
Effectiveness Of Neuro-Developmental Therapy In Children With Communication Disability


Abstract
The etiology of speech and language difficulties in children with communication disability is connected to many neuro-developmental differences in physiological stages and processes, which in case of neglecting could be a hidden source of ineffective educational as well as clinical treatment. Considering this fact, neuro-developmental therapy has been recommended as a very plausible method of treatment of especially preschool or early school age children. The main purpose of the research study is to evaluate the effectiveness of neuro-developmental therapy in children with communication disability from the perspective of the speech and language therapist, parents and teachers. The effects of the therapy will be evaluated in the areas of motor skills, attention, visual perception and communication. Methodology: A group of 30 children aged 4 to 8 years was subject to neuro-developmental therapy and the effect of a 30-week neuro-developmental therapy was partially analysed and discussed. Two selected cases are demonstrated with reference to their complex pre- and post-therapy evaluation. Results: The effects of the therapy were influenced by the physical and mental disposition of the children. The engagement of the parents plays a crucial role in the therapy. The effectiveness of the therapy and motivation of the family and the child is supported by communication and collaboration with a speech and language therapist. Conclusions: Some communication and perceptual-motor skills improved and some negative behaviours and pathological reflexes were inhibited.
Keywords: Case studycommunication disabilityneuro-developmental therapypreschool agespecial education
Introduction
The development of primary reflexes starts already in the intrauterine period and they are obvious right after birth. As the central nervous system gradually matures, their necessity decreases and they should be inhibited. Insufficient integration of some reflexes weakens the Broca’s and Wernicke’s areas responsible for phonemic hearing and articulation of sounds, as well as their integration through the subcortical region. From a speech-language pathology perspective, the most important reflexes are in the orofacial area (rooting, sucking, biting, chewing, swallowing, gag, and Babkin response).
Already in the prenatal period some risk factors might occur that weaken the inhibition of reflexes such as hyperemesis, high blood pressure, stress, diabetes. During the perinatal period a risk factor is a long or rapid birth, premature or late birth, caesarean section, induced birth, and breech presentation. A signal informing about a persistent primary reflex is an unsuitable and undesirable reaction of the nervous system, which affects further development, learning and behaviour. The basic symptoms of persistent primary reflexes include the following: beginning of verbal communication after 18 months of age, thumb sucking until 5 years of age or later, enuresis after 5 years of age, dyspraxia, coordination difficulties, impairment of visuomotor coordination, articulation difficulties, auditory and visual hypersensitivity and many others (Gogate & Hollich, 2016; González, Ciuffreda, Hernández, & Escalante, 2008; Konicarova & Bob, 2012; 2013a; 2013b; Melillo, 2016).
Problem Statement
The basic postnatal reflex is the Moro reflex. From a physiological perspective, it should disappear between the third and fourth month of age. It helps develop the breathing mechanism and eye movements. If this reflex persists, it may affect hyperactivity, auditory hypersensitivity, impulsive behaviour, anxiety, emotional and social immaturity, sensitivity to food, and increased adrenaline production leading to fatigue. It can also be related to allergy, asthma or chronic diseases (Konicarova & Bob, 2012; Volemanová, 2016). Right after birth children should be provided with the rooting and sucking reflex. The rooting reflex helps the child find a source of food in an active way and is activated by stimulation in the mouth region. In case of persistence, hypersensitivity around the lips and in the oral cavity occurs. Children have difficulties with transition to solid structured food. In children with persistent rooting reflex, hormonal changes were measured (abnormal function of the thyroid gland and overproduction of adrenaline). It affects articulation of the following sounds: [j], [l], [ɔː], [ʊ], [v], [tʃ], [ʃ], [ʒ] (Kondraciuk et al., 2014). The suction reflex allows protrusive movements of the tongue to suck in food. The suction process stimulates the development of vocalization and subsequent speech. If the reflex is not inhibited, the tongue remains in the frontal rest position accompanied with continuous pressure on the upper teeth, open occlusion, overbite). Speech is marked by articulation difficulties (interdental articulation), problems with swallowing and chewing, problems with coordination of speech or chewing with another activity. The process of concentrating is accompanied by inadequate tongue movements. Insufficient