
Acute Psychophysiological Responses To Laboratory-Induced Stress In Different Groups: An Exploratory Study


Abstract
Occupational stress has been broadly acknowledged as a global challenge and has been the focus of concern for many researchers as stress affects workers’ health and performance. Hence, the current study aimed to: a) assess psychophysiological stress among different occupational groups and b) identify differences, if any, between these groups using self-reports and heart rate variability (HRV) measures. Three different occupational groups (students; firefighters; air traffic controllers) of nine people in each group were analysed. The Trier Social Stress Test (TSST;
Keywords: Trier Social Stress Testoccupational healthheart rate variability”“psychophysiological stress”“bio-sensing platform”
Introduction
Stress has been defined as an imbalance between demands and resources. When facing a threat, the individual perceives the situation as challenging or exceeding one´s individual resources and endangering well-being (Lazarus R.S., 1984). Considering that adults spent a considerable amount of time in working contexts, researchers in the area of occupational health commonly use the term “occupational stress” to categorise stress at work. Occupational stress is broadly recognized as a global challenge and has been the focus of concern for a number of researchers (Cartwright & Cooper, 1997; Ganster & Rosen, 2013; McLeod, 2011). Occupational stress refers to negative experiences caused by an imbalance between job demands and the response capability of the workers. When job demands are too high to manage, stress responses are likely to occur (Schaufeli & Enzmann, 1998).
Stress responses are characterized by an onset of body changes. Cannon (Cannon, 1935) first described these as the “fight-or-flight” response. This is our body's primitive, automatic, inborn response that prepares the body to "fight" or "flee" from perceived attack, harm or threat to our survival. Once a danger is perceived, the autonomic nervous system (ANS) is activated. The ANS has a parasympathetic (rest) and a sympathetic (activation) branch. When a threat is perceived, the parasympathetic nervous system is inhibited and the sympathetic nervous system is triggered (Gordan, Gwathmey, & Xie, 2015). Therefore, the discharge of stress-related hormones evokes several physiological responses, such as the vasoconstriction of blood vessels, increased blood pressure and breathing rate, increased muscle tension and heart rate (HR) and a decrease in heart rate variability (HRV) (Taelman, Vandeput, Spaepen, & Van Huffel, 2009).
The impact of stress in the health condition is currently well recognized. Numerous personal, organizational, and medical costs are being associated with increased stress health problems, such as heart disease, hypertension, upper respiratory tract infections, peptic ulcers, reduced immunity, migraines, alcoholism, depression, suicidal tendencies, anxiety, as well as other mental disorders (Babatunde, 2013) (Smith, Karsh, Carayon, & Conway, 2003). Particularly, the link between work-related stress and cardiovascular disease has been well established (Schnall, Dobson, & Landsbergis, 2016) and Electrocardiogram (ECG)-derived measures, such as the HRV, are being used to monitor the direct effects of stress in the cardiovascular system (Föhr et al., 2017). The HRV defines the complex variation of beat-to-beat intervals mainly controlled by ANS over the interaction of sympathetic and parasympathetic activity and it can be indexed by time- and frequency-domain parameters (Shaffer, McCraty, & Zerr, 2014). Methods in the time-domain define the intervals between successive normal QRS complexes (the Q-wave, R-wave, and S-wave). Measurements in the frequency-domain provide information of how heartbeat power (variance) distributes as a function of frequency ("Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology," 1996).
Researchers interested in understanding the psychophysiological impact of acute stress responses in humans require a valid and reliable acute stressor that can be used under experimental conditions. The Trier Social Stress Test (TSST) has been proposed as a standard protocol for the experimental induction of stress in the field of basic and applied psychobiological research (Kudielka, Hellhammer, Kirschbaum, Harmon-Jones, & Winkielman, 2007) (Frisch, Häusser, & Mojzisch, 2015). The TSST was created in 1993 at the University of Trier by Clemens Kirschbaum and colleagues (Kirschbaum, Pirke, & Hellhammer, 1993). Hundreds of research studies have used the TSST in order to investigate the impact of acute stress on human neurobiology (Allen et al., 2017). Overall, the TSST consists of three successive phases: 1) A preparation period for 3 minutes); 2) a free speech task in which the participants have to argue why they are the best candidate for the job they wish to apply for 5 minutes); and 3) a mental arithmetic task (e.g. count down from 1022 by 13’s for five minutes). The two tasks are performed in front of a selection committee, consisted of three jury members that do not respond emotionally during the test, which makes the situation stressful for the participant (Kirschbaum et al., 1993). The TSST has been used to examine the interplay between social-evaluative threat, neurophysiological stress responses, social cognition and social behaviour. This tasks involves social evaluation, unpredictability and uncontrollability (Allen et al., 2017). The TSST tasks involve active cognitive processing and responses, and are generally associated with diverse degrees of parasympathetic withdrawal and sympathetic stimulation (Allen et al., 2017).
