
Disclosure Tuberculosis Stigmatized Identities And Its Workplace Implications In Pakistan

Abstract
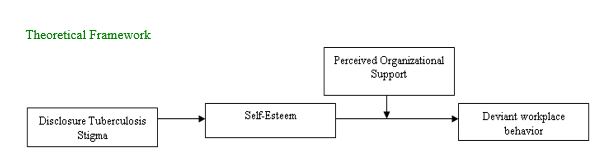
The current research study identified employee’s deviant behavior as an outcome of disclosure Tuberculosis stigmatized employees at workplace. Study indicates that self-esteem acts as an interlinking mechanism between disclosure TB stigma and deviant workplace behavior. Similarly, perceived organizational support act as a moderating role between self-esteem of TB stigmatized individuals and negative workplace outcomes at public and private hospitals of Pakistan. Data were collected from 321 middle and low level TB diagnosed employees. Social identity theory has been used as an overarching theory that supports the theoretical framework. Findings of hypothesized model showed that disclosure TB stigma has positive impact on self-esteem. Results identified that that low self-esteem increase the deviant behaviour of disclosure TB stigmatized employees. Moreover, the hypothesis has been rejected that perceived organizational support as a moderating variable between self-esteem and deviant workplace behaviour. In current research data has been collected through self-administered questionnaires in three time lag survey design;.
Keywords: Disclosure TB stigmaself-esteemdeviant workplace behavior
Introduction
In today’s competitive world workplace has become an important place where employees spend maximum amount of time with other organizational members instead of their family and friends. It is important for organization to consider the behaviors of their workforce either positive or negative. Most of the management science literature recognized that the reason of poor organizational performance is deviant workplace behaviour (DWB) (Metofe, 2017). Moreover, at workplace each individual employee is known by his/her own identity. At workplace these identities relate with positive and negative behaviors. Though, studies identified that in different social settings individuals develop a sense of identity, on the basis of these identities they belong to certain category, class or group. Similarly, social identity theory explained that due these social settings, stigmatized individuals remain separate themselves from non-stigmatized individuals (Hogg & Turner, 1987).
The social psychologists identified these attitudes and beliefs as a term known as stigma. The term stigma is used primarily for the person who considers misfortune in itself. It's a term that makes an individual less than the rest of people because of some features that are not worthy compared to the rest of the people. It is a mark, an attribute that creates the different identity of an individual (Goffman, 1963). Accordingly, individuals belongs to stigmatized group develop their separate identity, these devalued identities at workplace associated with negative behaviors. In management science literature there is a lack of attention on employee’s identities known as stigmatized identities, the current research paid attention in this area.
Problem Statement
One of the most important problem faces by public or private organizations is the negative behaviors of their employees. There is a plenty of research has been conducted on negative behaviors of workforce in the literature of social science but still there are some important aspects has received little attention. As we know unfortunately Pakistan is consider as a third world country. Different issued related to employees poor health and unemployment enhance day by day. There is lot of studies regarding these issues but still little attention on those aspects creates employees deviant behaviors. Pakistan is fifth among the countries with a high burden of tuberculosis in the world. At workplace employees diagnosed with TB become stigmatized. The impact of the stigma induced by tuberculosis in the workplace has received little attention from management researchers. Current study has explored that negative workplace behaviors of employees become reduce by disclosure of TB induce stigma through interlinking mechanism of self-esteem.
Research Questions
How disclosure reactions of TB induce stigma is positively related with self-esteem?
Does self-esteem mediate in the relationship between valance content (disclosure) of TB induced stigma and deviant workplace behavior?
Does perceive organizational support moderates in the relationship between SE and DWB of TB infected individuals such that negative relationship reduce with greater POS?
Purpose of the Study
The developing countries like Pakistan are amongst 30th highest countries that have high rate of Tuberculosis patients. The rate of unemployment is also high in these countries. People with serious infectious diseases like tuberculosis develop their separate identity known as stigmatized. At workplace employees exhibits negative behaviors due to different reasons but still there is gap to identify those factors that enhance workforce negative behaviors. The purpose of this research study is to identify actual identities of infected individuals at workplace that not only impact on employee’s psychological factor but also employees behaviors at workplace. This purpose of study is to contribute in the social-psychological literature that disclosure TB stigma has an impact on employee’s deviant workplace behavior. In like manner study also focus on self-esteem as an interlinking mechanism and some external factors like organizational support.