sucking reflex in the infant period and its persistence may lead to difficulties with tongue elevation, which may result in difficult articulation of sounds [l] and [r]. During the first months of life the oral cavity and the hand are connected by means of the Babkin response (also referred to as the palmomental or plantomental reflex), which persists until the fourth month of life of the child. It has a significant effect on the development of facial expression; its correct function is associated with the development of the asymmetrical tonic neck reflex. If the hand performs a movement (squeezing, grasping), the suction activity occurs. If this connection persists, hand movements affects movements in the orofacial area and vice versa (for example opening and closing the mouth when using scissors, biting others, difficulties with using cutlery, strong pencil grasp, tension of the facial muscles, association with the onset of the carpal tunnel syndrome). The development of drawing might be blocked by persistent palmar reflex. If not inhibited, problems occur with the pincer grasp and differentiating of individual finger movements. Preschool children avoid drawing and it is difficult for them to transform their thoughts into a graphical form. The ability to repeat words tends to remain intact, there is a problem however with articulation (transposition of sounds). A frequent feature is weakened posture and back pain while sitting at a table (Futagi, Yanagihara, Mogami, Ikeda, & Suzuki, 2013).
Neuro-developmental therapy is a concept that combines several methods focusing on sensory integration, special education, physiotherapy, visual screening and inhibition of primary reflexes. The therapy can be started at the age of four years, but a positive effect is also observed in adults. The therapy includes simple exercises aimed at imitating the movement induced by primary reflexes, which activates higher brain centres (Mayston, 2016). The exercises need to be repeated and performed slowly with maximum concentration. For the purposes of teachers, special education teachers, psychologists, speech-language therapists, occupational therapists and other professionals, a school-based neuro-developmental stimulation programme was designed and is suitable for whole classes. The exercises are based on the movement models of a 2 to 9-month-old child, which form the basis of other deliberate movements. The first exercise focuses on the development of balance, the following two exercises on the inhibition of primary reflexes in order to improve sensory integration; gradually other skills are added. It is necessary to perform the exercises every day for about 5 to 10 minutes for a period of 9 to 12 months. The exercises are linked together and the order must not be changed (Volemanová, 2016).
Research Questions
The objective of the research study is to assess the effectiveness of neuro-developmental therapy (NDT) in children with communication disability from the perspective of a speech-language therapist, parents and teachers of the child. A possible effect of NDT exercises will be monitored in the area of motor skills, attention, visual perception and communication. The following research question was formulated in line with the objective: What is the effectiveness of neuro-developmental therapy in selected children with communication disability from the perspective of speech and language therapist, parents and teachers of the child?
Purpose of the Study
The purpose of the research study is to obtain a complete body of data of at least 10 children with communication disability aged 4 to 8 years. Each child will undergo an initial diagnosis – assessment of persistent primary reflexes, and examined for postural reflexes. The assessment will also include the level of graphomotor skills, oromotor skills, and visual perception. The initial examination will also include a parent and teacher questionnaire in order to ensure a comprehensive picture of the child. All children will be trained in neuro-developmental stimulation from the first week, irrespective of the nature of persistent reflexes. The children’s parents will be advised on the requirement to perform the exercises on a daily basis. The exercises should be performed for a period of 30 weeks (corresponds with the number of lessons). After completion of the last lesson a final examination will be performed by using the same set of tests again including parent and teacher questionnaires. The measured data will then be analysed.
Research Methods
The assessment of persistent primary reflexes will be performed by means of the following diagnostic tests: Proprioception and balance test: one leg stand, heel-toe walk; Asymmetrical tonic neck reflex test (ATNR) in the tabletop position; Tonic labyrinth reflex test (TLR) in the standing position; Landau test; Symmetrical tonic neck reflex test (STNR) in the tabletop position; Galant reflex test; Ocular postural head reflex test; Labyrinth postural head reflex test; Moro reflex test – standard test for vestibular activation of the Moro reflex; Palmar reflex test ;Sucking reflex test.