Problem Statement
As discussed previously, stress is a complex and multidimensional process, which encompasses several dimensions of analysis. In order to fully understand the stress concept, interdisciplinary research methods are needed, combining both psychological and physiological measures. However, the direct physiological measurement of stress is a complex process (Hickman, Fricas, Strom, & Pope, 2011). The consolidation of objective and reliable stress biomarkers and health has been a challenge for researchers and clinicians. One is a lack of consensus on the meaning and operationalization of the concept of stress (Rodrigues, Kaiseler, & Queirós, 2015). Another is the absence of a reliable and comprehensive background with which to investigate the way in which organisms function and adapt in a constantly changing setting (Thayer, Ahs, Fredrikson, Sollers, & Wager, 2012). Although HRV has been proposed as a reliable and feasible measure for the quantification of stress responses, little agreement exists in the literature for the most suitable HRV-based metric for the detection and differentiation of stress events (Castaldo et al., 2015).
Research Questions
Taking into account the shortcomings in this area in the literature, the current study aims to provide novel findings and overcome some of the previous limitations in the assessment and quantification of stress concept. Hence, a general research question was formulated: 1)Does the Trier Social Stress Test (TSST) have the potential to evoke different psychophysiological stress reactions among different occupational groups?
Purpose of the Study
The current study sought to assess psychophysiological stress, by examining ECG-derived measures, using different occupational groups in order to understand if there are differences in stress responses between groups with different work backgrounds (students, firefighters and air traffic controllers in this study). For that purpose, the TSST was used as a testing platform, since this method is a gold standard stress task for inducing and evaluating stress. A bio-sensing wearable platform integrating different biomedical systems that enable the acquisition of real time ECG signals, computation of linear Heart Rate Variability (HRV) features and collection of perceived stress levels was developed and implemented. To the best of our knowledge, this is the first study investigating and comparing psychophysiological stress responses among different occupational groups.
Research Methods
Participants
The current study involved a convenience sample of three different occupational groups which are exposed to different type of stressors. All the participants were Portuguese. The independent variable was “profession” and the dependent variable was “stress” (using psychophysiological metrics).
A detailed description of the participants is given in the table below (Table 01).
Data collection
The exclusion criteria for the study were participants having a history of cardiovascular disease and/or taking prescription drugs known to affect cardiovascular function. The study was approved by the University of Porto Ethics Committee. All informants were carefully instructed about the study protocol and gave written informed consent prior to examination.