Researchers have studied that people become stigmatized due to Tuberculosis (TB).It is a doubtlessly fatal infectious disease that normally influences not only the lungs of patients, but can have an effect on any part of the body (Juniarti & Evans, 2011).The international report by world health organization regarding tuberculosis in (Organization, 2008), confirmed that (TB) is a serious infectious disease at different parts of the world and delay its treatment become the cause of death. Tuberculosis infected individuals become stigmatized because they consider their selves as devalued. In addition, the stigma associated with TB reduce treatment adherence (Ngamvithayapong, Winkvist, & Diwan, 2000). At workplace those employees diagnosed by (TB) face negative consequences; The first one is hiring discrimination because of a records of TB, secondly most of the infected employees due to (TB), face harassment and hostility of colleagues once they return to work, denial of diversifications at work, loss of process duties without basis, reassigning work features or degradation as well as denial of advertising or growth of salary and reduction of income, and requests to voluntarily step down from one’s role or process termination/dismissal. Finally, fears of being stigmatized can affect survivors’ disclosure choices (Stuart et al., 2004).
Many TB survivors have reported snitching with the decision to disclose their actual identity at workplace with their boss, co-workers because of fear of job loss, and limited opportunity for career advancement. There are numerous studies conducted on the stigmatization of TB patients worldwide (Aryal, Regmi, & Mudwari, 2012). Studies demonstrated that maximum number of tuberculosis infected individuals survives in densely populated countries. The higher ranked countries of TB infected patients are India and Pakistan(Dye, 2006).Recent work suggests that disease related stigma is less studied in Asian countries(Brohan, Slade, Clement, & Thornicroft, 2010).A few studies have been conducted on disease based stigma like AIDS and HCV in Pakistani context at workplace domain(Bashir, Nasir, Qayyum, & Bashir, 2012; Noor, Bashir, & Earnshaw, 2016).The present study investigates disclosure Tuberculosis stigmatized identities and its workplace outcomes (deviant workplace behavior) through interlinking mechanism of self-esteem that are less studied in previous psycho-social literature.
Stigmatized individuals at workplace enhance their negative behaviors because of low self-esteem. In addition, tuberculosis stigmatized individuals has negative impact on their self-esteem (Moya, Biswas, Chavez Baray, Martínez, & Lomeli, 2014). Disclosure of stigma can provide the opportunity to express hidden thoughts, feelings and emotions with those closest to you. It also creates a sense of self in stigmatized individuals. It will be useful for the well-being of infected people (Chaudoir & Fisher, 2010). One of the previous study conducted on lesbian mother identified that those people disclosed about the identity of their parents with others have higher self-esteem (Gershon, Tschann, & Jemerin, 1999). Most of the previous studies paid attention about internal stigmatization and its negative psychological outcomes (poor self-esteem). Thus, the current research scrutinize that when individuals disclose stigmatized identities, either at workplace or with family and friends that will positively related with self-esteem. It appears that disclosure TB stigmatized identities and its positive impact on self-esteem. It is a distinctive approach that has been less discusses in organizational context.
In organization employees with poor self-esteem mostly show negative behaviors at job. Their poor confidence and lack of esteem engage them in destructive activities at workplace (Chirasha & Mahapa, 2012). Researchers has shown that disclosure stigma empower individuals that increase that associated with positive self-esteem (Corrigan, Faber, Rashid, & Leary, 1999). In organizations, employees with high self-esteem do not participate in these negative activities. They avoid deviant behavior at the workplace because of high self-esteem. The high trust due to the disclosure of their negative characteristics with collaborators has made them safer and less engaged in diversion activities (Avey, Palanski, & Walumbwa, 2011). With the support of organizational support theory, (Viswesvaran et al., 2005) and (Rhoades, Eisenberger, & Armeli, 2001), empirically investigated that positive perceptions of employees towards their organization helped them to establish a great psychological attachment to the organization.
Authors depicted that social identity theory (SIT) provides a strong theoretical explanation of the present model. It provides foundation to investigate TB infected stigmatized individuals at workplace. According to (Hogg & Turner, 1987) due to social interaction individuals develop a sense of identity and group of stigmatized identities belong to specific category or group that will differentiate them from non-stigmatized group of people. Hence, stigmatized identities bridge the gap between stigmatized group of individuals and non-stigmatized group. Theory also revealed that on the basis of social- categorization mostly people classified their identities into in-group and out group. The one of the core function of these classified groups are their self-esteem. Social identities boost self-esteem of individuals within group and become reduce when they interact with out group. At workplace stigmatized individuals classified their separate identity and have impact on negative workplace behaviors (Bowles & Gelfand, 2010).
Literature Review
Disclosure (Tuberculosis) stigmatized identities and self-esteem
Psychologist on stigma identified that people with devalued identities generate positive and negative beliefs. Whenever they feel support from others they share their invisible attributes with others to build up their confidence. These attributes are known as disclosure of stigmatized identities or disclosure reactions victimized by chronic illness (Quinn & Earnshaw, 2011). In a supportive environment stigmatized identities reveal their values with others; this revelation process affects the people through two different mechanisms. Disclose stigmatized attributes with non stigmatized people mostly depends how much they receive social support, that encourage them and educate them that to disclose their actual identities (Chaudoir & Fisher, 2010). These disclosures reactions increase their confidence and positively impact their trust level (Zolowere, Manda, Panulo, & Muula, 2008).