The following two tests will be used for the evaluation of postural reflexes: amphibian reflex test and segmental rotation test. Each test item is scored on a scale of 0-4 points (0= no symptoms, 4= strong symptoms, apparent signs of discomfort and stress).
The level of graphomotor skills will be evaluated by means of the tracing test; the quality of oral movements will be examined by a modified version of the test of isolated oral movements by LaPointe and Wertz. To achieve a comprehensive perspective, a parent and teacher questionnaire will be used.
So far, a total of 45 children have been trained but only 30 continue exercise. In 15 cases, the procedure was terminated by the therapist because home exercise had not been performed on a regular basis. Many parents did exercise with their children only twice a week, which is insufficient for an adequate result.
Regarding the fact that most of the children are in the second third of the lessons, the authors of the present study decided to publish the data of only two children who had completed the whole procedure and where the initial and final diagnosis can be compared. Therefore, the research sample comprised one girl and one boy.
Findings
The initial diagnosis of these three respondents was performed during the first week of October 2017. After that their parents were instructed about the method and frequency of home exercises and were trained during the first lesson. Regular home exercise was performed for a period of 7 months; the final diagnosis was conducted at the beginning of May.
Case 1
The initial examination in Case 1 confirmed strongly persistent Moro reflex, which has a negative effect on coping with difficult situations, stress regulation, and energy management. In case of excessive exhaustion the girl reacts with fits of crying or aggression. The girl is incapable of energy management, is unable to relax, in case of exhaustion it is impossible for her to calm down or relax, she is unable to fall asleep. The only thing that helps the girl is when her mother inserts her breast into her mouth to imitate suction (the girl has not been breastfed since two years of age). The other persistent reflex is the sucking reflex. The girl always needs to have something in the oral cavity (pencil, fingers, chewing a T-shirt, etc.) Other apparent reflexes include the asymmetrical tonic neck reflex and amphibian reflex, which is very weak. Some mild symptoms were observed in the palmar reflex, ocular postural head reflex, tonic labyrinth reflex, and problems with proprioception and balance.
During the tracing activity the girl managed to imitate all shapes corresponding to her age. She had a tripod grasp of the writing utensil with a small angle. The pressure against the surface was very strong. The lines were strong and pressed in the surface. Tracing was very slow and performed with a considerable effort. While concentrating the girl showed overall body tension and involvement of the tongue, which was outside the oral cavity pressed between the lips.
The modified test of isolated oral movements revealed that the girl was able to imitate all movements at a very slow pace and with a considerable effort. Tongue elevation and depression was accompanied by neck muscle spasms, tendency to tilt the head back and engage muscle mentalis. Retaining her tongue behind the lower teeth was accompanied by wave motion of the whole tongue, folding, with a duration of only 2-3 seconds. The girl said that it was very difficult. Lip protrusion automatically activated the tongue, which started to move forward. The rest position of the tongue was interdental.
The girl expressed herself mainly in simple sentences and was very restrained in a conversation. She answered questions, respected the changing of roles of communication partners, but did not develop conversation herself. She understood basic data and rarely established visual contact. She had difficulties with right-left orientation and spatial orientation both on the surface and on the body image. Time orientation corresponded with the girl’s age. No particular problems were observed in the morphological-syntactical language aspect. The sentence structure was consolidated and no agrammatical structures were observed. The girl’s vocabulary corresponded with the age group, word recalling was slower. The girl used all word classes. She had difficulties with producing synonyms and homonyms, the production of antonyms was trouble free. The girl suffered from weakened short-term verbal-acoustic memory; her phonemic hearing was normal.
