
Assessment Of Investment Activity In Human Capital “Health”


Abstract
During global competition, sustainable economic growth is influenced by investments in human capital. Under conditions of the complex demographic situation in Russia, a major challenge is human capital “health”. Investments in capital “health” provide foundation for developing high-quality cumulative human capital of future generations, are twofold and may have different financing sources. Consequently, one should assess adequately investment activity efficiency and find out factors influencing it. The article examines the essence of investments in capital “health” in terms of human capital theory. Approaches to the definition of the investment activity and methods of its assessment are analyzed. The multi-factor indicator of the investment activity level is presented; it is consistent with the public policy related to nation’s health, possibilities of individuals to invest and real public health expenditures. Statistical data of health indicators and levels of investments in health protection in some countries are analyzed. The level of Russian activity of investing in capital “health” is defined; interpretation of factors influence on the investment activity index is presented. The proposed methodology allows defining directions of influence on creating sources of investments in human capital “health” and it can be used as an analysis instrument when developing the country’s social policy. The given methodology allows comparing levels of investment activity in different countries and drawing conclusions about real possibilities of transition from the post-industrial economy to the “innovative” one, as capital “health” is a foundation for qualitative national human capital having high levels of knowledge and corresponding competences.
Keywords: Investment activityassessmenthuman capitalhealth
Introduction
The investments in the capital “health” are traditionally understood as material, technological and financial recourses invested by someone for the implementation of the programs aimed at making the individuals healthy. They are not linked with the current consumption; they are based on investing own or loan capital and come with the definite social and economic effect that must be strategically obtained by the investor.
The essence of the investments in capital “health” mainly lies in the possibility to reduce the current expenditures of the public and individual for the health recovery.
The peculiarity of capital “health” is that the investments in it are, by definition, twofold.
Firstly, according to the principles of the traditional economic theory such investments allow an individual to increase the volume of his/her capital and (or) to increase its productivity. From this perspective, investments allow a person to deal with larger volume of revenues in the future at the cost of lowering the consumption during the present period.
Secondly, investments in specific capital “health” allow a person to reach a higher level of usefulness without regard to the wealth volume. It means that if two persons have an equal wealth level regarded as definite benefits reserve and an equal income flow the healthier person will have a higher level of welfare. It is explained by the higher capacity of a healthy person to perceive the usefulness of the physical goods and services, besides, a healthier person incurs less expenses when consuming goods. Thus, it would not be correct to regard investments in capital “health” only from the point of view of the future maximized revenue flow; these investments are necessary because a person gives certain value to the resource “life” that he wants to consume with the least expenses.
Problem Statement
The starting point for the public (region) when assessing the social component of capital “health” must be the conception of the qualitative composition of the population. The quality of population is regarded as an entire set of medical-genetic and social-psychological characteristics of people, their physical health, the level of the intellectual abilities development, psychophysiological context of life; the mechanisms of the reproduction of the intellectual potential of the society. The qualitative composition of population defines the quality of the social-employment potential of the country and its stable economic growth. The development of the qualitative composition of population mainly depends on the activity of investing in capital “health”. This poses a problem of the investment activity assessment for the goals of making decisions and defining the social-economic priorities concerning the nation’s health.
Research Questions
The studies of the theoretical, methodological and practical issues in the sphere of assessing the investments in the human capital were carried out by the following scientists: Becker (1962), Shultz (1971), Schumpeter (1999), Howitt (2005), and Royal, & O’Donnell, (2005). The issues of the investments in health were researched by Grossman (1972), O’Brien (1995), Fogel (2002), Kalemli-Ozcan (2016), Drummond (1987), Halkiv and Kulyniak (2016), Rivera and Currais (1999).
Despite the significant number of research, the issues of motivation and activity of investments in human capital “health” must be studied further and, first of all, at the population level. Thus, there is a need for the scientific justification of the growth of activity of investing in the development of human capital “health”.
Purpose of the Study
The purpose of the article is to reveal the reasons and factors influencing the investments in human capital “health” and to work out the methodology of the assessment of the investment activity and its significance for Russia on the grounds of the conducted research.
Research Methods
The logical method was used when analyzing the incentives of different subjects investing in capital “health”. In the course of discovering factors influencing the level of investment activity, the induction method was used, namely, the method of corresponding changes. The index-linked statistical method was used when creating the model of assessing the activity of investment in human capital “health”.
Findings
In the context of the “human capital” theory, the investments of the financial resources in the creation of human capital “health” are not only the basis for the personal development of an individual, they provide a platform for the creation of cumulative “human capital” of the future generations.
Like all material assets, capital “health” is vulnerable to wear. From this perspective it is possible, perhaps, to divide the investments in capital “health” into the primary ones and investments in major and current repairs. Not all the funds are invested by an individual. As a rule, the investments are divided between an individual and the government just as these subjects share the basic and funded parts of the pension.