On the other hand, studies identified patients with tuberculosis who should not disclose their stigma identities are facing barriers to obtaining support from friends, family members and spouses (Daftary & Padayatchi, 2013). The recent study regarding (TB) stigma found that only few people have confidence and positively evaluate themselves to disclose their disease (Hayes-Larson et al., 2017). Much has been said about the positive influence of social support on feelings of self-esteem, on the quality of life, on the success of professional and educational goals and on adherence to medical care is due to when people try to disclose their negative attributes with supportive ones (Hanghøj & Boisen, 2014). It has been found that the disclosure reaction offers above all advantages such as improving the self-esteem of the stigmatized people and promoting physical health (Pérez-Garín, Molero, & Bos, 2017).
Moreover, the openness to the diagnosis of the family, instead of avoiding it, can improve patients' self-esteem (Omiya, Ito, & Yamazaki, 2014). They also examined that educating and raising awareness in terms of revealing stigmatized identities improves their self-esteem (Adhikari, Kaehler, Chapman, Raut, & Roche, 2014). Therefore, from the previous literature of positive valence content i.e. disclosure of disease based stigma and its positive association with self-esteem, we hypothesized as,
H1: Disclosure of (TB) stigma is positively related with individual’s self-esteem
Self-esteem (mediating variable) as an interlinking mechanism in the relationship between disclosure tuberculosis stigmatized identities and deviant workplace behavior
Management scholars investigated different facts that those individuals trust on their abilities and values, they become more confident, they develop their own self-concepts such type of phenomenon is known as self-esteem(Baumeister, 2013; Rosenberg, Rosenberg, & McCord, 1978).Social identity theory by (Tajfel & Turner, 1979) also supports the above argument and explained that individuals try to improve their self-esteem to become the part of social group, to develop their identity. In spite of this, social psychological theory of the role of self-conception identified that individuals in their social interaction develop sense of identity. Additionally, those people belong from devalued group of identities; they categorized their identities different from other groups and linked their identities with stigmatized group of people and in prior studies stigmatization has negative impact on self-esteem (Hogg & Terry, 2000). Stigmatized people with their disclosure reactions mostly link with self-esteem (Zea et al., 2005). At workplace, the disclosure reactions of stigmatized workforce positively link with high esteem. The high confidence due to disclosing their negative attributes with co-workers made them more confident and less engaged in deviance activities (Avey et al., 2011). The first reason is that their positive esteem and worth at job motivate them to do their job well. Secondly, their confidence will increase their performance. These are the responses that people wants to establish their esteem (Rotundo & Sackett, 2002; Viswesvaran et al., 2005). The theoretical narratives highlighted the path to self-acceptance that was often imbued with oppression experiences; however, the participants told stories of remarkable patience, perseverance, strength and emerging confidence (Austin, Lee, & Fine, 2016).
Most of the prior literature demonstrated that when stigmatized people disclose their attributes and receive more supportive reactions, they become fearless to disclose their attributes in next situations. Indeed, also found the positive association between disclosure of stigmatization and self-esteem (Quinn & Chaudoir, 2009). People with a high level of self-esteem or self-confidence will be less committed to aggressive or deviant behavior in the workplace. They have originated that self-esteem is one of the important predictors that is related to different behaviors in the workplace. People who try to maintain their identity that who they are? Their value inside the organization with their co-workers reduce their deviant behaviors (Avey et al., 2011). Furthermore; the above arguments identified that individual’s poor self-esteem positively associated with negative valence content as well as high self-esteem linked with disclosure of tuberculosis stigmatized reactions. The high and low self-esteem at workplace also associated with deviant workplace behavior. On the basis of existing literature current study hypothesized as,
H2: SE act as mediating variable in the relationship between disclosure TB stigma and deviant workplace.
Pos act as a moderating variable between self-esteem and deviant workplace behavior
The support of organization towards their employee’s increases the overall productivity of organization. This concept was first introduced that identified employees positive perception towards their organization is known as perceived organization support (POS) (Eisenberger, Huntington, Hutchison, & Sowa, 1986). Secondly, when organizations enhance their association with their employees, at that extent employees develop a general perception, that their organization cares about their well- being and respect (Kurtessis et al., 2017). Most of the employees at workplace diminish their negative behaviors when they perceive support from their organization. More support from department increase employee’s self-esteem.
To improve their working environment, employees focus on organizational support. It invokes trust, provides a source of high self-esteem among their employees and helps to satisfy their existential needs (Törner, Pousette, Larsman, & Hemlin, 2017). With the support of social psychological literature, people suffer from serious infectious and chronic diseases such as (Tuberculosis). They labeled this disease as a part of their devalued identities; they become stigmatized and known as (TB) stigmatized people. Most of the studies on stigmatization identified that; these devalued identities reduce individual’s self-esteem (Quinn & Earnshaw, 2013). Indeed, disease based stigma negatively affects the hope and self-esteem of individuals (Yanos, Roe, Markus, & Lysaker, 2008). Since, in organizational context low self-esteem is associated with drastic negative results, such as deviant behavior in the workplace (Ferris, Brown, Lian, & Keeping, 2009).