Her behaviour as noted in the parent questionnaire is mentioned above. Unfortunately, no information was provided by the class teacher. The teacher thought there were no problems in the educational process and refused to complete the questionnaire. The girl’s mother was very motivated for the exercise, was very concerned about her daughter’s behaviour and wanted to help. She started regular exercise with the girl, but already during the first week of exercise she observed significant negative changes in behaviour, the girl was extremely weepy, back-talking, did not respect authority and became aggressive. The girl’s mother was unable to overcome these problems and quit regular exercise. During the next visit the mother was explained that irregular exercise supports these manifestations. After that they resumed regular exercise 4 hours before bed time every day. After three days the negative manifestations gradually subsided and almost disappeared before the next visit. During the first six weeks of exercise these manifestations were present. From the seventh lesson, an improvement was observed without any negative manifestations. After six weeks of exercise, interdental articulation disappeared completely and the rest position of the tongue was corrected. However, the girl’s need to have something in the oral cavity increased; this was accompanied by increased salivation. After another three weeks of exercise, increased stimulation of the oral cavity was eliminated.
During the final diagnosis, improvement was observed in all areas. Some symptoms were observed only in the asymmetrical tonic neck reflex (Figure
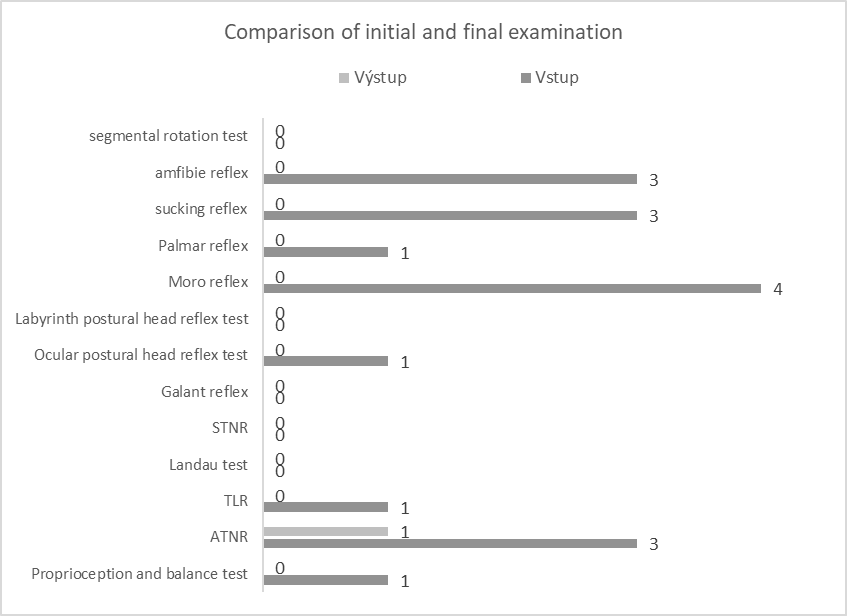
In the tracing test the pressure on the surface improved. Copying of shapes became smoother, faster and the lines were not pressed in the surface. The girl’s oromotor movements were imitated without engagement of the articulation organs and neck muscles. The tongue was relaxed, the girl was able to hold the tongue behind the lower teeth without wavy movements. The rest position of the tongue improved spontaneously. In the area of communication an improvement was observed, the girl engaged in and developed conversation spontaneously. When she was assigned a task, she asked additional questions and was interested in details. She expressed herself in complex clauses and sentences. Word recalling improved, the girl used synonyms and homonyms in a skilful way. Her short-term verbal-acoustic memory improved.
The information provided by the girl’s mother confirms improvement in behaviour. The girl sleeps calmly, learned to relax, and is capable of better energy management. In case of negative emotions she no longer searched for her mother’s breast. According to her mother, the girl is generally more cheerful and is interested in learning about new things.
