
Using Complementary Kinetic Means For Gymnasts With Spinal Imbalances And Lumbar Pain

Abstract
The growing interest in sports activities, both recreational and high-performance ones, has caused, in recent decades, a considerable increase in the pathologies of the musculoskeletal system. Among them, lumbar pain is the most common musculoskeletal disorder in athletes, its rate ranging between 3.3 and 4.6% of overexertion injuries related to sports activity. In performance gymnastics, the interruption of sports activity, especially for medical reasons (lumbar pain), has a negative impact on the performance capacity, and therefore we should develop a complex recovery programme that allows the athletes to return as quickly as possible to their specific activity and also to maintain an optimal state of health. Sports medicine increasingly requires the use of complementary kinetic means in the prophylaxis and recovery of various spinal imbalances, as well as in order to enhance sports performance. This study aims to objectify, through pain assessment questionnaires, the effectiveness of a complex recovery programme using complementary kinetic means (Shiatsu, Yumeiho, reflexology) on a group of 5 female athletes practicing performance aerobic gymnastics, who show spinal imbalances and suffer from lumbar pain. In conclusion, we can state that, from our observations and the pain assessment questionnaires completed by the female gymnasts before and after 9 months of participation in the complex recovery programme, a decrease in the pain sensitivity threshold is highlighted in all the investigated athletes.
Keywords: Sportlumbar painpain assessment
Introduction
The growing interest in sports activities, both recreational and high-performance ones, has caused, in recent decades, a considerable increase in the pathologies of the musculoskeletal system. Among them, lumbar pain is the most common musculoskeletal disorder in athletes, its rate ranging between 3.3 and 4.6% of overexertion injuries related to sports activity (Pantoja, 2012).
Spinal imbalances in performance athletes include a wide range of possible injuries as a result of direct or indirect trauma, load-induced trauma or that affect a segment presenting degenerative changes.
Lumbar pain is a common symptom for most athletes. Its aetiology is varied and caused by several factors including: age, level of athletic performance, stress on the lumbar area during training, physical fitness (Garcès, 1994).
In performance gymnastics, the interruption of sports activity, especially for medical reasons (lumbar pain), has a negative impact on the performance capacity; therefore, we should develop a complex recovery programme that allows the athletes to return as soon as possible to their specific activity and maintain an optimal state of health. Sports medicine increasingly requires the use of complementary kinetic means in the prophylaxis and recovery of various spinal imbalances, as well as in order to enhance sports performance.
Problem Statement
We present below the main manipulations of the recovery programme based on manual therapies (Shiatsu, Yumeiho, reflexology) (Shigeru, 1998, p. 16; Saionji, 1994, pp. 27-33; Oxenford, 1998, pp. 7-9).
This recovery programme was applied to the female athletes included in our research as follows:
-
Massage of the back area: with the patient lying face down (prone position), the therapist massages her back area using a combined friction-kneading manipulation. Duration: 5-7 minutes.
-
Shiatsu: the therapist exerts thumb pressure from the lumbar to cervical areas on points corresponding to the urinary bladder meridian, which are located on the inner and outer edges of the paravertebral muscles. The pressure is exerted for 2-3 seconds on each point, while the patient is exhaling.
-
Handling the upper chest area: with the patient lying face down, the therapist presses her chest area with the back of the hand on both sides of the paravertebral muscles, and when the maximum tension point is reached, he induces the manipulative impulse in order to align the upper thoracic vertebrae.
-
Handling the middle chest area: the patient adopts the kneeling position, with palms behind the head and fingers together. The therapist’s hands will be placed under the patient’s armpits and will grasp her forearms as close as possible to the wrists. Then, the therapist draws the patient closer to him concomitantly with a lifting motion, regains the straight position, pushes her back with his chest, and when the maximum tension point is reached, he induces the manipulative impulse in order to align the middle thoracic vertebrae.
-
Handling the lower chest and upper lumbar areas: the patient adopts the kneeling position, with the head bent forward. The therapist adopts the standing-on-tiptoe position, with knees perpendicular to the patient’s paravertebral muscles, at the lower angles of the shoulder blades, and grasps her torso from behind, under the armpits, stabilizing her head with his forehead. The abrupt chest traction backwards is performed simultaneously with the maximum head flexion. This manipulation can be done in 3 or 4 support points.