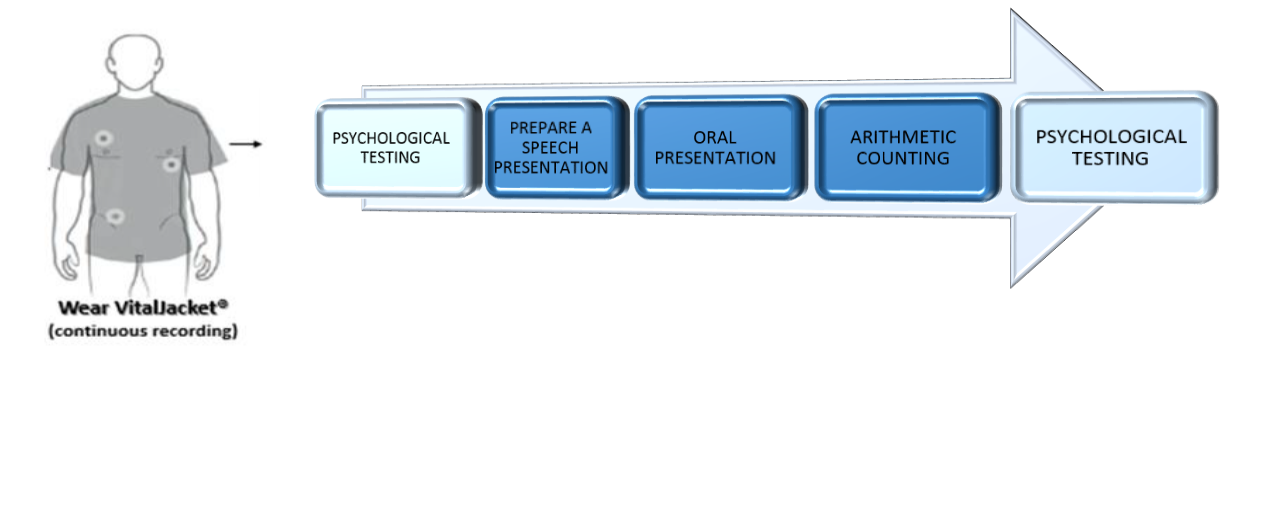
A presentation session was organized to explain the aim and the overall protocol of the study. The protocol lasted approximately 15 minutes and included a combination of tasks as shown in Figure
Participants completed the demographic, medical survey and the State-Trait Anxiety Inventory (STAI 6-item short-form) (Marteau & Bekker, 1992). Emotional, physical, and cognitive aspects of stress can be quantified using this self-report assessment instrument. Considering that our goal was to evaluate the differences in state anxiety from a non-stress to a stress moment, we chose the short-form of the STAI, that according to the authors is more sensitive to fluctuations in state anxiety (Marteau & Bekker, 1992).
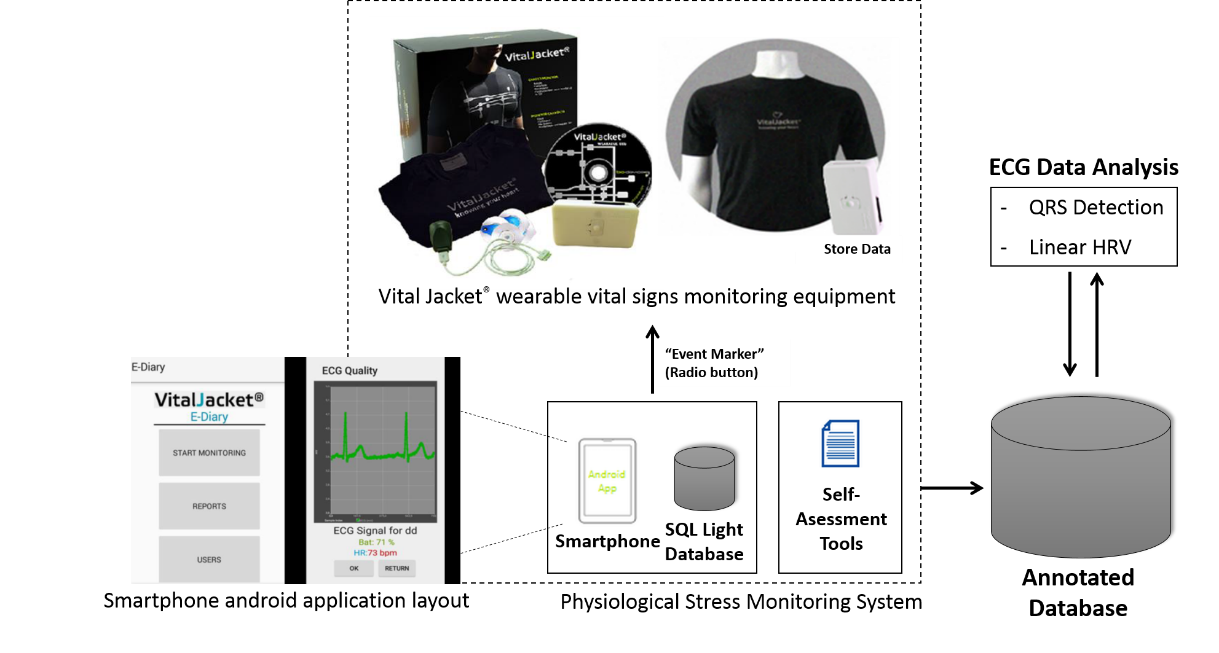
Participants were equipped with Vital Jacket
After being equipped with the Vital Jacket® equipment, participants performed the TSST. The STAI questionnaire was filled up before and just after the TSST.