Case 2
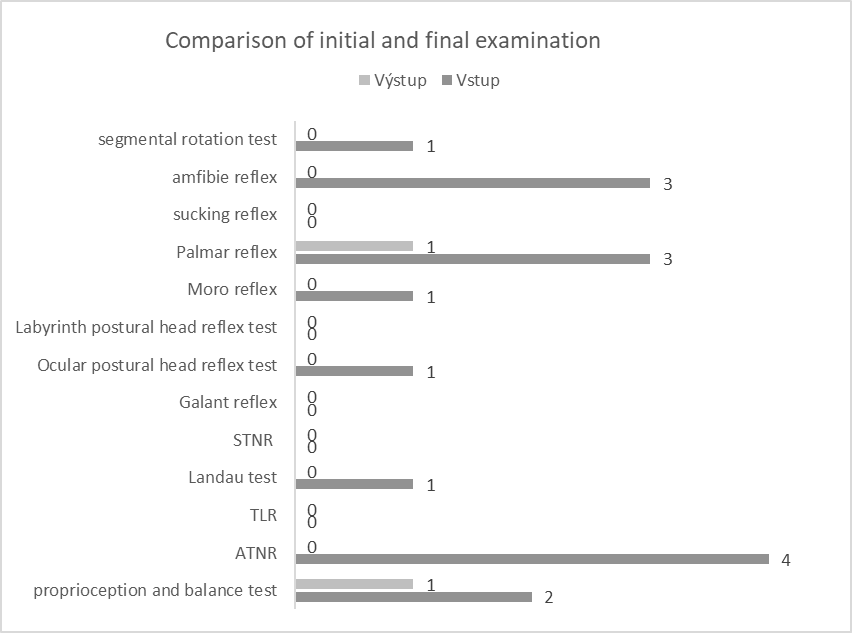
Prior to the initial diagnosis and inclusion in the research sample, the boy’s articulation improved and corresponded with relevant standards. During the initial diagnosis the boy showed manifestations of persistent primary reflexes in the asymmetrical tonic neck reflex (Graph 3). These manifestations were assessed as grade 4. Apparent problems were also observed in connection with persistent palmar reflex and weak manifestations of the amphibian reflex. Both reflexes were assessed as grade 3. Some symptoms were observed in segmental rotation, Moro reflex, ocular postural head reflex, and Landau reflex. The area of proprioception and balance was assessed as grade 2.
Considerable difficulties were observed in the tracing test. It was difficult for the boy to copy geometrical shapes. The grasp of the writing utensil was either very convulsive or too light. The pressure against the surface was also either too strong or too weak. The lines were shaky or too strong. At first the boy needed to examine the picture, then he drew a part of it, examined the picture again and continued drawing. The boy needed more time to complete the task, was nervous and restless, and had a tendency to divert from the topic and speak about something else or do another activity. In the modified test of isolated oral movements, the boy did not show any deficiencies. In a conversation the boy preferred his own topics, in case of topics beyond the boy’s interest he had a tendency to divert the conversation and talk about something of his interest. The boy expressed himself in simple sentences with loose sentence structures. He understood basic data and established visual contact for a short time. He had difficulties with spatial orientation both on the surface and on the body image, time orientation was not consolidated. His use of the language corresponded with applicable standards; there were some agrammatical structures in spontaneous speech in the context of declension of less frequent words. The boy’s vocabulary corresponded with the age group, word recalling was slower. In speech the boy uses all word classes, is able to produce synonyms and antonyms, he has difficulties with producing homonyms. The boy suffered from weakened short-term verbal-acoustic memory; his phonemic hearing was normal.
The parent questionnaire was completed by the mother, according to whom the main problems were in the area of the boy’s attention. He is often distracted, does not react to instructions and is immersed in his own activities. When they are in public, the mother is worried about the boy entering personal zones of other people, touching surrounding objects, etc. When they are indoor, the boy often hits doors, furniture and people. The boy refuses to draw and complete any graphomotor oriented tasks.