Employees who identify a lot with their organizations are more likely to contribute to achieving organizational goals (Edwards & Peccei, 2010; Frenkel & Yu, 2011). Workers benefit from socio-emotional resources and improve their skills to carry out their tasks within the organization and less involved in deviance behaviors (Battistelli, Galletta, Vandenberghe, & Odoardi, 2016). Some scholars argued that the perceived support of the organization acts as a double-edged sword for both employees and organizations (Li, Chiaburu, & Kirkman, 2017). This sword will strong employees psychological process and boost their self-esteem. Such supportive responses from organization mostly increase employee’s positive esteem (Vardaman et al., 2016).
Research found different negative behavioral outcomes at workplace. They examined that perceived organizational support has the ability to diminish these negative behaviors (Vatankhah, Javid, & Raoofi, 2017). The previous literature also shows that deviant workplace behaviour decreases productivity and performance (Yasir,& Rasli, 2018). The negative behaviors will be reducing by highest perceived organizational support (Yildiz & Yildiz, 2015). Therefore; people with high POS will enhance the self-esteem of employees that will reduce the negative workplace behaviors. Hence, this study hypothesized as,
H3: POS act as a moderating variable between self-esteem and deviant workplace behaviors. It decrease the negativity between self-esteem and DWB of people diagnosed with (Tuberculosis) at workplace.
Research Methods
Research Design
Management science researchers consider quantitative research methodology to obtain the data from respondents. To increase effectiveness of the study as well as to obtain tremendous results a good research design help research scholars (Wiersma & Jurs, 2005). With the support of this research design researchers become able to achieve authentic results (Chase, Teel, Thornton-Chase, & Manfredo, 2016).
Population and Sample
From October, 2017 to March 2018, data were collected from contact people diagnosed with tuberculosis in several public and private Tuberculosis hospitals across different provinces Pakistan as well as state of Azad Jammu & Kashmir. The reason to conduct study in this sector is that Tuberculosis is an infectious and epidemic like HIV/AIDS especially at workplace. One of the past study identified that healthcare professionals working with people diagnosed TB experience discrimination against their peers for fear of contagion and association with "improper or immoral behavior" (Siegel et al., 2015). The second important reason to conduct this study in country like Pakistan is the most appropriate. World health organization clarified number of cases regarding tuberculosis in Pakistan and consider among the top 30 countries in the world (Organization, 2016).
We contacted the medical superintendent (MS) of the public and private hospitals across Pakistan and discuss them the purpose of the survey. They were also informed that data will only be obtained by employees, especially diagnosed with Tuberculosis and these employees perform their jobs six days in a week.
Procedure
In first time lag data of disclosure (TB) stigma affected individuals included, on second stage data on self-esteem as well as on perceived organizational support (POS) has been collected, at third time lag data was collected regarding deviant workplace behavior. The total number of questionnaire was 550. The same number of questionnaires was distributed in all three time intervals and the response rate was 321 only.
Instrumentation of the study
In order to investigate hypotheses of research study, primary data has been received from TB affected employees. To collect the data the suitable instrument used in this study was “questionnaire”. Authors used adopted as well as adapted questionnaire in English as well as translated in Urdu.
Following instruments used for data gathering.
Disclosure Tb stigmatized identities
Disclosure stigma has been measured by using the 12-items by (Van Rie et al., 2008). The scale used in the current study range from 1 (Very Unlikely) to 5 (Very likely) on five point of intervals. The value of Cronbach’s alpha= 0.7 and 0.8. Similarly, in this study the range adapt from Likert scale instead of original scale.
SE
The scale used for this variable developed by (Rosenberg, 1965) includes 10-items scale, also known as “Rosenberg Self-Esteem Scale”. Examples of items include the following: “I take a positive attitude toward myself,”.Alpha reliability of the scale was 0.72. Range of current scale is, 1. S.D to 5. S.A
Perceived organizational support
The scale of POS, 8-items scale has been measured by (Eisenberger et al., 1986). The alpha reliability of the scale was.93 and eight items includes: “The organization strongly considers my goals and values” and “The organization really cares about my well being”. Scale of this variable is, 1.Strongly disagrees to 5. Strongly agree.
Deviant work place behavior
The scale of deviant workplace behavior has been developed by (Bennett & Robinson, 2000), including 19-items.Sample items included the following: “Said something hurtful to someone at work”. “Made fun of someone at work” and alpha reliability for the scale was .78.
Findings
Examining the time lag data, research scholars prefer to conduct structural equation modeling. Likewise, in current study SEM has been used to check the correlation as well as regression analysis.
Confirmatory Factor Analysis (CFA)
In current research study, after exploratory factor analysis and before testing hypotheses, We carried out this factor analysis to test the factor structure. Current model consisted of four (4) latent variables; DTS, SE, POS, DWB. Authors analyzed CFA through statistical software in order to check the fitness of current model. In order to identify the fitness of model numerous measurements has been observed.
