
The Importance Of Physical Therapy As Mean For Correcting Clubfoot (Varus- Equin)

Abstract
Left untreated, congenital clubfoot gradually worsens, causing the faulty positions to become permanent and irreversible; however, if a correct kinetic treatment is in place and applied on time, both statics and locomotion can be improved. The purpose of this work is to present the specificities (characteristic particularities) and reasoning of our multiple phase kinetic treatment in acquiring an aesthetic, functional, pain-free and plantigrade foot, as well as to check the kinetic treatment’s outcomes (effectiveness and security) applied for the clubfoot’s recovery in the adolescent patient. The principles to have guided the kinetic treatment programme’s development were connected with the biomechanics specific to the joint complex of the foot, taking account of the clinical and functional status and implicitly, patient’s age. The kinetic treatment strategy was achieved by gradually increasing the number of physical exercise, depending on the rehabilitation process stages, seeking to get a balance between invertor and evertor muscles to achieve adequate foot cinematics. Our study assessed the influence of musculoskeletal changes over movement mechanics on a 14-year old patient with clubfoot, untreated surgically. The data collected before and after the kinetic treatment was applied showed a functional progress, with a significant improvement both of the range of motion and muscle strength of the foot, thus contributing to the improvement of walking and the carry out of physical exercise. Using the specific kinetic methods and techniques rationally, significant reduction of pain and improvement of foot aesthetics were achieved, with a substantial contribution on our patient’s mental state.
Keywords: Clubfoot (varus - équin)physical therapydeformities
Introduction
Clubfoot (
Idiopathic clubfoot is bilateral in approximately half the cases; males are reported to be more affected than females. Although there is a consensus on the fact that males are more affected than females, there isn’t one with regard to the existence of a difference in the severity of the disease which can be attributed to gender (O’Shea & Sabatini, 2016).
With respect to the treatment for this condition of the foot, there have been numerous studies over these past years that have proved the short-term effectiveness of nonoperative treatment both for recovery, and for reduction of the need for surgery (Richards et al., 2008).
At present, there are limited studies about the incidence, nature and severity of symptoms in adults with clubfoot, but they suggest that symptoms increase and function diminishes with advancing age (Brodsky, 2010).
Problem Statement
This paper aims to present the theoretical and practical aspects of clubfoot during adolescence.
No matter the treatment carried out, the relapse tendency in clubfoot is high. Some of the predisposing factors of relapse consist in the rigid clubfoot and the child’s tender age, while in children with ligament laxity, clubfoot relapse is very low. Frequency of relapses decreases after the age of 4 (Ponseti, 2002).
There are differences with regard to treatment of clubfoot in a new-born and in a teenager (untreated clubfoot); they consist in the fact that foot is easier and faster to repair in new-borns, and repair is more difficult and takes longer in teenagers. Kinetic treatment of clubfoot should begin as soon as possible, immediately after birth. It consists in reducing basic deformities. Therefore, getting a valuable result depends on the time kinetic treatment is begun, as well as on how rigorous therapeutic sequences are. Establishing an individualised kinetic treatment program requires specialized experience and knowledge of design and supervision.
Kinetic treatment aims to carry out and maintain optimal relation between tibia and ankle bone joints, ankle bone and heel bone, heel bone and cuboid, but also the other disturbed joints; achieve optimal muscular relation both between invertor and evertor muscle formations of the foot, as well as between flexor and extensor formations of the foot.
To regain foot functionality, normal aspect and good mobility, pathogenesis of clubfoot needs to be understood, as well as effects of treatment carried out, not only in terms of foot correction, but also the long-term results and quality of life for the treated foot (Dobbs, Morcuende, Gurnett, & Ponseti, 2000).
Research Questions
Considering the complexity of the intervention plan recalled by the literature for subjects with congenital clubfoot, this study raises the following questions:
Can kinesiotherapy be deemed as an effective means of correction in clubfoot subjects?
Is kinesiotherapy a high potential method to repair clubfoot in teenagers?
Purpose of the Study
The purpose of this paper is to develop a multi-phase kinetic treatment programme to ensure an aesthetic, functional, pain-free and plantigrade foot, as well as to check the kinetic treatment’s outcome (effectiveness and security) applied for the repair of clubfoot.
Research Methods
To set up the background information in support of our research purpose, the following research methods were used:
- bibliographical research method - to make the approached theme’s theoretical profile,
- observation method - to view and assess the progress of the subject’s joint dysfunction throughout the study,
- tests method - to confirm/ infirm the efficiency of the kinetic treatment carried out using initial and final assessments made to the subject about joint amplitude.