-
Massage of the trapezius muscle and cervical area: with the patient in the kneeling position, the therapist massages her trapezius muscle and cervical area using a combined friction-kneading manipulation. Duration: 5-7 minutes.
-
Shiatsu: the therapist exerts finger pressure on points corresponding to the urinary bladder meridian, which are located on the inner and outer edges of the paravertebral muscles in the cervical area and on pressopuncture points in the trapezius muscle area.
-
Shoulder girdle alignment: the therapist performs a specific palm grasp to align the patient’s shoulder girdle.
-
Cervical spine elongation: the therapist grasps the patient’s chin with the left hand and her occipital area with the right hand, flexes her head to 10-15 degrees and performs an axial traction on her cervical spine to release tension from the cervical vertebrae.
-
Handling the cervical spine: the therapist performs left-right passive rotational mobilizations, a left-right lateral tilt, flexion and extension of the cervical area, and when the maximum tension point is reached, he induces the manipulative impulse in order to release tension from the cervical spine.
-
Massage of the gluteal and supra-trochanteric regions: with the patient lying face down, the therapist massages her left gluteal region with the left hand, elbow in extension, through perpendicular pressure exerted simultaneously with a slight lateral move. The therapist’s right hand stabilizes the patient’s pelvis. The massage of the supra-trochanteric region can be done with both thumbs perpendicular to one another, performing friction with kneading through longitudinal motions, by gently going up along the gluteal muscles. Duration: 5-7 minutes.
-
Shiatsu: the therapist exerts thumb pressure on the points in the lumbar, sacral, posterior-superior iliac crest and gluteal areas.
-
Handling the left/right sacroiliac joint: the patient lies on the right side, with the left lower limb slightly bent and the right one stretched. The therapist kneels with the legs on both sides of the patient’s left calf, presses her left hip with the right elbow and leans the left hand on her left shoulder. When the therapist’s strength gets tense, the patient’s waist twists. If her waist does not twist, the therapist’s body weight must be used to press again immediately. This is repeated on the opposite side.
-
Decoaptation of the left coxofemoral joint: the patient lies on the right side, with the left lower limb stretched and the right one bent. The therapist is in the sitting position at the patient’s feet, on the longitudinal axis; with the legs, he stabilizes the patient’s right lower limb at the ankle and knee, while grasping her left lower limb with both hands – in the distal third of the calf. Slight thigh rotations with flexion of the knee are performed to relax the muscles, and then axial traction is done, followed by tensioning and a manipulative impulse.
-
Plantar reflexology: the therapist performs reflexogenic massage of the feet, stimulating the inner edge of the patient’s foot, which corresponds to the reflexogenic area of the spine.
Research Questions
We assume that reducing the various spinal imbalances in women gymnasts can be achieved through a recovery programme based on the above-mentioned complementary kinetic means and can be objectified through pain assessment questionnaires.
Purpose of the Study
This study aims to objectify, through pain assessment questionnaires, the effectiveness of a complex recovery programme using complementary kinetic means (Shiatsu, Yumeiho, reflexology) on a group of 5 female athletes practicing performance aerobic gymnastics, who show spinal imbalances and suffer from lumbar pain.
5. Research Methods
The research methods used were: theoretical documentation method, experimental method, case study method, comparative analysis method, graphical method.
Experimental research subjects: a group of 5 female athletes, members of the UNEFS Sports Club in Bucharest, practicing performance aerobic gymnastics.
Age of the investigated athletes: between 14 and 17 years
Diagnosis: dorso-lumbar scoliosis, lumbar lordosis, neck pain, back pain, low back pain
Medical history: pain in the lumbar, thoracic or cervical area, pain in the coxofemoral joint, knee, ankle and wrist
Implementation of the recovery programme: during a 9-month period, with a frequency of one session per week for each female athlete
Period during which the experimental research was conducted through pain assessment questionnaires: initial assessment: 22.02.2012; final assessment: 21.11.2012
To objectify the effectiveness of this complex recovery programme based on complementary kinetic means, an initial assessment of the 5 female athletes was carried out through pain assessment questionnaires on 22.02.2012, then the subjects followed the complex recovery programme during 9 months, and finally a new assessment was performed on 21.11.2012 to highlight the effects of this programme.