Data analysis
Statistical analysis was performed using IBM SPSS AMOS (v.24) software. Taking into account the small sample number, some parameters failed in the normality test (Shapiro-Wilk Normality Test), so all parameters were analyzed using non-parametric statistical tests. Kruskal-Wallis test was the non-parametric alternative test used to test if there were significant statistical differences on ECG-derived measures between the three groups, and the Wilcoxon signed-rank test was also used to compare STAI results from the beginning to the end of the TSST for each group (Pallant, 2013).
In order to extract heartbeat information from the ECG recordings, a software from Biodevices S.A, with an ECG analyzer was used. This software has an algorithm based on the one developed by Pan Tompkins (Pan & Tompkins, 1985) incorporating ECG physiological filters to detect the “R” points of the ECG waveform. Using this analyzer, the RR interval (time between two consecutives “R” peaks in the ECG) was extracted. A simple verification according to Clifford et al. (Clifford, Azuaje, & McSharry, 2006) was made to verify if all the RR intervals were physiologically correct. The RR intervals that have physiological validation are named normal-to-normal (NN) intervals. ECG-data were normalized using Voss ´s et al. (2015) study with a healthy population. These authors conducted a study with the largest dataset of healthy subjects (N=1906) and analyzed age and gender-related HRV differences.
Following the guidelines presented by the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology ("Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology," 1996), different HRV time and spectral domains parameters were evaluated (see Table
Findings
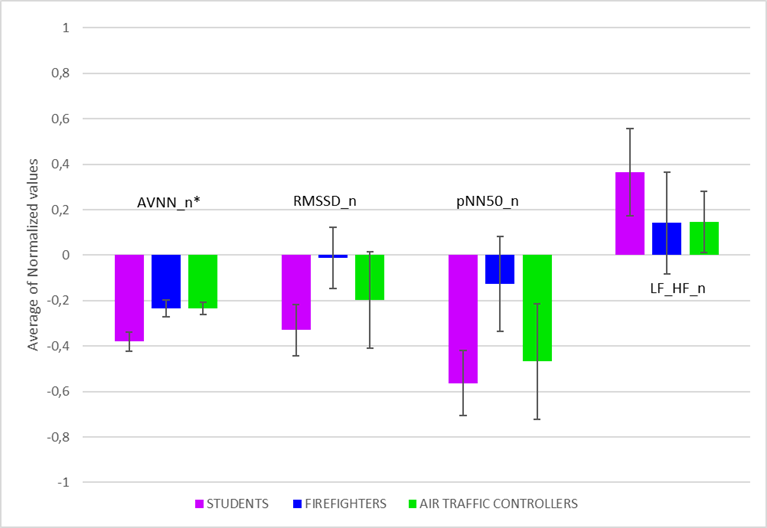
Regarding the ECG analysis, two blocks of 5-minutes were analysed for each participant, resulting in 54 blocks of 5-minute clinical grade-ECG. ECG-derived measures (AVNN, RMSSD, pNN50 and LF/HF) were normalized according to normative values provided by Voss et al. (Voss, Schroeder, Heitmann, Peters, & Perz, 2015), considered the gold standard among the HRV-related studies available in literature and corresponding to each participant’s gender and age interval.