According to the class teacher, the boy is often distracted or immersed in an activity, often does not react to his classmates or the teacher. He becomes attached to his activities and needs to have them finished. The teacher often observes nervousness, restlessness and non-observance of personal zones. In terms of learning the trivium, the boy is an average learner and requires sufficient time and regular repetition.
After the initial diagnosis the boy was trained in neuro-developmental therapy during the first week and the boy’s mother was instructed about the necessity of regular home exercise. The mother was sufficiently motivated for the exercise. During the first weeks of exercise, no change in behaviour was observed. No compensations were observed during the exercise, only when performing balance activities the boy was rash, counted too quickly and did not want to obey adults. It was too difficult for him to perform exercises with his eyes shut, he tried to open his eyes a little. The first changes in behaviour were observed by both the mother and the teacher after lesson 18, when the boy started to be more concentrated, stopped preferring his own activities and their completion, and started communicating with his classmates. The boy hit furniture less frequently and kept greater distance from other people. According to the teacher, his reading and especially independent writing improved. The boy’s handwriting was of identical size, regular shape and precise lines.
After completion of the final examination, improvement was observed in all monitored areas. Slight difficulties still remain in the area of balance without looking. The boy tries to avoid these activities and tends to open his eyes a little to have some visual control. In case of increased pressure and stress, slight manifestations of the palmar reflex occur. The remaining reflexes were inhibited (Figure
The tracing test was performed by the boy without significant difficulties. Pressure against the surface was normalized, the boy used a tripod grasp without convulsion. Copying of geometric shapes was smooth without stopping. The boy managed to coordinate the eye and the hand. In the modified test of isolated oral movements, no significant difficulties were observed just as in the initial examination. During conversation the boy is now much more responsive and is able to talk about more topics. Word recalling is normalized, sentence structure is consolidated, there are no agrammatical structures in the boy’s speech. The boy establishes eye contact more often. Spatial orientation is consolidated both on the surface and on the body image, time orientation and short-term verbal-acoustic memory improved.
According to the mother, the boy’s attention improved, he stopped hitting objects around him and is no longer tempted to touch everything around him. He improved in respecting personal zones and his overall approach to reading and especially independent writing and drawing improved. Drawing is still not among his favourite activities but is no longer negated. This was also confirmed by the class teacher, who also suggested improvement in social relationships between the boy and his classmates.
Conclusion
During the first four weeks of exercise, the children’s sickness rate increased, which prevented their regular engagement and some exercises were delayed by two to three weeks. Around the fifth lesson the sickness rate decreased (possibly due to inhibition of primary reflexes, this may also be coincidental). Compensations occurred mainly during the first two weeks in the prone position, but gradually disappeared in most children. In the first week some children showed negative changes in behaviour (weepiness, fits of aggression, infantilism, back talking, disrespecting authority, etc.) Mothers often interrupt regular exercise or stop completely (irregularity multiplies negative symptoms because the reflexes are stimulated on an irregular basis and their inhibition is slower). After consultation they carry on exercise on a regular basis and negative behaviour usually decreases after two or three days and disappears at the end of the week. Only one child was diagnosed with the Spinal Galant reflex (according to the paediatrician, persistent diurnal enuresis is normal in a girl aged 5 years and 10 months, no specialized treatment is provided, this causes major complications and social stigmatization in kindergarten).
In both clients, improvement was observed in all monitored areas. At the end of neuro-developmental therapy, almost no manifestations of persistent primary reflexes were observed. Regular exercise resulted in inhibition of these reflexes and activation of postural reflexes. Both clients improved in concentration, perception of their own body image, and self-knowledge. They also improved in the area of communication, motor skills, graphomotor skills, and visuomotor coordination. All partial functions required for the adoption of academic skills were consolidated. In terms of family relationships, the relationship between the child and the mother improved. At the end of the therapy the mothers were more relaxed, they were no longer worried about the performance and behaviour of their children. They gained confidence in themselves as mothers who can help their children.