The present theoretical model consisted of four variables including one IV, one DV, one mediating variable and one moderating variable. There are different thresholds for all above measurements in table 4to check the fitness of model. The threshold value for RMSEA is, .050, IFI = .902, TLI = .89 and for CFI = .90. In order to achieve the excellent model fitness, researchers can modify the results through co variances of error terms (Hair, Ringle, & Sarstedt, 2011). After CFA the measurements of current model are as follows. The value of RMSEA is .039 which is less than 0.05 that point out a good fit of model, IFI value of current model is equal to 0.899 which demonstrates a good fit, TLI = 0.892 which also proves excellent fit, CFI = 0.898 again represents good fit of current theoretical model.
Descriptive Analyses
All theoretical variables i.e. disclosure TB stigma, self-esteem of employees, perceived organizational support, deviant workplace behaviors and their descriptive statistical results are presented in the given table. The table also includes the value of mean and standard deviation. The mean represent feedback of selected participants towards agrees and disagrees. Hence, the higher value of mean represent that respondents inclined towards agrees and vice versa.
The current study examined the descriptive statistics of all variables in the given table;
The above table represents the mean (M) and standard deviation (SD) of the current investigated variables. It indicates that higher value of means represents that participants’ move towards agreement side of the statement whereas the lower value of mean shows negative side of the variable by respective feedback of the selected participants.
The mean value of disclosure stigma (M=3.56, SD = 0.68), demonstrates that stigmatized individuals disclose their stigmatized identities in front of others and most of the participants agreeing with statements. Furthermore, self-esteem (M=3.47, SD = 0.71), that showed infected individuals reduce self-esteem at workplace. The mean value of perceived organizational support (Mean=3.92, SD = 0.57), demonstrates that respondents perceive supports from their organization. In addition, the value of deviant workplace behavior (M=3.34, SD = 0.70), shows that infected employees exhibit more deviant workplace behaviors.
Correlation Analyses
**p <.05, *p <.01, Disclosure TB stigma, SE= Self-esteem, POS= Perceived Organizational Support, DWB= Deviant workplace behavior.
The above table presented the correlation analyses.
The current research model also identified self-esteem is significantly and positively correlated with disclosure TB stigma (r=. 212, p < .05). The above table also presented that perceived organizational support was non-significantly correlated with disclosure tuberculosis stigma (r=.073, p > .05). Perceived organizational support and employees self-esteem positively and significantly correlated with each other (r=. 208, p <.05).
Additionally, deviant workplace behavior was non-significantly correlated with disclosure tuberculosis stigma (r=.098, p >. 01). Also, deviant workplace behavior was positively and significantly correlated with self-esteem (r=.224, p < .05) as well as with perceived organizational support (r=.132, p < .05).
Hypotheses Testing
Testing of Hypotheses
Test of Hypothesis 1
H1. Disclosure TB stigma is positively related with SE.
***=P <.001, β represent standardized regression coefficients, B= un-standardize regression coefficients, S.E= Standard Error
Author accepts and rejects the proposed hypothesis on the base of above mentioned values.
H1. Disclosure TB stigma is positively related with self-esteem.
According to the results of Table
Test of Hypothesis H2.
H2: Self-esteem mediates the relationship between disclosure tuberculosis stigmatized identities and deviant workplace behavior.
The result from above table revealed that direct effect of disclosure TB stigma on self-esteem is insignificant (β =.062, p>.05) but indirect effect is significant with value (β =.041, p< .01). Also the value of confidence interval lies between zero and revealed that there is partial mediation. Therefore, H2 is accepted.
Test of Hypothesis H3
H3. POS positively act as a moderator between self-esteem and deviant workplace behavior.
According to table
Conclusion
In current study the first objective is, to find out the relationship between disclosure TB induce stigma with positive self-esteem. To scrutinize the answer of the fourth research objective, to find out the relationship between disclosure TB induce stigma with positive self-esteem, hypothesis H1 was formulated. The result of study exposed that disclosure stigma is positively related with self-esteem and H1 is accepted. The result of current study also consistent with (Chaudoir & Fisher, 2010) that disclosure of stigma in front of non-stigmatized individuals may enhance their confidence level and they feel that their family and friends support them because of their infected disease. The disclosure of stigma increases the level of self-esteem. The previous research scholars demonstrated that people with stigmatized attributes generate positive and negative beliefs. People with disclosing stigmatizing belief has positive impact on their self-esteem (Quinn & Earnshaw, 2011).
Another study also found similar results that tuberculosis stigmatized people mostly hide or internalized their attributes with others to avoid rejection, but those find supportive environment, try to disclose their infectious nature that may enhance their esteem, worth, because they evaluate their selves positively (Heijnders & Van Der Meij, 2006). The finding of the current study also aligning with (Hanghøj & Boisen, 2014) that demonstrates the association between disclosure stigma and improvement of psychosocial health including anguish distress, better interpersonal relationships with each other and maintain their level of esteem.