Investing in capital “health” may be presented in several ways:
an individual’s investments in himself/herself – during the life a person invests in himself/herself and he/she is an owner of the knowledge, abilities, skills (“competences” as it is named nowadays) that allow him to be an active subject in different systems of activity;
the economic entities’ investments in the health of the staff are conditioned by the creation of additional economic benefits of the employees’ increased performance and reduced losses of the working time;
capital “health” is a national value, consequently, the maintenance of the human capital at the appropriate level is the concern not only of the separate individuals, health authorities but of the entire society.
Thus, the social-economic aspects of the researched problem can be studied from three points of view: the regional interests, the interests of the economic entities and individuals.
The problem of creation of capital “health” and increased return is related to the problem of the regional social-economic systems development.
As for the regional priorities of investing in capital “health”, the following principles may be the starting point:
region is a reproductive social-economic system;
the goal of the regional economic functioning is qualitative life-support of the population;
the region’s end product is the reproduction of cumulative “health capital” that, on the one hand, meets the current demands of the region’s economy and, on the other hand, complies with the requirements of the developing production;
regional peculiarities related to the natural-climate factors, social-economic and national-cultural traditions form the basis for the creation of cumulative capital “health”;
region is a subject able to solve the problems of investments in capital “health” at the expense of its own financial resources.
As the regional and public interests are connected with the economic growth, the regional policy involves the location of production. It draws into analysis another group of subjects with the specific interests – economic entities.
The regional population is the most important resource for the economic entities and for the economy in general. They are the employees who integrate the financial, production and other resources in order to ensure the efficient functioning of the economic entities. Life values and interests of many employees change under the changing conditions of the environment. People may become more interested in their health and well-being. They may also expect that the quality of their working life will ensure the comfortable conditions in accordance with their concerns, as well as health and security (Yakobson, Kirillova, Batsyun, Lidin, & Gafarova, 2009).
Rapid response of the managers to the personal needs and expectations of the employees is a key condition of the increased revenue of the firm. The researches show that there is an evident link between the satisfaction of the needs of the organization’s human capital and higher labour productivity. Thus, the managers must apply the innovative approaches to the capital “health” of their employees which will allow the workers to increase productivity.
However, this statement is true only if there is no excess labour supply at the market. As the experience shows in case of unemployment, Marx’s model of the employees’ exploitation begins to work.
According to the research of the Association of Managers, the share of investments in the protection of the staff’s health and labour in the structure of the social investments of the Russian business is only 13% (Fig. 01).
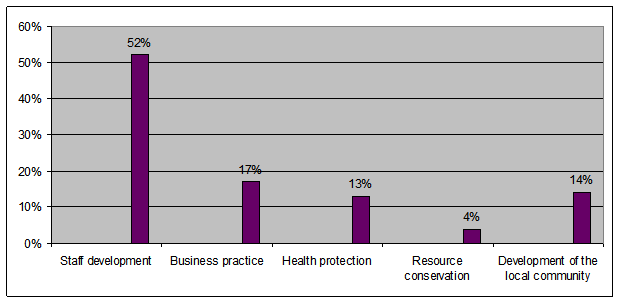
Notably, the participation of businesses in the development of community (including the maintenance of the employees’ health) is changing from the irregular charity to the pragmatic social investments (Litovchenko, 2004).
As to an individual, he/she invests in capital “health” according to his/her desires. Empirical evidence shows the tendency to invest in this asset is differentiated between the different layers of the population of one country and between the populations of different countries.
It is well-known that in the economic theory, the medical services are classified as luxury goods, as the demand for them grows faster than the incomes of the population. Thus, the medical services are similar to such welfare goods as savings, touristic, financing, juridical, educational services.
It is clear that the low propensity to invest in capital “health” is naturally explained by the function related to the welfare level. The low level of welfare means that a person has not enough goods or values with the extremely high marginal benefit – food, clothes, accommodation and other goods that constitute the foundation of the human existence in the social community.
Obviously, in this case the investments in capital “health” are either equal to the basic ones (that is, the governmental ones) or exceed them only a little. Therefore, the low basic indicators of the people’s health in the majority of the Russian regions can be explained by the low incomes.
But there are two questions. Will people invest in their health a larger part of their increased income (it is indicative of the higher marginal propensity to the investments in capital “health”)? How can one know that they will not have demands for some other goods that they will consider more attractive than health?
Firstly, the intention of a person to invest in capital “health” depends on his/her intention to use this asset for as long as possible. If a person’s forecasts cover a short period of time his/her propensity to invest will be lower as he/she intuitively extends the current state to the nearest future. In this case the strategic investments cannot be mentioned, in the best variant these investments will be directed to the current repairs that are necessary due to the sudden reduction of capital “health”.
