
Biomechanical control-based locomotor function rehabilitation technology for children with cerebral palsy


Abstract
Locomotor functions of children with special needs by the example of infantile cerebral palsy have been studied. The interaction with the support of children with special needs has been examined. It has been proved that during the jump of children of the main group there was an increase in pressure on the support relatively the lateral direction during the repulsion phase, they required more time to perform the initial phase of the jump due to the involvement of additional compensatory mechanisms to ensure the stability when landing. Thus, special attention should be given to the improvement of their coordination abilities and removal of muscle hypertonus. During physical exercises, it is recommended to focus on stretching and to enhance power quality of lower extremities. This approach will improve their motor adaptation. Moreover, the regional hemodynamics reaction to locomotor load among children with special needs has been assessed. It has been shown that children of the main group have a specific functional reserve of regional blood flow in proximal lower extremities. After locomotor load in the main group, there was an increase of pulse blood filling and blood flow velocity in hips, whereas the vegetative maintenance of distal extremities was decreased, which caused venous outflow. It enables us to recommend loading of hip muscles and unloading of shin muscles while forming locomotion adaptive stereotypes.
Keywords: Childrenhealthpeople with special needscerebral palsybiomechanicscomputer tensodynamographyrheovasography
Introduction
Modern society has fundamentally changed the views on problem of people with special needs. The concept of disability, which implies the existence of physical or psychological defects and, as a consequence, the need for rehabilitation, is being replaced by the concept of "special people" which is also widely used in Russian scientific papers. Such shift concerns not only a terminological change, but also an inner transformation of the approach to the problem and its solutions. People with special needs (PSN) – the definition recorded in Russian legislation – within this paradigm are treated as full members of society (Platt, 2016). Herewith, the task of society is not to expand the range of health and social services for these people, but to facilitate their full adaptation and inclusion in all spheres of public life with overcoming both social and physical barriers (Summa, & Vannozz, 2016).
At the present stage, this approach is mainly implemented in the social and psychological field. From the physical point of view, these people are still considered as patients in need of special medical attention. This contradiction is a considerable barrier to the full integration of people with special needs in society, especially in childhood. It is necessary to extend the integrated approach to the physiological aspects. The theory of functional systems represents a promising way towards it (Wang, & Huang, 2016).
The theory of functional systems was put forward by P. K Anokhin as a result of his research of mechanisms, compensating body dysfunctions. The research has shown that the compensation of dysfunctions can occur only during mobilization of the significant number of physiological components, which are mostly located in different parts of the central nervous system and periphery, but functionally integrated to result in an adaptive effect (Geisser, 2015). This functional integrative unity of differently distributed structures and processes of the adaptive effect was described as «functional system» (Anokhin, 1968). Adaptive effect is the quintessence of the functional system. It determines the composition, the rearrangement of efferent excitations and the inevitable reverse afferentation of the intermediate of the final adaptive effect (Davletjarova, & Kapilevich, 2016).
One of the main physiological constituents of the normal formation and development of child’s organism is movement. Movement contributes to the development of all cortex areas, coordination of intracentral connections, compensation and correction of physical and mental deficiencies, formation of locomotor interactions of analyzer systems and cognitive processes (Bredikhina, & Baranova, 2015). Movement maintains the efficiency of the organism and is necessary for its life support. Accordingly, formation of motor skills in children with special needs is an essential part of their adaptation. At the same time, it is important to focus primarily on the mobilization of their own compensatory mechanisms that can be implemented by examining physiological characteristics of the locomotor adaptation (Mawase, & Bar-Haim, 2016).
Specific movement patterns of these children may serve the basis for the formation of new movement skills, which will lead to a better ability to move. However, the development of adaptation techniques should be based on physiologically sound principles and with the consideration of the functional state of nervous and musculoskeletal systems and vegetative support mechanisms (Davlet'yarova, & Korshunov, 2015).
As we have mentioned above, the integrative approach is implemented more successfully when the focus is on socio-psychological adaptation of children with special needs. Some authors see the solution of this problem in the neurophysiological aspect and consider locomotor activity as a means of socialization and psycho-physiological adaptation, as well as education (Marret, & Vanhulle, 2013). The effectiveness of this approach is assessed using the theory of functional systems, which considers effective adaptation as the successful integration of a child with special needs in society through the rational use of his existing skills and the mobilization of compensatory mechanisms, rather than the rehabilitation of a function up to the level of physiological norm (Imms, 2008).
In this respect, the aim of the research was to study the physiological differences of the motor adaptation of children with special needs associated with limited mobility.
Research objectives
-
To study the nature of the interaction with the support among children with special needs.
-
To assess the regional hemodynamics reaction on locomotor load among children with special needs.