- basic statistics methods (numerical and graphic methods) - to render the evolution and trends of the data collected, variables of statistical interest – quantitative- wise such as age, dorsal flexion (degrees) before and after the kinetic treatment is carried out, plantar flexion (degrees) before and after the kinetic treatment is carried out, abduction (degrees) before and after the kinetic treatment is carried out, adduction (degrees) before and after the kinetic treatment is carried out and related to categories such as gender (male/female), origin background (urban/rural) and the affected foot (right/left).
Representation of the data gathered found the basic notions of the study as well as directions to apply practical conclusions about the effectiveness of the kinetic treatment underwent by the subject with congenital clubfoot.
Findings
This paper proposes a case study: a 14 year old male patient, diagnosed with unilateral congenital clubfoot; he had been subjected to passive correction by cast and kinesiotherapy. When examined, the right foot’s abnormal position was found; it was rotated inwards (varus). Walking was impaired, deformed and steps were unequal. Prancing gait was thus noticed. Heel walk was not possible, as the patient couldn’t position his foot in eversion. Further to evaluation of joint mobility, amplitude deficit was found out on all movements.
We hypothesize that by using a multi-phase, supervised kinetic treatment programme, gradually increasing physical activities, featuring specific methods and techniques for muscle tone and flexibilization, the outcome will consist in an aesthetic, functional, pain-free and plantigrade foot.
Basically, the intervention plan applied included general information about clubfoot, specific clinical manifestations, kinetic treatment, insisting on the correct execution of exercises. We used a language of communication suitable to the subject’s level of understanding in order to explain the most important aspects of clinical and therapeutic management of the disease as clear as possible.
The operational objectives of the kinetic treatment carried out to repair the foot joint were: improve dorsal flexion, plantar flexion, abduction, and adduction, muscle strength of the foot / lower limb, controlled stability and ability.
To achieve the operational objectives proposed, kinetic treatment included the following techniques:
To improve joint mobility of the foot: akinetic techniques, passive dynamic kinetic techniques, active dynamic kinetic techniques, stretching techniques, neuromuscular facilitation techniques;
To improve muscle strength of the foot: static kinetic techniques, active dynamic kinetic techniques, neuromuscular facilitation techniques;
To improve controlled stability and ability of the foot: active dynamic kinetic techniques, neuromuscular facilitation techniques.
Research results
Next, we will present the patient’s evolution during the period 5 August 2017 – 5 June 2018. Comparison of the tests results in the two assessments (initial and final) using tables (Table
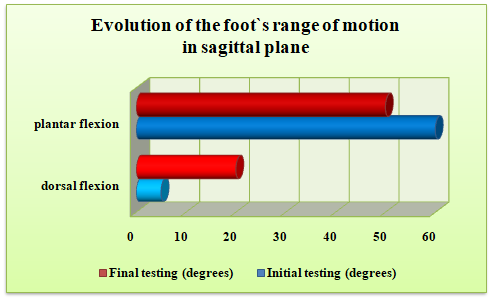
Evolution of ranges of motion in sagittal plane- dorsal and plantar flexion.
Foot’s dorsal flexion improved by about 150 after the exercises to correct clubfoot were performed.
Plantar flexion was also improved, within the meaning that clubfoot was reduced from 600 to 500. This is a significant evolution in an adolescent patient with congenital clubfoot who did not undergo any surgery previously.
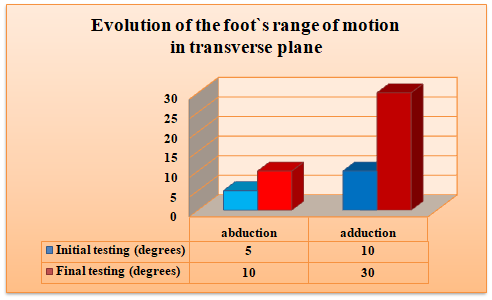
Evolution of the range of motion in transverse plane - abduction and adduction.
The foot’s abduction movement registered an increase by approximately 50 after the specific kinetic programme was carried out.
The adduction motion, as expected, registered the most significant improvement of mobility, starting from only 100 going up to 300, so a visible improvement of 200.
Mention should be made that the presence of pain impacts the overall functional capacity of the patient with clubfoot, affecting usual activities in a negative way, giving a significant disability.
After the program was carried out, there was a significant reduction of pain, which thus shows that kinetic treatment was effective.
The unaesthetic shape of the foot was one of the main patient dissatisfactions, as this was one of the characteristics of the discussions in this study.
