
Kinetic Rehabilitation For Adults With Gonarthrosis

Abstract
The main goal of this study is to investigate the beneficial effects of the rehabilitation through medical gymnastics for adults with gonarthrosis. Research methods: pedagogical observation, investigation, tests for muscular and articular assessment, statistical-mathematical method and graphical representation of the data. The study was conducted in the specialised gym of the “Sf. Luca” Chronic Disease Hospital of Bucharest, from December 2016 to May 2017, with a group of 10 male and female subjects of 49-67 years old, hospitalised for the treatment of gonarthrosis. Control tests used: height (cm), weight (kg), glycaemia (g/l), blood pressure (mmHg), muscular strength and mobility of knee joint. Medical gymnastics, including exercises of warm-up, mobility and coordination, balance, posture, breathing and non-competitive sport elements, was used for kinetic rehabilitation. The study results confirm the improvement of the condition of patients submitted to an early rehabilitation plan, phased and individualised depending on their diagnosis and particularities, focusing on the morphofunctional and mental aspects. The rehabilitation treatment must be continued at home, workplace or in special spaces, under the supervision of the kinesiotherapist, in order to prevent the possible relapses of the disease and to maintain and improve the functional progress reached during the sessions made in the hospital.
Keywords: Gonarthrosisassessmentmedical gymnasticsrehabilitationadults
Introduction
Gonarthrosis is the most common articular disease of the knee. It is also called “the disease that immobilises the knee”, because of the pain felt in the joint, the walking with a limp and the obvious swelling of the knee. Its frequency is due to the genetic heritage, life-long excessive strain of the joint, injuries or rheumatism of the affected joint or neighbouring joints (Slăvilă, 2016a).
Gonarthrosis does not affect young people, but people over 40 years old. In the last years, there are an increasing number of persons who seek the help of the doctor, taking into consideration that the elderly are more and more active and prefer efficient treatments instead of classical and conservative ones (Sbenghe, 1981).
Kinesiotherapy is included in the means of medical rehabilitation of motor disabilities. This is a therapeutic method largely used in the phase immediately after the injury and continued with the phase of spontaneous recovery; it is a valuable auxiliary before and after surgery in the phase of sequelae (Stroescu, 1979; Sbenghe, 1987; Crețu, 2003).
Medical gymnastics is mainly intended to initiate and improve the remaining motricity or the rehabilitation during the complex process of physical, mental, professional and social readaptation of the individual; it has a very important role in the rehabilitation of motor disabilities during all evolutionary stages of the disease (Nicolescu, 2010; Potop, 2014).
Problem Statement
From a mechanical point of view, the knee, also called the “intermediate joint of the lower limb”, has a great ability in the full extension, and thus it can support the large pressure exerted by the human body. The knee also has high mobility and, starting from a certain degree of flexion, ensures the optimum orientation and movement of the leg related to the unevenness of the ground. The skeleton of the knee includes the lower end of the femur bone, the upper extremities of the tibia and fibula and also the knee cap/patella – a specific bone of this zone (Baciu, 1977; Gavrilescu, 2010).
Knee joint is the largest mobile segment that links the thigh to the shank and has numerous implications in pathology. Some authors consider it a condylar joint or a trochlea joint, which has only one level of movement freedom and allows the flexion and extension, ensuring the anterior and posterior movement of the lower limb (Potop, 2011; Timnea & Baican, 2017).
Gonarthrosis or arthrosis is one of the oldest diseases worldwide; it is characteristic of the vertebrates and can affect them everywhere. It is responsible for the alteration of life quality in all its aspects, because it generates pains and mobility limitation (Constantin, 1997; Slăvilă, 2016b).
Arthrosis is defined as a chronic, degenerative, painful and deforming articular disease anatomically characterised by initial destructive alterations of the articular cartilage, formation of osteophytes and eventual synovial inflammatory responses. The disease consists of degeneration, a kind of aging of the articular system. The cartilaginous surfaces, bone masses, ligaments and synovia are more or less damaged and fulfil their task insufficiently.
Gonarthrosis can be divided into two forms
All articular deformations will cause arthrosis, regardless of their origin. Also, the less severe injury can generate arthrosis. A simple sprain poorly treated can maintain a swelling of a cartilaginous zone, which will facilitate degeneration of the peripheral tissues.
Gonarthrosis is diagnosed by an orthopaedist following up a clinical examination focused on the painful knee. The mobility, oedema, sensibility and walking shall be checked up. The X-rays will prove the “grinding” of the articular cartilage (diminution of the articular space height) and the appearance of the osteophytes (bone spurs).