Locomotor functions of children with disabilities were studied using an example of infantile cerebral palsy. Cerebral palsy is a group of permanent disorders, associated with the development of movement, resulting in the restricted mobility.
Subject of research
The study involved 90 children aged between 8 and 12 years (average age 10,37 ± 1.74 years), including 54 boys and 36 girls.
The main group consisted of 60 children (36 boys and 24 girls) with special needs.
The control group consisted of 30 children (18 boys and 12 girls) without any special needs.
Materials and methods
The study was conducted at State-Funded Regional Institution «Rehabilitation Center for children and adolescents with disabilities» (Closed Administrative-Territorial Unit, Seversk).
A set of non-invasive physiological research methods was used:
Computer tensodynamography
Rheovasography
Nature of the interaction with the support among children with special needs was studied using a method of computer tensodynamography. To implement this method, the force platform was used. A force platform is a multicomponent force plate with an aluminum protective panel for measuring support reaction forces, the moment and the center of pressure during the jump and coordination analysis. Force platform detects pressure points on the whole surface and provides a detailed information about footwork - weight distribution, lifting and rotation. This technology allows a high accuracy diagnosis of various pathologies of the musculoskeletal system and a targeted correction and optimization of movement patterns. The obvious advantage of this method is reflected in the absence of test devices on the body of the person under test, which can restrict his free movement. Using a motion capture system allows obtaining objective and accurate quantitative data and display the results of research in a user-friendly form.
The study of blood flow was based on rheovasography using a «Rheo-Spectrum» rheograph (SPA Neurosoft, Ivanovo, Russia).
The rheogram was recorded at rest and after locomotor load in the part «Hip-shin» of the left and right lower extremity simultaneously. The first electrode was applied to the area of the upper third of hip, the second electrode - below the kneecap under the tibia lump at the level of a minimum diameter of the shin, and the third electrode was fixed on the lower part of the shin at the level of the smallest diameter. During the study of regional hemodynamics, the rheogram, which presents a curve reflecting the pulse oscillation of electrical resistance, was recorded. During the increase in blood filling, there was a rise of the curve amplitude and vice versa, which means the recording of the impedance dynamics in the reverse polarity. Rheogram shows systolic and diastolic parts. The first is due to the blood flow, the second is associated with the venous outflow.
Factual data are presented in the form of «mean ± error» (М±m). The significance of differences between the groups was assessed using a nonparametric Mann-Whitney.
Results and discussion
To investigate the nature of the interaction with the support, children with disabilities were invited to jump onto the force platform, on the force platform and from the force platform.
During the jump onto the force platform, it was observed that the repulsion of children of the main group is characterized by the presence of a permanent initial angle in joints, which means a higher phase of active repulsion. That is confirmed by the research data which indicate that the minimum value of vertical force Fz in the main group during repulsion is significantly higher than 2.5 H, against the control group with the value of -0.5 H. A horizontal force value, directed towards the movement in landing phase Fx, is significantly higher than that in the control group. Besides, the force directed towards lateral sides Fy, is 2.5 times higher than that in the main group. Thus, horizontal forces in the main group were significantly lower during the jump in the landing phase due to impaired motor coordination, spontaneous locomotion, synkineses etc.
The maximum value of vertical force F in the main group is less than 806. 4 H. This is because during acceleration of mobile units, the effect of retarding gravity forces and inertia of other mobile units, resistance forces of agonist muscles, as well as muscle hypertonus of lower extremities are observed. The value of horizontal force Fx directed towards the movement in the landing phase is not significantly higher than the value of the control group – 43.9 H. the horizontal force directed to lateral sides Fy is higher in the main group – 40.7 H, because total CG projection during weight bearing when landing is asymmetrical due to contractures and muscular spasticity.
The time spent for the minimal effort in the main group is significantly lower, than in the control group, due to the absence of the amortization phase. According to EMG of the lower extremities, muscular activity in the main group was significantly higher than in the control group; thus, the time spent for the maximum effort was also shown to be less.
Research has concluded that children with special needs apply more effort when performing a jump, but the maximum value of the jump force in the control group was significantly higher. Moreover, in the main group, there was the increase in the pressure on a support to the lateral side on the Fy axis.
The study of time values revealed a quicker reaction of the main group during the initial phase of the jump. Children in the main group applied maximal efforts, but demonstrated a lower maximal force of the jump.
The study of the jump on the force platform has shown that the minimum value of vertical force Fz in the main group is significantly lower -178.63H. This is explained by the fact that during acceleration, the locomotion of mobile units is affected by retarding forces (gravity and inertia). Values of the horizontal force directed towards movement Fx are significantly lower than those in the control group as the children of the control group have a preconditioned more rapid muscle contraction during the light work mode, which is not typical for the main group.
