaluating individual worker health status consists in eight scaled scores, represented by the weighted sums of the questions in the section. The score represents a percentage of the maximum possible value (100%) of the respective domain of the scale, on each scale (Brazier, Roberts, & Deverill, 2002). The eight sections are: physical functioning, vitality, mental health, physical role functioning, bodily pain, emotional role functioning, social role functioning, general health perceptions (Ware, Snow, Kosinski, & Gandek, 1993).
D. General attitudes and beliefs Scale questionnaire, the short version measures the irrational cognitions and their three contents (achievement, approval, comfort), the subscales being the following: rationality, global evaluation of self value, the need to achieve, the need for approval, the need for comfort, the absolutist requirement of justice, the global assessment of others. The emotional distress generated by the awareness of desires in the form of needs is measured by four contents that express the need for accomplishment, approval, comfort and justice. The scale measures both dimensions of unconditional acceptance, both by the others and by oneself, dimensions that are involved in generating emotional distress (Lindner, Kirkby, Wertheim, & Birch, 2007).
E. Profile of Mood Disorders questionnaire Short version-Romanian adaptation (PDA) measures both positive emotions and functional negative emotions, as well as dysfunctional negative emotions on a 39-item scale. The scale allows the calculation of a global value of distress, a score of negative emotions (functional and dysfunctional), of a positive emotion score as well as scores for sadness "(functional)" worry " (functional)," anxiety " (dysfunctional), and "depression" (dysfunctional) (Opris, & Macavei, 2007). Statistical tests used: ANOVA, Bartlett's Test , Kruskal-Wallis test and Spearman correlation coefficient for correlations between questionnaires variables, p value was significant at 0.05.
Findings
There were 29 respondents in kindergarten, from a total of 38 employees. In school no.1, out of 58 employees, 53 questionnaires were completed. In school no. 2 there were 77 respondents form 88 employees. In school no.3, out of 42 employees, 33 questionnaires were completed and in school no.4 all participants completed the received questionnaires. The characteristics of the studied groups by gender are shown in Table
The proportion of urban employees is predominantly high in school no 1 and Kindergarten compared to the other schools, where the significant majority of employees are residents in rural areas. At the kindergarten, one fifth of the employees are rural residents (Table
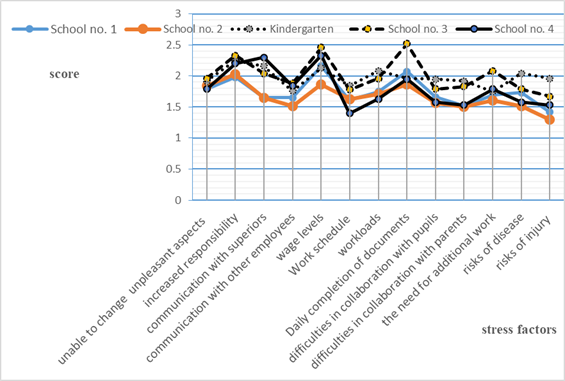
Some occupational stressors differ significantly (through frequency) according to school such as:
-"daily completion of documents"has a higher value(p=0.01) in School no. 1(average score 2.08) and School no. 3 (average score 2.5) compared with School no. 2 (average score 1.86);
"difficulties in collaboration with parents"has a higher value (p=0.01) in Kindergarten (average score 1.91) and School no. 3 (average score 1.82) versus School no. 2 (average score 1.5);
-"the need for additional work"has a lower value (p=0.04) in School no. 2 (average score 1.6) versus School no. 3 (average score 2.08);
-"communication with superiors" has a lower value (p=0.00) in School no. 1 and School no.2 (both with average score 1.64) versus School no. 4 (average score 2.3);
-"wage level" has a higher value (p=0.01) in School no.3 (average score2.45) versus School no. 2 (average score 1.86);
-"risks of disease" has a lower value (p=0.01) in School no. 2 (average score 1.51) versus Kindergarten (average score 2.04);
- "risks of injury" has a higher value (p=0.00) in Kindergarten (average score 1.95) versus School no. 2 (average score 1.3) (Fig.1.).
"Mean age", "general health perceptions", functional (and dysfunctional) emotions (negative and positive) and another individual characteristics of the worker do not present statistically significant differences according to the school unit.
Average scores of stress factors over 2 are considered elevated (never =1). The main stressors are represented by the daily completion of documents, wage levels, increased responsibility, with higher scores in School no. 3.