The treatment of gonarthrosis involves: the necessary measures taken for reducing the articular stress; avoidance of the aggressive sports and overstress; control of body weight; balneophysiotherapy and kinesiotherapy; administration of painkillers, corticosteroids and sterile viscoelastic solutions administered into knee joint (Slăvilă, 2016a).
Research Questions
In order to conduct our research, we have proposed the following questions:
Does the synthesis of the information taken from specialised literature and personal experience improve the methods of kinetic intervention on the patients with gonarthrosis?
Is the rehabilitation program established depending on other diseases or objectives of the patients?
Is the beneficial role of kinesiotherapy proven (pain relief, recovery of knee articular stability and mobility)?
Are the patients influenced positively during the programs of kinesiotherapy?
Does the kinesiotherapy relieve the articular pains and increase the mobility of knee joint?
Purpose of the Study
The main goal of this study is to investigate the beneficial effects of the rehabilitation through medical gymnastics for adults with gonarthrosis.
Research Methods
Research methods
Findings
Gonarthrosis is most frequently defined as the change involving damage of the articular cartilage of the knee joint, emergence of abnormal knee tissue, reactive changes in synovial membrane and pathological synovial fluid. The review of thee specialised literature on gonarthrosis reveals: the existence of several studies supporting the systemic therapy of the arthrosis by means of the sterile viscoelastic solutions (Stănescu, 2009); the efficacy of individual physical therapy during the medical treatment for gonarthrosis in the working population engaged in physical labour; comparison between the state of pain and mobility before and after the treatment (Kasumovic et al., 2013); rehabilitation of knee mobility using hydrokinesiotherapy in patients with gonarthrosis (Burcea, Georgescu, Armean, & Burlibașa, 2014); main causes of the gonarthrosis and of other forms of arthrosis; when and how they can be treated; conservative treatment and knee arthroplasty (Stănescu, 2018); the impact of dynamic platform exercises on knee joint muscle strength in patients with gonarthrosis treated with microfracture method (Klupiński, Krochmalski, & Woldańska-Okońska, 2017) etc.
This study monitored a group of 10 male and female subjects from the urban environment, with different professions, aged from 49 to 67 years, hospitalised for the treatment of gonarthrosis.
Table
The values of glycaemia in the whole group of subjects have a mean of 43.0 mg/dl, with a mean error of 8.17 and a poor homogeneity (25.84%). The blood sugar values of the patients under study indicate a stage of latent diabetes (Figure
Given the age of the subjects of this study, the values of blood pressure and glycaemia are clinically significant for each individual who participated in the research. The study has revealed that blood pressure values, along with glycaemia values, have a decisive influence on the kinesiotherapy program and the progress made by each patient from one session to another. Therefore, besides the specific kinesiotherapy treatment, the patients received a proper medication during their hospitalisation, which contributed to their successful rehabilitation.
Table
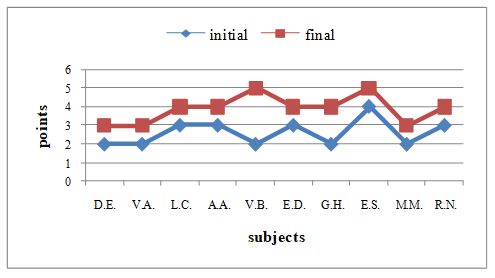
The analysis of the results of muscle strength development in the quadriceps for the studied subjects, as shown in Table
Figure
The kinesiotherapeutic programs personalised for each patient participating in this study were based on the physical, mental, professional and social rehabilitation of the individual as soon as possible. These programs have an active contribution, even after the sessions made with the specialised staff of the hospital, to the rehabilitation of the motor disability caused by gonarthrosis, regardless of the disease stage before rehabilitation.
The rehabilitation program focused on the function or segments of the injured limb and took into account the progressive complexity of exercises performed under the supervision of the kinesiotherapist, meant to ensure gestures or movements with direct finality, depending on the specifics of the disease, age, physical capacity, medical history record etc.
The beneficial effects of kinesiotherapy recorded during our research on gonarthrosis are explained by highly efficient rehabilitation means and methods selected and adapted to each and every patient. The created commands and programs were clearly transmitted and easy for everyone to understand.
Conclusion
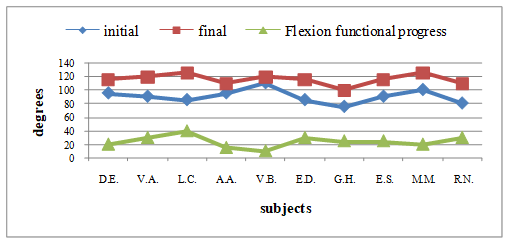
This research has proven that the progress in the development of knee motricity and mobility is directly proportional to the improvement of patient’s physical possibilities and confirms the efficiency of the gonarthrosis rehabilitation program used in the case of the group under study.