The force directed to lateral sides Fy is higher in the main group with the value of -60.50H. This is due to the fact that in the control group, total CG returns to the right position after the flight phase more rapidly, which is not typical for the main group because total CG is outside the normal range.
The maximum value of vertical force Fz in the main group is significantly higher than 768.90H because on the background of spasticity, synkinesis etc., they apply more effort during the flight phase. The maximum values of the horizontal force, directed towards movement Fx, are significantly lower in the main group as there are no preconditions for fast contraction of gastrocnemius muscles.
The first time value on both Fy and Fx axes accords with minimal efforts. Time in the direction of the Fz axis in the main group is significantly higher due to the influence of unconscious locomotion and coordination of movement in the flight phase.
The ratio of the second time value and maximal effort on axes Fz and Fy is correct. The horizontal effort to the locomotion side and the time, spent for the jump on the force platform in the main group, is significantly higher. More time was spent in the main group due to its slow phase of active repulsion.
Basing on the research conducted, we may conclude that during the jump on the force platform in the main group, it was revealed that the increase in force on vertical axis Fz, which is due to the involvement of additional compensatory mechanisms to ensure the stability when landing.
The study of time values revealed that the children of the main group are slower in reaching a maximum force action on the platform but faster in performing a minimal effort.
Investigation of the jump from the force platform has shown that the minimal values on the Fx axis to the side of movement are significantly higher in the main group due to the impaired standing pose, which is linked with the change in total CG. The study of axis Fy gave no significant differences. The minimum value of vertical force Fz is significantly lower in the main group due to motor problems in knee joints of flexion contractures.
Placing reaction, which balances internal forces (muscle forces), plays an important role in the repulsion mechanism. Placing reaction of the main group is instable, thus, more forces were applied to the side of movement on the Fx axis.
Children of the main group apply more effort due to the predominance of muscle spasticity, which results in lateral ataxia and in a change in normal limits of total CG.
Locomotion of vertical forces in the main group is slower due to the cushioning flexion of hip, knee and ankle joints. For this reason, they cannot reach the maximum force during the repulsive phase.
The study of time values for minimal forces on axes Fy and Fx gave no significant differences between groups. In the vertical direction, the minimum force of a jump in the main group is significantly higher due to an increased phase of the support on toes.
The recording of the second time value gave no significant differences between groups during the repulsion from the platform.
Basing on the research conducted, we may conclude that in the main group during the initial phase of the jump from the platform, there was an increase in the pressure on the support in the vertical direction of the Fz axis. During the repulsion from the platform, there was an increase in the pressure on the support in horizontal and lateral directions and a decrease in the vertical direction of the Fz axis. In addition, children with special needs require more time to complete the initial phase of the jump, as compared with the control group.
Thus, particular attention should be given to the development of their coordination abilities and removal of muscle hypertonus with the focus on stretching and power quality of lower extremities. This approach will improve their motor adaptation.
Vegetative maintenance by the circulatory system is an important component of physiological regulation of locomotion. Efficiency of oxygen supply to muscles in necessary quantity and disposal of waste products largely determine locomotor acts. Rearrangement of the vegetative maintenance system is very important for adaptation to various conditions, including motoric disorders, diseases of the musculoskeletal system. Moreover, rearrangement of this system is not linear, as different mechanisms can be involved at different stages. Locomotor skill development of children with special needs should be implemented with the consideration of functional reserves of the regional blood flow in lower extremities.
To assess hemodynamic changes in lower extremities, a rheographic complex «Rheo-Spectrum-2» of LLC «Neurosoft» was used. Rheographic index (RI), Frequency Response Index (FRI), rapid blood filling index (Vmax), slow blood filling index (Vavg), diastolic index (DSI), dicrotic index (DCI), venous outflow (VO) were assessed. Rheography of lower extremities was performed before and after a 10 minute walk on the electric treadmill (at a speed of 1 km/h).
It was shown that in the main group the pulse blood filling was 3 times higher in the left hip (Figure
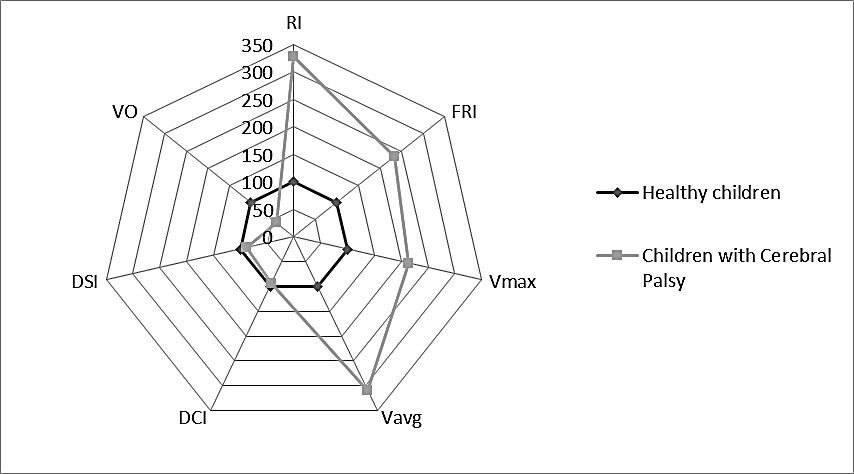
The study of pulse blood filling values in shins at rest gave no valid differences between groups.