The second objective of this study was to find out that self-esteem as a strong interlinking mechanism in the relationship between disclosures of TB induced stigma and deviant workplace behavior. Existing theory and research support this proposed hypothesis in Pakistani context. As per statistical results H2 is accepted.
The existing findings are similar with current statistical results. In like manner, research has shown positive stigmatized beliefs like disclosure reactions or disclosing the stigmatized identities in front of supportive ones will enhance individual’s self-esteem (Pachankis, 2007). Therefore, finding of previous literature aligned with current statistical results who suggested that the positive aspects of self-esteem, on the basis of their investigation, found that people with high esteem, mostly increase their social connections (Owens & McDavitt, 2006). At workplace, the disclosure reactions of stigmatized workforce positively link with high esteem. The high confidence due to disclosing their negative attributes with co-workers made them more confident and less engaged in deviance activities (Avey et al., 2011).
To determine that perceive organizational support act as a moderating variable between self-esteem and DWB of TB infected individuals. The third objective of the study formulated as well as H3 hypothesized which is rejected based on statistical results. The statistical result of present research model is inconsistent with previous literature. The possible explanation of obtained results may be stigmatized individuals with poor self-esteem not perceive any support from their organization. They hide their devalued identities at workplace and their managers and co-workers not know how about their actual identity and due to this their level of esteem become reduce and they maintain their negative relationship ship between self-esteem and deviant workplace behavior. Therefore, POS not act as a healthy moderator between self-esteem and deviant workplace behavior.
The statistical results of theoretical model support the current study and contribute in the existing literature of not only social science but also in psychology. The positive valance content that is disclosure of stigma due to TB positively relate with self-esteem. The current results exposed and align with existing theory and literature. Infected stigmatized individuals whenever feel supportive environment from others they disclose their disease or devalued stigmatized identities that increase their level of self-esteem (Ragins, 2008).
Limitations and Future Directions
The current research study comprehensively addressed that how disclosure tuberculosis stigmatized identities and its workplace outcomes through interlinking mechanism of self-esteem in public and private hospitals of Pakistan. Although, there are few limitations exist which are needed to be considered by future research scholars.
References
- Adhikari, B., Kaehler, N., Chapman, R. S., Raut, S., & Roche, P. (2014). Factors affecting perceived stigma in leprosy affected persons in western Nepal. PLoS Neglected Tropical Diseases, 8(6), e2940.
- Aryal, N., Regmi, P. R., & Mudwari, N. R. (2012). Violence against women living with HIV: a cross sectional study in Nepal. Global journal of health science, 4(3), 117.
- Austin, P. C., Lee, D. S., & Fine, J. P. (2016). Introduction to the analysis of survival data in the presence of competing risks. Circulation, 133(6), 601-609.
- Avey, J. B., Palanski, M. E., & Walumbwa, F. O. (2011). When leadership goes unnoticed: The moderating role of follower self-esteem on the relationship between ethical leadership and follower behavior. Journal of Business Ethics, 98(4), 573-582.
- Bashir, S., Nasir, M., Qayyum, S., & Bashir, A. (2012). Dimensionality of counterproductive work behaviors in public sector organizations of Pakistan. Public Organization Review, 12(4), 357-366.
- Battistelli, A., Galletta, M., Vandenberghe, C., & Odoardi, C. (2016). Perceived organisational support, organisational commitment and self‐competence among nurses: a study in two Italian hospitals. Journal of nursing management, 24(1), E44-E53.
- Baumeister, R. F. (2013). Self-esteem: The puzzle of low self-regard: Springer Science & Business Media.
- Bennett, R. J., & Robinson, S. L. (2000). Development of a measure of workplace deviance. Journal of Applied psychology, 85(3), 349.
- Bowles, H. R., & Gelfand, M. (2010). Status and the evaluation of workplace deviance. Psychological Science, 21(1), 49-54.
- Brohan, E., Slade, M., Clement, S., & Thornicroft, G. (2010). Experiences of mental illness stigma, prejudice and discrimination: a review of measures. BMC health services research, 10(1), 80.
- Chase, L. D., Teel, T. L., Thornton-Chase, M. R., & Manfredo, M. J. (2016). A comparison of quantitative and qualitative methods to measure wildlife value orientations among diverse audiences: A case study of Latinos in the American Southwest. Society & natural resources, 29(5), 572-587.
- Chaudoir, S. R., & Fisher, J. D. (2010). The disclosure processes model: understanding disclosure decision making and postdisclosure outcomes among people living with a concealable stigmatized identity. Psychological bulletin, 136(2), 236.
- Chirasha, V., & Mahapa, M. (2012). An analysis of the causes and impact of deviant behaviour in the workplace. The case of secretaries in state universities. Journal of Emerging Trends in Economics and Management Sciences, 3(5), 415.