Secondly, the volume of investments in capital “health” will be larger in the society where the individuals’ responsibility before their families is higher. This indicator has heavy correlative dependence on the volume of investments in culture capital. Though, it should be noted that the habit of responsible attitude to the health is not a function related to the current investments in culture capital, it correlates with the accumulated volume of this capital in the society.
Thirdly, the volume of investments in capital “health” is defined by an individual’s ability to manage this asset as he/she sees fit. Simply put, the greater the degree of freedom a person has in the society, the more he/she invests in capital “health”. In this case, as with any investment decision, the factor of political risk is of great importance.
Finally, the level of investments in health depends to some extent on the way of consuming this resource reserve. This consumption may be twofold. In the vast majority of cases capital “health” is “spent” during the working process, and this consumption can be more or less intensive depending upon the profession, place of work, specificity of the staff, personal characteristics of an individual. At the same time, an individual can recover his/her capital “health” during the leisure time.
Therefore, the level of investments in capital “health” is conditioned by different incentives of investors, and their investing activity is influenced by different factors the most important of which is the level of financial resources. This relationship can be described as the following function:
where
Thus, among the indicators of the World Health Organization showing the level of the national health via the social-economic indices, the following groups were classified:
factor-based indices indicating the level of the public investment activity (the health expenditures as a percentage of GDP, health expenditures per capita);
factor-based indices indicating the level of an individual’s one investment activity (GNP per capita).
They are presented for a number of countries
In the author’s opinion, the indices of the factor-based indicators the grounds of which are formed by the maximum values of the factors in the countries can be used for the calculation of the integral criterion of the investment activity in capital “health”:
where
The calculation of the indices of the factor-based indicators is made by the following formulae:
where
where
where
Let us define the integral index of the investment activity in capital “health” in Russia and other countries using the proposed model (Table
The index of the investment activity in capital “health” for Russia is:
Continuing these calculations, it seems logical to present the indicators characterizing the national levels of health and death in the analogical form of indices:
The calculation of the indices of the efficient indicators is made by the following formulae:
where
where
Therefore, the basis is the effective value of the indicator (maximum or minimum, correspondently) in the countries included in the analyzed group:
maximum health expenditures, the length of the healthy life, GDP per capita, health expenditures per capita;
minimal death rate.
The calculated indices are shown in Figure
The analysis showed that when creating, the rating of the investment activity in capital “health”, Russia is almost at the bottom of the list of the analyzed countries. The index of the Russian investment activity is only 0.06, whereas in Sweden it is 0.59, in Germany – 0.52, in Norway – 0.82, in France – 0.4 of the maximum efficient level. The values of the index of the investment activity in capital “health” correlate with the values of indices of the male and female longevity (Figure
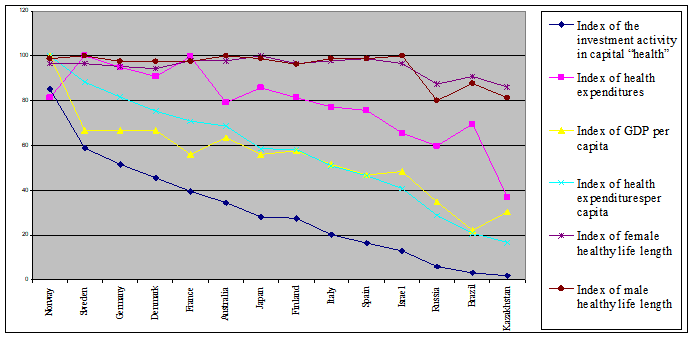
The indices calculated according to the proposed methodology show that the policy of investing in capital “health” in Russia is unsatisfactory. The underestimation of the health resources as an object of market economy is a deterrent to the efficient development of many countries and regions. In Russia as well as in many countries of the post-Soviet epoch there are “unhealthy economies”, that is, health as an economic category is neither the assessment object, nor criterion, nor the goal of their development. It is demonstrated by the extremely low longevity of people (65-75 years) compared with the human genetic potential (100-120 years) (Drummond, 1987).
After the analysis of the Russian investment activity in capital “health”, the spider chart of the above-mentioned characteristics according to WHO statistics for 2015 was created (Figure
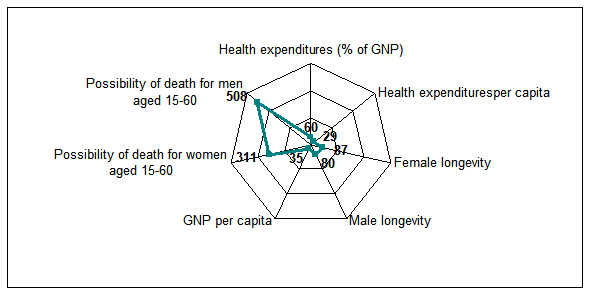
The undertaken analysis shows that the per capita income in Russia is 35% of the maximum one in the countries of the researched group. Health expenditures as a percentage of GDP is 60% when compared with the maximum expenditures in the countries, and health expenditures per capita – only 29%.