The limitations of the study include both parents and teachers, who may have a tendency to underestimate or overestimate children’s performance. Parents fail to perform exercises on a daily basis and do so only a few times a week or they do not remember how to perform exercises properly, or they do not notice compensations used by their children. The exercises must be supervised by a parent or a different qualified person to ensure proper execution. Children must not do the exercises by themselves although they remember how to do them. The results of the initial or final evaluation might be distorted by the current mood of the client, fatigue, health status, etc. Termination of exercises might results from non-achievement of the desired results, reluctance, or long-term pressure on the part of the parent or child.
The data obtained represent a basis for longitudinal studies, which the authors of the present study intend to perform. The results of individual children will be compared and the effectiveness of neuro-developmental therapy will be assessed. NDT provides an opportunity to help children improve their skills required for academic achievement and improved quality of life.
References
- Futagi, Y., Yanagihara, K., Mogami, Y., Ikeda, T., & Suzuki, Y. (2013). Review Article: The Babkin Reflex in Infants: Clinical Significance and Neural Mechanism. Pediatric Neurology, 49, 149-155. DOI:
- Gogate, L., & Hollich, G. (2016). Early Verb-Action and Noun-Object Mapping Across Sensory Modalities: A Neuro-Developmental View. Developmental Neuropsychology, 41(5-8), 293-307. doi:
- González, S. R., Ciuffreda, K. J., Hernández, L. C., & Escalante, J. B. (2008). The Correlation between Primitive Reflexes and Saccadic Eye Movements in 5th Grade Children with Teacher-Reported Reading Problems. Optometry & Vision Development, 39(3), 140-145.
- Kondraciuk, A., Manias, S., Misiuk, E., Kraszewska, A., Kosztyła-Hojna, B., Szczepański, M., & Cybulski, M. (2014). Impact of the orofacial area reflexes on infant's speech development. Progress in Health Sciences, 4(1), 188-194.
- Konicarova, J & Bob, P. (2013b) Asymmetric tonic neck reflex and symptoms of attention deficit and hyperactivity disorder in children. International Journal of Neuroscience [serial online], 123(11), 766-769. Available from: Academic Search Ultimate, Ipswich, MA. Accessed May 31, 2018
- Konicarova, J., & Bob, P. (2012) Persisting primitive reflexes in medication-naïve girls with attention-deficit and hyperactivity disorder. Neuropsychiatric Disease & Treatment [serial online], 9, 1457. Available from: Complementary Index, Ipswich, MA. Accessed May 31, 2018. doi:
- Konicarova, J., & Bob, P. (2013a) ADHD in children, balancing deficits and primitive reflexes. Biological Psychiatry [serial online], 73(9), 98-99. Available from: Science Citation Index, Ipswich, MA. Accessed May 31, 2018.
- Mayston, M. (2016). Bobath and Neurodevelopmental therapy: What is the future? Developmental Medicine & Child Neurology, 58(10), 994. doi:10.1111/dmcn.13221
- Melillo, R. (2016) Persistent primitive reflexes and childhood neurobehavioral disorders. Neuroplasticity in learning and rehabilitation. Hauppauge, NY, US: Nova Biomedical Books. Available from: PsycINFO, Ipswich, MA. Accessed May 31, 2018.
- Volemanová, M. (2016) Pohybem se učíme. Praha: INVTS.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
09 April 2019
Article Doi
eBook ISBN
978-1-80296-059-4
Publisher
Future Academy
Volume
60
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-1062
Subjects
Multicultural education, education, personal health, public health, social discrimination,social inequality
Cite this article as:
Tabachová, J., & Vitásková, K. (2019). Effectiveness Of Neuro-Developmental Therapy In Children With Communication Disability. In E. Soriano, C. Sleeter, M. Antonia Casanova, R. M. Zapata, & V. C. Cala (Eds.), The Value of Education and Health for a Global, Transcultural World, vol 60. European Proceedings of Social and Behavioural Sciences (pp. 538-548). Future Academy. https://doi.org/10.15405/epsbs.2019.04.02.68