The obtained values are suggestive of stress in all groups, when compared to normative values (Figure
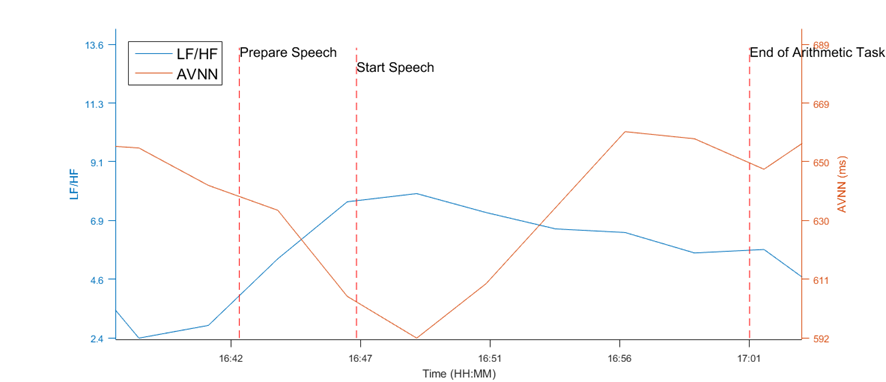
Below is an example of how ECG-derived measures (AVNN and LF/HF) change during the stress task. (Figure
STAI scores showed that participants had higher levels of stress during the stress experiment (1.93 ± 0.51) compared to the non-stress condition, before the TSST (1.80 ± 0.56). However, Wilcoxon test does not confirm the significant difference in the two stages.
Discussion
This study aimed to assess psychophysiological stress among different occupational groups and to understand if there are differences between these groups, using self-reports and HRV measures. Physiological results found support for the importance of using the TSST as a gold standard procedure designed to produce a psychophysiological stress response. ECG-derived measures were indicative of stress, when compared to normative values (Voss et al., 2015). Lower values of AVNN during the TSST suggest an overall increase in heart rate or cardiac sympatho-excitation, typical in stress situations (Tharion, Parthasarathy, & Neelakantan, 2009). The AVNN is an indicator of the ratio of the cardiac sympathetic to parasympathetic tones. A similar study conducted with students using TSST, showed that AVNN metric was the most reliable metric to recognize mental stress (Pereira, Almeida, Cunha, & Aguiar, 2017). The trend of AVNN proves its efficacy in distinguishing mental stress among different occupational groups. Changes in the RMSSD and pNN50 are both reported in the literature to reflect parasympathetic modulation ("Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology," 1996). Hence, decreases of RMSSD and pNN50 during the stress condition reflected a depressed HRV, typical during stress (Castaldo et al., 2015). Within the frequency-domain, a significant increase in the LF/HF ratio during the stress condition was also found, also indicating the effect of stress on sympathovagal balance. Higher values reflect the domination of the sympathetic system over the parasympathetic one; typical of stress responses (Kaur, Bhalla, Bajaj, Sanya, & Babbar, 2013). These results were concordant with an elevation of self-perception measures of stress (STAI 6-item) in the stress condition.
The significant reduced AVNN in the student group along with other ECG-derived measures showed a consistent behaviour, suggesting more stress in the student group. A possible explanation of these results could be related with the fact that these groups have different work experience backgrounds. Firefighting and air traffic control are known for being very stressful occupations (Jou, 2013) (Perrin et al., 2007). Therefore, these professionals would be more used to dealing with stress on a daily basis, particularly with the unpredictability and uncontrollability of daily encounters, and these components are part of the TSST. Another possible explanation could be the age difference. Students in this sample were young compared to the other two groups. Being still young could have caused the stress levels to be higher compared to older people.
This study has limitations, particularly the small sample size and the simplistic protocol of the study. Despite that, this study shows that the TSST is a useful tool for the assessment of stress in different groups. Possible implications of this study could be the design of protocols whereas is important to assess the effects of stress on individuals, using experimental settings (ex., examining the effects on working memory and attention (Olver, Pinney, Maruff, & Norman, 2015)). Findings confirm the negative impact of stress in a broad range of cognitive functions. Additionally, the TSST can be used to investigate biological pathways between stress and cardiovascular disease (Birkett, 2011). Finally, the use of this type of bio-sensing platforms, in association with a wide range of wearable devices recently developed within the Internet of Things (IoT) can be a valuable contribution for the development of “smart”, low-cost, simple and affordable quantified health technologies extended to a broad range of occupations.
Acknowledgments
We would like to thank all the participants who agreed to participate in this study. This work has been supported by the National Funds through the FCT Fundação para a Ciência e Tecnologia (Portuguese Foundation for Science and Technology) within the project VR2Market CMUP-ERI/FIA/0031/2013 and FCT PhD grant PD/BD/135023/2017.