Assessment methods:
Pain assessment questionnaires:
The Roland-Morris Low Back Pain and Disability Questionnaire (Roland & Morris, 1983)
The Visual Analogue Scale for Pain (VAS Pain)
In the following drawing (Figure
Findings
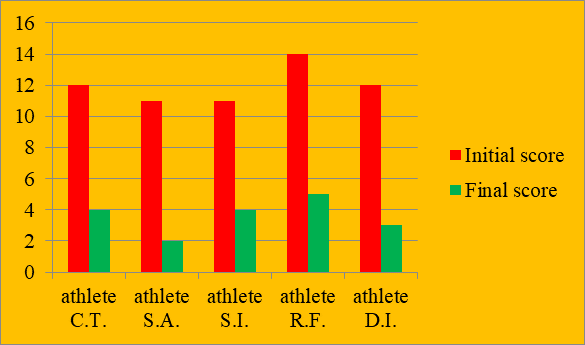
The aforementioned questionnaires were completed by the 5 athletes practicing performance aerobic gymnastics before and after 9 months of participation in the complex recovery programme based on complementary kinetic means.
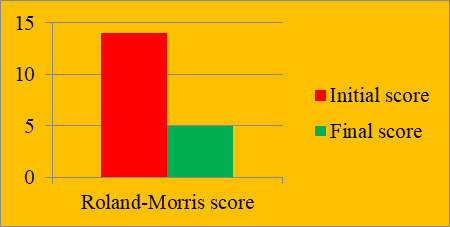
Case study no. 1 – Athlete C.T. – dorso-lumbar scoliosis
The athlete initially recorded 10 points in the Roland-Morris Low Back Pain and Disability Questionnaire, and after 9 months of participation in the recovery programme, 4 points, indicating a 66% (8/12x100) improvement (Figure
The Visual Analogue Scale for Pain (VAS Pain) highlights moderate/intense pain in the lumbar area, moderate pain in the thoracic area, mild pain in the cervical area and moderate pain in the left coxofemoral joint. After 9 months of participation in the recovery programme, a pain relief was noted in all the previously mentioned areas.
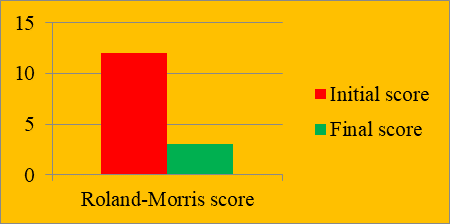
Case study no. 2 – Athlete S.A. – lumbar lordosis
The athlete initially recorded 11 points in the Roland-Morris Low Back Pain and Disability Questionnaire, and after 9 months of participation in the recovery programme, 2 points, indicating an 81% (9/11x100) improvement (Figure
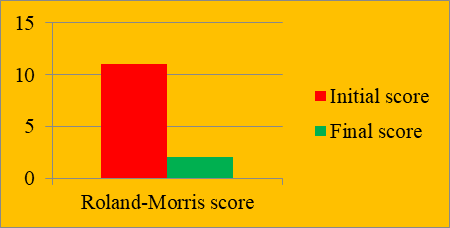
The Visual Analogue Scale for Pain (VAS Pain) highlights moderate/intense pain in the lumbar area, moderate pain in the thoracic and cervical areas and moderate pain in both knees and the coxofemoral joint. After 9 months of participation in the recovery programme, a pain relief was noted in all the previously mentioned areas.