The functional progress of the affected joint is due to the correlation between the kinesiotherapeutic program of rehabilitation after gonarthrosis and the real possibilities of the patient. This correlation shortens the reintegration of patients into socio-professional life by fighting efficiently against the main symptoms of gonarthrosis.
Our study certifies the improvement of patients’ condition following the implementation of an early rehabilitation plan, sequenced and individualised according to the diagnosis and particularities of the patient, focusing on their morphofunctional and mental particularities.
The rehabilitation treatment must be carried on at home, workplace or in special facilities, under the supervision of the kinesiotherapist, in order to prevent the possible relapses of the disease and to maintain and improve, as the case may be, the functional progress reached during the sessions performed in the hospital.
Acknowledgments
This paper is part of the research plan for 2017-2018 of the Faculty of Physical Education and Sport of the Ecological University of Bucharest. In charge with the project: Professor Vladimir Potop, PhD. The authors of this paper express their gratitude to the senior professor CFM, Doctor Mircea Slăvilă, department head in “St. Luca” Chronic Disease Hospital of Bucharest, for his collaboration and support for carrying out this study.
References
- Baciu, C. (1977). Anatomia funcțională și biomecanica aparatului locomotor. București: Sport-Turism.
- Burcea, C. C., Georgescu, L., Armean, P., & Burlibașa, M. (2014). Rehabilitation of knee mobility using hydrokinesitherapy in patients with gonarthrosis. Sport Medicine Journal, 3(39), 2406-2410.
- Centers for Disease Control and Prevention. (2010). Normal joint range of motion study. Retrieved from https://www.cdc.gov/ncbddd/jointrom/
- Constantin, B. (1997). Geriatrie. București: Editura Medicală.
- Crețu, A. (2003). Ghid clinic și terapeutic fizical-kinetic în bolile reumatice. București: Bren.
- Gavrilescu, D. (2010). Anatomia funcțională și biomecanica. București: Editura Didactică și Pedagogică, R.A.
- Kasumovic, M., Gorcevic, E., Gorcevic, S., & Osmanovic, J. (2013). Efficacy of physical therapy in the treatment of gonarthrosis in physically burdened working men. Materia Socio Medica, 25(3), 203-205.
- Klupiński, K., Krochmalski, J., & Woldańska-Okońska, M. (2017). The impact of dynamic platform exercises on knee joint muscle strength in patients with gonarthrosis treated with microfracture method. Polski Merkuriusz Lekarski, 42(252), 247-251.
- Nicolescu, M. (2010). Tratamentul ortopedico-chirurgical în afecțiunile aparatului locomotor. București: All.
- Potop, V. (2011). Kinesiology techniques in knee traumatology by means of fitness. International Scientific Session “Applications of Kinetotherapy and Sports Medicine in Motor Activities”, Bucharest: Bren (pp. 49-54).
- Potop, V. (2014). Gimnastica de bază. București: Discobolul.
- Timnea, O. C., & Baican, M. S. (2017). Anatomie și biomecanică. București: Discobolul.
- Sbenghe, T. (1987). Kinetologie profilactică, terapeutică și de recuperare. București: Editura Medicală.
- Sbenghe, T. (1981). Recuperarea medicală a sechelelor post-traumatice ale membrelor. București: Editura Medicală.
- Slăvilă, M. (2016a). Recuperare kinetoterapeutică în reumatologie. București: Printech.
- Slăvilă, M. (2016b). Recuperare kinetoterapeutică în geriatrie și gerontologie. București: Printech.
- Stănescu, M. (2009). Boala artrozică, ținta consolidării terapiei sistemice cu ajutorul soluțiilor sterile vascoelastice. Retrieved from http://www.getmd.com
- Stănescu, M. (2018). Gonartroza. Retrieved from https://m.facebook.com/story.php?story_fbid=2190594664291749&id=842215452463017)
- Stroescu, I. (1979). Recuperarea funcțională în practica reumatologică. București: Editura Medicală.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
16 February 2019
Article Doi
eBook ISBN
978-1-80296-054-9
Publisher
Future Academy
Volume
55
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-752
Subjects
Sports, sport science, physical education
Cite this article as:
Timnea, O. C., Stănescu, A. M., Potop, L., & Timnea, A. C. (2019). Kinetic Rehabilitation For Adults With Gonarthrosis. In V. Grigore, M. Stănescu, M. Stoicescu, & L. Popescu (Eds.), Education and Sports Science in the 21st Century, vol 55. European Proceedings of Social and Behavioural Sciences (pp. 369-376). Future Academy. https://doi.org/10.15405/epsbs.2019.02.46