References
- Allen, A. P., Kennedy, P. J., Dockray, S., Cryan, J. F., Dinan, T. G., & Clarke, G. (2017). The Trier Social Stress Test: Principles and practice. Neurobiology of Stress, 6, 113-126. doi:10.1016/j.ynstr.2016.11.001
- Babatunde, A. (2013). Occupational Stress: A Review on Conceptualisations, Causes and Cure. Economic Insights-Trends & Challenges, 2(3), 73-80.
- Biodevices (Producer). (n.a., December, 2017). Certifications. Retrieved from http://www.vitaljacket.com
- Birkett, M. A. (2011). The Trier Social Stress Test Protocol for Inducing Psychological Stress. Journal of Visualized Experiments : JoVE(56), 3238. doi:10.3791/3238
- Cannon, W. B. (1935). Stress and strains of homeostasis. American Journal of Medical Science, 189, 1-14.
- Cartwright, S., & Cooper, C. L. (1997). Managing workplace stress (Vol. 1): Sage.
- Castaldo, R., Melillo, P., Bracale, U., Caserta, M., Triassi, M., & Pecchia, L. (2015). Acute mental stress assessment via short term HRV analysis in healthy adults: A systematic review with meta-analysis. Biomedical Signal Processing and Control, 18, 370-377. doi:http://dx.doi.org/10.1016/j.bspc.2015.02.012
- Clifford, G. D., Azuaje, F., & McSharry, P. (2006). Advanced methods and tools for ECG data analysis: Artech house Norwood, MA.
- Cunha, J. P. S. (2012). pHealth and Wearable Technologies: a permanent challenge. In I. Press (Ed.), Studies in Health Technology and Informatics (pp. 185-195).
- Cunha, J. P. S., Cunha, B., Pereira, A. S., Xavier, W., Ferreira, N., & Meireles, L. (2010). VitalJacket: A wearable wireless vital signs monitor for patients' mobility in cardiology and sports. Paper presented at the 4th International Conference on Pervasive Computing Technologies for Healthcare, 22-25 March, Munich, Germany.
- Föhr, T., Tolvanen, A., Myllymäki, T., Järvelä‐Reijonen, E., Peuhkuri, K., Rantala, S., . . . Ermes, M. (2017). Physical activity, heart rate variability–based stress and recovery, and subjective stress during a 9‐month study period. Scandinavian journal of medicine & science in sports, 27(6), 612-621.
- Frisch, J. U., Häusser, J. A., & Mojzisch, A. (2015). The Trier Social Stress Test as a paradigm to study how people respond to threat in social interactions. Frontiers in psychology, 6, 14.
- Ganster, D. C., & Rosen, C. C. (2013). Work Stress and Employee Health:A Multidisciplinary Review. Journal of Management, 39(5), 1085-1122. doi:10.1177/0149206313475815
- Gordan, R., Gwathmey, J. K., & Xie, L.-H. (2015). Autonomic and endocrine control of cardiovascular function. World Journal of Cardiology, 7(4), 204-214. doi:10.4330/wjc.v7.i4.204
- Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. (1996). Circulation, 93(5), 1043-1065.
- Hickman, M. J., Fricas, J., Strom, K. J., & Pope, M. W. (2011). Mapping Police Stress. Police Quarterly, 14(3), 227-250. doi:10.1177/1098611111413991
- Jou, R.-C., Kuo, C-W., Tang, M-L. (2013). A study of job stress and turnover tendency among air traffic controllers: The mediating effects of job satisfaction. Transportation Research Part E. doi:http://dx.doi.org/10.1016/j.tre.2013.01.009
- Kaur, S., Bhalla, P., Bajaj, S. K., Sanya, S., & Babbar, R. (2013). Effect of physical and mental stress on heart rate variability in type-A and type-B personalities. Indian Journal of Applied Basic Medical Sciences, 15(20), 1-13.
- Kirschbaum, C., Pirke, K.-M., & Hellhammer, D. H. (1993). The ‘Trier Social Stress Test’–a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology, 28(1-2), 76-81.
- Kudielka, B. M., Hellhammer, D. H., Kirschbaum, C., Harmon-Jones, E., & Winkielman, P. (2007). Ten years of research with the Trier Social Stress Test—revisited. Social neuroscience: Integrating biological and psychological explanations of social behavior, 56, 83.
- Lazarus R.S., F., S. (1984). Stress, coping and adaptation. New York: Springer.