- Corrigan, P. W., Faber, D., Rashid, F., & Leary, M. (1999). The construct validity of empowerment among consumers of mental health services. Schizophrenia research, 38(1), 77-84.
- Daftary, A., & Padayatchi, N. (2013). Integrating patients' perspectives into integrated tuberculosis-human immunodeficiency virus health care. The International Journal of Tuberculosis and Lung Disease, 17(4), 546-551.
- Dye, C. (2006). Global epidemiology of tuberculosis. The Lancet, 367(9514), 938-940.
- Eisenberger, R., Huntington, R., Hutchison, S., & Sowa, D. (1986). Perceived organizational support. Journal of Applied psychology, 71(3), 500.
- Ferris, D. L., Brown, D. J., Lian, H., & Keeping, L. M. (2009). When does self-esteem relate to deviant behavior? The role of contingencies of self-worth. Journal of Applied psychology, 94(5), 1345.
- Frenkel, S. J., & Yu, C. (2011). Managing coworker assistance through organizational identification. Human Performance, 24(5), 387-404.
- Gershon, T. D., Tschann, J. M., & Jemerin, J. M. (1999). Stigmatization, self-esteem, and coping among the adolescent children of lesbian mothers. Journal of Adolescent Health, 24(6), 437-445.
- Goffman, E. (1963). Stigma: Notes on a spoiled identity. Jenkins, JH & Carpenter.
- Hair, J. F., Ringle, C. M., & Sarstedt, M. (2011). PLS-SEM: Indeed a silver bullet. Journal of Marketing theory and Practice, 19(2), 139-152.
- Hanghøj, S., & Boisen, K. A. (2014). Self-reported barriers to medication adherence among chronically ill adolescents: a systematic review. Journal of adolescent health, 54(2), 121-138.
- Hayes-Larson, E., Hirsch-Moverman, Y., Saito, S., Frederix, K., Pitt, B., Maama, B. L., & Howard, A. A. (2017). Prevalence, patterns, and correlates of HIV disclosure among TB-HIV patients initiating antiretroviral therapy in Lesotho. AIDS care, 29(8), 978-984.
- Hogg, M. A., & Terry, D. I. (2000). Social identity and self-categorization processes in organizational contexts. Academy of management review, 25(1), 121-140.
- Hogg, M. A., & Turner, J. C. (1987). Intergroup behaviour, self‐stereotyping and the salience of social categories. British Journal of Social Psychology, 26(4), 325-340.
- Juniarti, N., & Evans, D. (2011). A qualitative review: the stigma of tuberculosis. Journal of Clinical Nursing, 20(13‐14), 1961-1970.
- Kurtessis, J. N., Eisenberger, R., Ford, M. T., Buffardi, L. C., Stewart, K. A., & Adis, C. S. (2017). Perceived organizational support: A meta-analytic evaluation of organizational support theory. Journal of Management, 43(6), 1854-1884.
- Li, N., Chiaburu, D. S., & Kirkman, B. L. (2017). Cross-level influences of empowering leadership on citizenship behavior: Organizational support climate as a double-edged sword. Journal of Management, 43(4), 1076-1102.
- Metofe, P. A. (2017). Antecedents of Deviant Work Behavior: A Review of Research. Acta Psychopathologica, 3(5).
- Moya, E. M., Biswas, A., Chavez Baray, S. M., Martínez, O., & Lomeli, B. (2014). Assessment of stigma associated with tuberculosis in Mexico. Public health action, 4(4), 226-232.
- Ngamvithayapong, J., Winkvist, A., & Diwan, V. (2000). High AIDS awareness may cause tuberculosis patient delay: results from an HIV epidemic area, Thailand. Aids, 14(10), 1413-1419.
- Noor, A., Bashir, S., & Earnshaw, V. A. (2016). Bullying, internalized hepatitis (Hepatitis C virus) stigma, and self-esteem: Does spirituality curtail the relationship in the workplace. Journal of health psychology, 21(9), 1860-1869.
- Omiya, T., Ito, M., & Yamazaki, Y. (2014). Disclosure of congenital cleft lip and palate to Japanese patients: reported patient experiences and relationship to self-esteem. BMC research notes, 7(1), 924.
- Organization, W. H. (2008). Global tuberculosis control: surveillance, planning, financing: WHO report 2008 (Vol. 393): World Health Organization.
- Organization, W. H. (2016). World malaria report 2015: World Health Organization.
- Owens, T. J., & McDavitt, A. R. (2006). The self-esteem motive: Positive and negative consequences for self and society. Self-esteem issues and answers: A sourcebook of current perspectives, 398-406.
- Pachankis, J. E. (2007). The psychological implications of concealing a stigma: a cognitive-affective-behavioral model. Psychological bulletin, 133(2), 328.
- Pérez-Garín, D., Molero, F., & Bos, A. E. (2017). The effect of personal and group discrimination on the subjective well-being of people with mental illness: the role of internalized stigma and collective action intention. Psychology, health & medicine, 22(4), 406-414.