Case study no. 3 – Athlete S.I. – lumbar lordosis
The athlete initially recorded 11 points in the Roland-Morris Low Back Pain and Disability Questionnaire, and after 9 months of participation in the recovery programme, 4 points, indicating a 63% (7/11x100) improvement (Figure
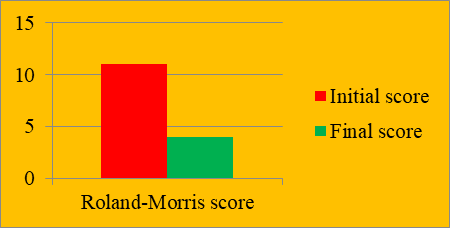
The Visual Analogue Scale for Pain (VAS Pain) highlights moderate/intense pain in the lumbar area, mild pain in the cervical area, intense pain in the left coxofemoral joint and moderate pain in both wrists. After 9 months of participation in the recovery programme, a pain relief was noted in all the previously mentioned areas.
Case study no. 4 – Athlete R.F. – dorso-lumbar scoliosis
The athlete initially recorded 14 points in the Roland-Morris Low Back Pain and Disability Questionnaire, and after 9 months of participation in the recovery programme, 14 points, indicating a 64% (9/14x100) improvement (Figure
The Visual Analogue Scale for Pain (VAS Pain) highlights moderate/intense pain in the lumbar area, moderate pain in the thoracic area, moderate pain in the left coxofemoral joint and mild pain in the left posterior thigh. After 9 months of participation in the recovery programme, a pain relief was noted in all the previously mentioned areas.
Case study no. 5 – Athlete D.I. – dorso-lumbar scoliosis
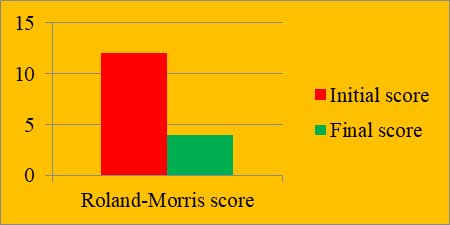
The athlete initially recorded 12 points in the Roland-Morris Low Back Pain and Disability Questionnaire, and after 9 months of participation in the recovery programme, 3 points, indicating a 75% (9/12x100) improvement (Figure
- The Visual Analogue Scale for Pain (VAS Pain) highlights moderate/intense pain in the lumbar area, moderate pain in the thoracic area and moderate pain in the right ankle joint. After 9 months of participation in the recovery programme, a pain relief was noted in all the previously mentioned areas.
Figure
Conclusion
In conclusion, we can state that, from our observations and the pain assessment questionnaires completed by the female gymnasts before and after 9 months of participation in the complex recovery programme, a decrease in the pain sensitivity threshold is highlighted in all the investigated athletes.
Back pain is reported more and more frequently in sports activity, being one of the main causes of muscle imbalances induced by an improper training method and the adoption of an incorrect posture when performing various sports gestures.
Athletes can practice their favourite sport without restrictions and with successful results even when they have spinal imbalances and back pain, provided that they benefit from appropriate training, effective prevention methods and correct treatment.
References
- Garcès, G. (1994). Espondilolisis y espondilolistesis en el deporte. Archivos de Medicina del Deporte, XI(42), 181-186.
- Oxenford, R. (1998). Reflexología – técnicas sencillas para aliviar el estrés y estimular la mente. Barcelona: Parramòn.
- Pantoja, C. S. (2012). Lesiones de la columna lumbar en el deportista. Revista Medical Condes, 23(3), 275-282.
- Roland, M., & Morris, R. (1983). A study of the natural history of back pain (Part I: Development of a reliable and sensitive measure of disability in low-back pain). Spine, 8, 141-144.
- Saionji, M. (1994). Miracolul secolului XX – Yumeiho. Timişoara: Eurobit.
- Shigeru, O. (1998). Libro completo de Shiatsu: Teoria, practica, diagnostico y tratamientos. Madrid: Gaia.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
16 February 2019
Article Doi
eBook ISBN
978-1-80296-054-9
Publisher
Future Academy
Volume
55
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-752
Subjects
Sports, sport science, physical education
Cite this article as:
Acasandrei, L. (2019). Using Complementary Kinetic Means For Gymnasts With Spinal Imbalances And Lumbar Pain. In V. Grigore, M. Stănescu, M. Stoicescu, & L. Popescu (Eds.), Education and Sports Science in the 21st Century, vol 55. European Proceedings of Social and Behavioural Sciences (pp. 353-360). Future Academy. https://doi.org/10.15405/epsbs.2019.02.44