- Lomb, N. R. (1976). Least-squares frequency analysis of unequally spaced data. Astrophysics and Space Science, 39, 447-462. doi:10.1007/BF00648343
- Marteau, T. M., & Bekker, H. (1992). The development of a six-item short-form of the state scale of the Spielberger State-Trait Anxiety Inventory (STAI). Br J Clin Psychol, 31 ( Pt 3), 301-306.
- McLeod, J. (2011). Coping with work stress: A review and critique. Counselling and Psychotherapy Research, 11(3), 243-244.
- Olver, J. S., Pinney, M., Maruff, P., & Norman, T. R. (2015). Impairments of spatial working memory and attention following acute psychosocial stress. Stress Health, 31(2), 115-123. doi:10.1002/smi.2533
- Pallant, J. (2013). SPSS survival manual: McGraw-Hill Education (UK).
- Pan, J., & Tompkins, W. J. (1985). A real-time QRS detection algorithm. IEEE Trans Biomed Eng, 32(3), 230-236. doi:10.1109/tbme.1985.325532
- Pereira, T., Almeida, P. R., Cunha, J. P. S., & Aguiar, A. (2017). Heart rate variability metrics for fine-grained stress level assessment. Comput Methods Programs Biomed, 148, 71-80. doi:10.1016/j.cmpb.2017.06.018
- Perrin, M. A., DiGrande, L., Wheeler, K., Thorpe, L., Farfel, M., & Brackbill, R. (2007). Differences in PTSD prevalence and associated risk factors among World Trade Center disaster rescue and recovery workers. American Journal of Psychiatry, 164(9), 1385-1394.
- Rodrigues, S., Kaiseler, M., & Queirós, C. (2015). Psychophysiological Assessment of Stress Under Ecological Settings. European Psychologist, 20(3), 204-226. doi:10.1027/1016-9040/a000222
- Schaufeli, W., & Enzmann, D. (1998). The burnout companion to study and practice: A critical analysis: CRC press.
- Schnall, P. L., Dobson, M., & Landsbergis, P. (2016). Globalization, work, and cardiovascular disease. International Journal of Health Services, 46(4), 656-692.
- Shaffer, F., McCraty, R., & Zerr, C. L. (2014). A healthy heart is not a metronome: an integrative review of the heart's anatomy and heart rate variability. Frontiers in psychology, 5, 1040. doi:10.3389/fpsyg.2014.01040
- Smith, M. J., Karsh, B.-T., Carayon, P., & Conway, F. T. (2003). Controlling occupational safety and health hazards.
- Taelman, J., Vandeput, S., Spaepen, A., & Van Huffel, S. (2009). Influence of Mental Stress on Heart Rate and Heart Rate Variability, Berlin, Heidelberg.
- Tharion, E., Parthasarathy, S., & Neelakantan, N. (2009). Short-term heart rate variability measures in students during examinations. Natl Med J India, 22(2), 63-66.
- Thayer, J. F., Ahs, F., Fredrikson, M., Sollers, J. J., & Wager, T. D. (2012). A meta-analysis of heart rate variability and neuroimaging studies: implications for heart rate variability as a marker of stress and health. Neurosci Biobehav Rev, 36(2), 747-756. doi:10.1016/j.neubiorev.2011.11.009
- Voss, A., Schroeder, R., Heitmann, A., Peters, A., & Perz, S. (2015). Short-term heart rate variability—influence of gender and age in healthy subjects. PloS one, 10(3), e0118308.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
19 November 2018
Article Doi
eBook ISBN
978-1-80296-047-1
Publisher
Future Academy
Volume
48
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-286
Subjects
Health, psychology, health psychology, health systems, health services, social issues, teenager, children's health, teenager health
Cite this article as:
Rodrigues, S., Paiva, J. S., Dias, D., Pereira, T., & Silva Cunha, J. P. (2018). Acute Psychophysiological Responses To Laboratory-Induced Stress In Different Groups: An Exploratory Study. In Z. Bekirogullari, M. Y. Minas, R. X. Thambusamy, & C. Albuquerque (Eds.), Health and Health Psychology - icH&Hpsy 2018, vol 48. European Proceedings of Social and Behavioural Sciences (pp. 71-80). Future Academy. https://doi.org/10.15405/epsbs.2018.11.8