The longevity of men and women in relation to the maximum one in the researched countries is 20% and 13% less, correspondently. The excessive rate of the adult mortality is noted –5.1times higher among men and 3.1 times higher among women in relation to the minimal death rate.
The main current policy direction of the public related to the increased capital “health” in the national economy is the increase of the population income especially of the people living below the poverty line. In this case the majority of the income will be consumed whereas the volume of investments in capital “health” will not change or rise only a little. It makes sense to increase the public volume of investments in capital “health” at the same time.
As a rule, the government incurs the obligation to make initial investments in capital “health”. This includes the public expenditures to save a person’s life and to support the basic characteristics of capital “health”. Particularly, this includes the programs of immunization coverage, mother and child health protection, free medical care, preventive and anti-epidemic measures.
The marginal usefulness of these investments is extremely high, but at the same time the government cannot be sure that an individual is aware of the value of this usefulness. If the government relied only on the private initiative, the society would bear the high costs addressing the lateness of these investments.
Conclusion
The proposed model of the process of investing in capital “health” may be used to explain the investor’s priorities when defining the optimality of the definite solution in the investment process. The choice of the best solutions related to the investments in the national health must be undoubtedly based on the results of the economic analysis with the usage of the methods of assessing the economic efficiency of investments.
References
- Becker, G. (1962). Investment in Human Capital: Theoretical Analysis. Journal of Political Economy, 70, 9-49. doi 10.1086/258724.
- Drummond, M.F. (1987). Resource allocation decision in health care: a role for quality of life assessments? J.Chron. Dis, 40, 605-616. oi.org/10.1016/0021-9681(87)90021-X.
- Fogel, R. W. (2002). Nutrition, Physiological Capital, and Economic Growth. РАНО Headquarters Washington. DC October 3, 29
- Grossman M. (1972). On the concept of health capital and the demand for health. Journal of Political Economy, 80.
- Halkiv L., & Kulyniak I. (2016). Analysis of Healthcare Costs in the Context of Investment Renovation of Human Capital. International Economics Letters, 5, 44-53.
- Howitt, P. (2005). Health, human capimal and economic growth: a schumpeterian perspecmive. РАНО Headquarters Washington. February 9, 29.
- Kalemli-Ozcan S., (2016). A Stochastic Model of Mortality, Fertility, and Human Capital Investment. Journal of Development Economics, 70, 1. 103. doi.org/10.1016/S0304-3878(02)00089-5.
- Litovchenko, S. E. (2004). Corporate social responsibility: a report on social investment in Russia. Association of Managers. Retrieved from: http://www.undp.ru/download.phtml?$350.
- О 'Brien, B. (1995). Principles of economic evaluation for health care programs. J.Rheumatol, 22, 1399-1402.
- Rivera, B., & Currais. L. (1999). Income Variation and Health Expenditure: Evidence for OECD Countries. Review of Development Economics, 3, 258.
- Royal, C., & O’Donnell, L. (2005). Embedding human capital analysis in the investment process: a human resources challenge, Asia Pacific Journal of Human Resources, 43, 117-136. doi.org/10.1177/1038411105050308
- Schumpeter, J.A (1999). Theory of economic development (research business profits, capital, credit, interest and cycle conjuncture). Moscow, Publishing house "Progress".
- Shultz, T. (1971). Investment in Human Capital. London, N.V.
- Yakobson, A.Ya., Kirillova, T., Batsyun, N.V., Lidin, K.L., & Gafarova, E.V. (2009). Some Problems of Transition to post-industrial Development in the Siberian Region. Prace Komisji Krajobrazu Kulturowego, 14, 9-17.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
17 December 2018
Article Doi
eBook ISBN
978-1-80296-049-5
Publisher
Future Academy
Volume
50
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-1464
Subjects
Social sciences, modern society,innovation, social science and technology, organizational behaviour, organizational theory
Cite this article as:
Gafarova, E. (2018). Assessment Of Investment Activity In Human Capital “Health”. In I. B. Ardashkin, B. Vladimir Iosifovich, & N. V. Martyushev (Eds.), Research Paradigms Transformation in Social Sciences, vol 50. European Proceedings of Social and Behavioural Sciences (pp. 384-393). Future Academy. https://doi.org/10.15405/epsbs.2018.12.47