- Quinn, D. M., & Chaudoir, S. R. (2009). Living with a concealable stigmatized identity: the impact of anticipated stigma, centrality, salience, and cultural stigma on psychological distress and health. Journal of personality and social psychology, 97(4), 634.
- Quinn, D. M., & Earnshaw, V. A. (2011). Understanding concealable stigmatized identities: The role of identity in psychological, physical, and behavioral outcomes. Social Issues and Policy Review, 5(1), 160-190.
- Quinn, D. M., & Earnshaw, V. A. (2013). Concealable stigmatized identities and psychological well‐being. Social and personality psychology compass, 7(1), 40-51.
- Ragins, B. R. (2008). Disclosure disconnects: Antecedents and consequences of disclosing invisible stigmas across life domains. Academy of Management Review, 33(1), 194-215.
- Rhoades, L., Eisenberger, R., & Armeli, S. (2001). Affective commitment to the organization: The contribution of perceived organizational support. Journal of Applied Psychology, 86(5), 825.
- Rosenberg, F. R., Rosenberg, M., & McCord, J. (1978). Self-esteem and delinquency. Journal of youth and adolescence, 7(3), 279-294.
- Rotundo, M., & Sackett, P. R. (2002). The relative importance of task, citizenship, and counterproductive performance to global ratings of job performance: A policy-capturing approach. Journal of Applied Psychology, 87(1), 66.
- Siegel, J., Yassi, A., Rau, A., Buxton, J. A., Wouters, E., Engelbrecht, M. C., . . . Nophale, L. E. (2015). Workplace interventions to reduce HIV and TB stigma among health care workers–Where do we go from here? Global public health, 10(8), 995-1007.
- Stuart, S. N., Chanson, J. S., Cox, N. A., Young, B. E., Rodrigues, A. S., Fischman, D. L., & Waller, R. W. (2004). Status and trends of amphibian declines and extinctions worldwide. Science, 306(5702), 1783-1786.
- Tajfel, H., & Turner, J. C. (1979). An integrative theory of intergroup conflict. The social psychology of intergroup relations, 33(47), 74.
- Törner, M., Pousette, A., Larsman, P., & Hemlin, S. (2017). Coping with paradoxical demands through an organizational climate of perceived organizational support: an empirical study among workers in construction and mining industry. The Journal of Applied Behavioral Science, 53(1), 117-141.
- Van Rie, A., Sengupta, S., Pungrassami, P., Balthip, Q., Choonuan, S., Kasetjaroen, Y., . . . Chongsuvivatwong, V. (2008). Measuring stigma associated with tuberculosis and HIV/AIDS in southern Thailand: exploratory and confirmatory factor analyses of two new scales. Tropical medicine & international health, 13(1), 21-30.
- Vardaman, J. M., Allen, D. G., Otondo, R. F., Hancock, J. I., Shore, L. M., & Rogers, B. L. (2016). Social comparisons and organizational support: Implications for commitment and retention. Human relations, 69(7), 1483-1505.
- Vatankhah, S., Javid, E., & Raoofi, A. (2017). Perceived organizational support as the mediator of the relationships between high-performance work practices and counter-productive work behavior: Evidence from airline industry. Journal of Air Transport Management, 59, 107-115.
- Wiersma, W., & Jurs, S. G. (2005). Research methods in education: An introduction.
- Yanos, P. T., Roe, D., Markus, K., & Lysaker, P. H. (2008). Pathways between internalized stigma and outcomes related to recovery in schizophrenia spectrum disorders. Psychiatric Services, 59(12), 1437-1442.
- Yasir, M. and A. Rasli. (2018). Direct and indirect effects of ethical leadership on workplace deviance in public healthcare sector of Pakistan. Journal of Advances in Management Research, 15(4), 558-574.
- Yildiz, B., & Yildiz, H. (2015). The effect of servant leadership on psychological ownership: The moderator role of perceived organizational support. Journal of Global Strategic Management| Volume, 9(2).
- Zolowere, D., Manda, K., Panulo, B., & Muula, A. (2008). Experiences of self-disclosure among tuberculosis patients in rural Southern Malawi. Rural & Remote Health, 8(4).
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
17 May 2019
Article Doi
eBook ISBN
978-1-80296-061-7
Publisher
Future Academy
Volume
62
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-539
Subjects
Business, innovation, sustainability, environment, green business, environmental issues
Cite this article as:
Sohail, U., Qureshi, M. I., Raza Naqvi, S., & Khan*, A. (2019). Disclosure Tuberculosis Stigmatized Identities And Its Workplace Implications In Pakistan. In M. Imran Qureshi (Ed.), Technology & Society: A Multidisciplinary Pathway for Sustainable Development, vol 62. European Proceedings of Social and Behavioural Sciences (pp. 109-124). Future Academy. https://doi.org/10.15405/epsbs.2019.05.02.10