Depending on the school unit, the stressors that show significant differences in terms of the sex variable are only in the following situations:
- "difficulties in collaboration with pupils" are significantly higher stressors in women versus men only in School no. 3.
-" difficulties in collaboration with parents " are significantly higher stressors in women versus men only in School no. 3 (male average scores 1.2 versus women's average scores of 2) with p = 0.0033.
Depending on the school unit, only the following stressors show significant differences from the point of view of the residence variable:
- "communication with superiors" is a higher stressor (p = 0.01) only in School no. 2 in employees with rural residence (average of 1.75) versus those with urban residence (average of 1.21).
-"Work schedule" is a higher stressor (p=0.04) only in School no. 2 in those with rural residence (average of 1,73 ) versus those with urban residence (average of 1.21).
Also, only in School no. 2, "level of education" is higher (p=0.006) in those with urban residence (average of 4) versus those with rural residence (average of 3.26).
At the same time, the "age" variable is higher only in kindergarten at those with urban residence (with a mean of 46.86 years) compared to those with rural residence (average 35.5 years) without any significant differences in the other school units regarding residence
The stressor represented by "wage levels" was significant only in School no. 4, males had a higher score (mean of 3.5) versus women (mean of 2.19) with p = 0.017.
-"increased responsibility" only in School no. 1 is significantly higher (p=0.03) in females (average of 2,09) versus males (average of 1.28).
-"risks of disease" only in School no. 3 is significantly higher (p=0.008) in women (average of 1.94 ) versus (average of 1.2 ).
-"risks of injury " only in School no. 3 is significantly higher (p=0.01) in women (average of 1.49 ) compared with males (average of 1 ).
-"age"variable differs significantly according to sex only in School no. 4 being higher (p=0.04) in males (average 54.25 ani) versus the female employees (38.31 years).
There are numerous significant correlations of the subscales of the SF 36 questionnaire with the individual variables, the occupational stressors, the dimensions of the General attitudes and beliefs scale as well as the profiles of Mood Disorders Short version - Romanian adaptation (positive as well as negative functional and dysfunctional emotions) and their association being often different depending on the school unit.
For the school with the lowest number of respondents, School no. 4, the significant correlations of the subscales of the SF 36 questionnaire are the following:
-"social role functioning" with the following:
positive with "physical role functioning" (p=0.00), "emotional role functioning" (p=0.03), "mental health" (p=0.002) "bodily pain" (p=0.018) "general health perceptions" (p=0.037)
and negatively with: "unable to change unpleasant aspects"( p=0.002), "communication with superiors" (p=0.020), "increased responsibility" (p=0.000), "risks of injury"(p=0.013), "communication with other employees" (p=0.005), "workloads" (p=0.000), "Work schedule" (p=0.004)
positive with "total positive emotions" (p=0.025), "physical role functioning" (p=0.015), "mental health"(p=0.022), "general health perceptions" (p=0.012)
and negatively with: "unable to change unpleasant aspects" (p=0.024), "increased responsibility" (p=0.019), "risks of disease" (p=0.008), "risks of injury"(p=0.018), "communication with other employees" (p=0.015);
-"physical role functioning", positive with: "rationality"(p=0.002) "total positive emotions"(p=.027), "emotional role functioning"(p=0.003), "mental health"(p=0.011), "social role functioning"(p=0.000), "bodily pain"(p=0.035), "general health perceptions"(p=0.034)
and negatively with: "unable to change unpleasant aspects"(p=.0018), "increased responsibility" (p=0.003), "risks of injury" (p=0.000), "communication with other employees" (p=0.001), "workloads" (p=0.005);
-"emotional role functioning" has only negatively correlations as folows: "self" (p=0.009), "social role functioning"(p=0.036), "unable to change unpleasant aspects" (p=0.007), "increased responsibility" (p=0.017), "risks of disease" (p=0.026), "risks of injury" (p=0.007), "workloads" (p=0.011);
-"vitality" has negatively correlation only with "total negative functional emotions"(p=0.027) and positive with the folowing: "total positive emotions" (p=0.006) "mental health"(p=0.000), "general health perceptions" (p=0.028);
-"mental health" ", positive with: "total positive emotions" (p=0.031), "physical functioning" (p=0.022), "physical role functioning" (p=0.011);
and negatively with: "total negative functional emotions" (p=0.037), "unable to change unpleasant aspects" (p=0.020), "increased responsibility" (p=0.016), "workloads" (p=0.045);
-"bodily pain" positive with "rationality" (p=0.033) and negatively as follows: "self"(p=0.031), "communication with superiors" (p=0.001)"increased responsibility" (p=0.008), "communication with other employees" (p=0.000), "workloads" (p=0.015);
-"general health perceptions" positive with: "total positive emotions" (p=0.025) "physical functioning" (p=0.012) "physical role functioning" (p=0.034) "vitality" (p=0.028)
and negatively with: "increased responsibility" (p=0.0019), "total negative functional emotions" (p=0.049).