At the end of the specific kinetic treatment carried out, the shape of the patient’s foot was significantly improved.
All this progress made (increase of joint mobility, pain reduction and improvement of foot’s aesthetics) gave the patient self-confidence and stronger will to keep carrying out the kinetic therapy; the patient stated that the kinetic treatment carried out was beneficial both physically and mentally, giving him more energy, self- respect and improving his communication to other people.
Conclusion
The repair methods used to treat clubfoot are extremely varied depending on school, starting from successive long casts placed as outpatients to foot manipulations twice a day under prolonged hospitalisation.
The foot’s joint complex, adapted to the forces and loads acting over it has contact points, pressures and axes that are affected in clubfoot. This joint complex forms a kinetic connection linking the lower limb to the ground, a key condition both to achieve walking, and to perform other day to day activities. In this context, development of the kinetic treatment strategy depending on the clinical and functional status and the patient’s age with gradual increase of physical activities depending on the intervention process’s stages has demonstrated a functional evolution, thus leading to a valuable outcome as to walking and day to day activities of the patient with clubfoot. The use of specific methods and techniques for muscle tone and flexibilization of kinetic therapy led to a significant improvement of the range of motion and muscle strength of the patient with clubfoot. Therefore, kinetic treatment should be the first option irrespective of the Dimeglio score or the patient’s age; this fact was demonstrated by the positive outcome registered by this study’s patient, who is a teenager who has not undergone any surgery. In order to get a successful functional outcome in approaching kinetic treatment of clubfoot, it is absolutely necessary to apply methods and techniques by complying with the basic biomechanical principles and anatomical features of the area concerned. Thanks to the therapeutic massage and passive mobilisation techniques, tissue is both relaxed and warm, and muscular retractions are prevented.The earlier the condition is treated, the better and faster the results will be. What’s more, articular stiffness occurring after muscular retractions will be prevented. A child born with clubfoot will never have a normal foot in adulthood. Sequalae present at the end of growth will intensify during adult life. Apart from pain, instability and long-term related sequalae, clubfoot will also affect the patients’ quality of life both economically, and socially (Besse, Leemrijse, Thémar-Noël, & Tourné, 2006). Nonoperative management of clubfoot requires specialists to have good knowledge and a close interdisciplinary co-operation (and to parents too) in order to achieve significant results.
References
- Besse, J. L., Leemrijse, T., Thémar-Noël, C., Tourné, Y., & Association Française de Chirurgie du Pied. (2006). Congenital club foot: treatment in childhood, outcome and problems in adulthood. Revue de Chirurgie Orthopedique et Reparatrice de l’Appareil Moteur, 92(2), 175-192. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/16800074
- Brodsky, J.W. (2010). The adult sequelae of treated congenital clubfoot. Foot and Ankle Clinics, 15(2), 287-296. DOI:
- Dobbs, M. B., Morcuende, J. A., Gurnett, C. A., & Ponseti, I. V. (2000). Treatment of idiopathic clubfoot: an historical review. The Iowa Orthopaedic Journal, 20, 59-64. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/10934626
- O’Shea, R. M., & Sabatini, C. S. (2016). What is new in idiopathic clubfoot? Current Reviews in Musculoskeletal Medicine, 9(4), 470-477. DOI:
- Ponseti, I. V. (2002). Relapsing clubfoot: causes, prevention, and treatment. The Iowa Orthopaedic Journal, 22, 55-56. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1888384/
- Richards, B. S., Faulks, S., Rathjen, K. E., Karol, L. A., Johnston, C. E., & Jones, S. A. (2008). A comparison of two nonoperative methods of idiopathic clubfoot correction: the Ponseti method and the French functional (physiotherapy) method. The Journal of Bone and Joint Surgery. American volume, 90(11), 2313-2321. DOI: 10.2106/JBJS.G.01621.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
15 August 2019
Article Doi
eBook ISBN
978-1-80296-066-2
Publisher
Future Academy
Volume
67
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-2235
Subjects
Educational strategies,teacher education, educational policy, organization of education, management of education, teacher training
Cite this article as:
Neagoe*, I. C., & Burcea, C. (2019). The Importance Of Physical Therapy As Mean For Correcting Clubfoot (Varus- Equin). In E. Soare, & C. Langa (Eds.), Education Facing Contemporary World Issues, vol 67. European Proceedings of Social and Behavioural Sciences (pp. 1283-1288). Future Academy. https://doi.org/10.15405/epsbs.2019.08.03.158