Other school units have significant correlations only for both of the dimensions "social role functioning" and "general health perceptions" of the subscales of questionnaire SF36 subscales.
Conclusion
Among the surveyed variables there are many correlations that are different according to the school unit, which underlines the importance of the organizational context and differentiated association of individual factors. This entitles us to entertain the importance of organizational and individual approach for programs of stress reduction in the workplace.
The complexity of interdependence between different organizational occupational stressors and the individuality of cognitive structures that associate them with instances and patterns of affective experiences, contextually modulated, determine a polymorphism of associating employees’ perceptions of health with both occupational stressors, anxiety and irrational cognitions.
The concordant results in all four school units show that perception of Quality of Life in terms of health refers primarily to emotional, social and physical components that are intercorrelated.
Irrational cognitions as well as emotions (positive and negative) at organizational level do not associate significantly with perceptions of health or occupational stressors.
The descriptive perspective of statistical indicators of scale parameters on perceptions of health, stressors, irrational cognitions, functional and dysfunctional emotions offers a general picture with organizational features that requires, after evaluating their level and applying general corrective measures, the individual approach with the help of the psychologist.
Based on these results, the perception of the health status of the employees in education from the point of view of the occupational stressors, the perspective of individual approach and evaluation as well as the individualized mechanisms of coping in which the psychologist has a key role, are essential.
References
- Brazier J.E., Roberts J., Deverill M., (2002).The Estimation of a Preference-based Measure of Health from the SF-36 . Journal of Health Economics, 21, (2), pp. 271-292.
- David D. (2012). Tratat de psihoterapii cognitive și comportamentale, Polirom, Iasi
- Ellis, A., DiGiuseppe, R. (1993), Are inappropriate or dysfunctional feelings in rational-emotive therapy qualitative or quantitative?, Cognitive Therapy and Research, 17, 471-477 .
- Lindner, H., Kirkby, R., Wertheim, E., Birch, P.(2007). Scale of attitudes and general beliefs (adapted by Trip, S.). In D. David (coordinator), Sistem de evaluare clinică .[Clinical evaluation system]. Ed. RTS, Cluj Napoca
- Opriș, D. și Macavei, M. (2007). The profile of affective distress. In D. David (coordinator), Sistem de evaluare clinică [Clinical evaluation system]. Ed. RTSD, Cluj-Napoca.
- Preda, V.-R. (2010). Effects of stress and coping strategies on teachers and pupils, PhD Thesis, Babes Bolyai University, Faculty of Psychology and Education Sciences.
- Ware, J.E., Snow, K.K., Kosinski, M., Gandek, B. (1993). SF-36 Health Survey. Manual and interpretation guide. Boston: The Health Institute, New England Medical Center.
- EU-OSHA, European Union Information Agency for Occupational Safety and Health. (n.d.). Psychosocial risks and stress at work Retrieved September 15, 2018, from: https://osha.europa.eu/ro/themes/psychosocial-risks-and-stress
- Internațional Labour Organization . (n.d.). Psychosocial risks and work-related stress
- Retrieved September 15, 2018, from: https://www.ilo.org/safework/areasofwork/workplace-health-promotion-and-well-being/WCMS_108557/lang--en/index.htm
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
15 August 2019
Article Doi
eBook ISBN
978-1-80296-066-2
Publisher
Future Academy
Volume
67
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-2235
Subjects
Educational strategies,teacher education, educational policy, organization of education, management of education, teacher training
Cite this article as:
Triff*, D. (2019). Correlations Between Health, Occupational Stress Factors And General Attitudes In Primary Education. In E. Soare, & C. Langa (Eds.), Education Facing Contemporary World Issues, vol 67. European Proceedings of Social and Behavioural Sciences (pp. 1325-1333). Future Academy. https://doi.org/10.15405/epsbs.2019.08.03.163