After locomotor load, pulse blood filling in the main group increased moderately in the right and left hip in comparison with the control group.
In the control group, physical activity resulted in a significant increase in both shins, whereas in the main group this parameter was decreased. The results indicate that during physical activity, children with special needs have an increase in pulse blood filling mainly in hips, while healthy children in shins. It is also worth noting that in the main group, blood filling strives to achieve the same values between the left and the right hip after locomotor load.
At rest children of the main group have an increased FRI in the left hip, which is 2 times higher than target values, compared to FRI in the right hip, which are 1.5 times lower (Figure
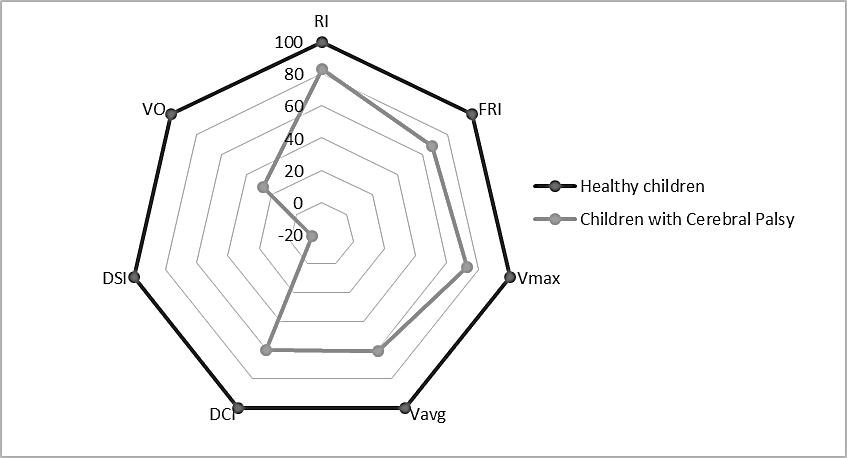
After locomotor load, an FRI decrease in hips and an FRI increase in shins are observed in the control group. In the main group, FRI in shins is significantly decreased in comparison with target values. Thus, the locomotor load positively affects children with disabilities (with support or without support), which leads to the equilibrium of FRI.
At rest, blood flow in large bore arterial vessels in the main group (with support and without support) was 2 times higher in the left hip and 1.5 times lower in the right hip in comparison with the control group. In the main group, blood flow in the left hip was 3 times higher, compared to the right hip. Studying shins gave no principal differences.
After the load, velocity in hips substantially increases in both groups (particularly on the right), while the velocity increase in shins is recorded only in the control group.
At rest, blood flow in small and medium bore arterial vessels in the main group (with and without support) in the left hip was 3 times higher and 1.5 times lower in the right hip compared with the control group. If compare the left and the right hip in the main group, the velocity increases by 5 times. Studying shins gave no principal differences.
After the physical exercise, velocity in shins among children of the main group (with support and without support) has slightly increased, whereas in the control group, the increase was more significant (especially on the right). After exercises, the velocity in shins of the main group (with or without a support) has slightly increased, whereas the significant increase was pronounced in the control group (particularly on the right).
At rest, peripheral vascular resistance (measured in DCI) in the right and left hip was moderately decreased in the main group compared to the control group, and increased in the shin on the right and on the left.
After the load in both groups (with support and without support), DCI decreased in the right and left hips. After the load in the control group, there was an increase of DCI in shins, whereas in the main group, there was an increase in the right shin.
Diastolic and venous outflow indexes, characterizing condition of the venous sector, are significantly lower in the main group (with support and without support), compared to the control group. In the main group, DSI and VO were significantly higher in the left hip compared to the right one.
After the locomotor load, DSI in both groups increases in hips, but in the main group, VO remains significantly higher. The difficulty of venous outflow in shins is recorded after the physical exercise in both groups, but is more pronounced in the main group.
Conclusion
The study of interaction with the support among children with disabilities has revealed that in the development of rehabilitation programs, special attention should be given to the improvement of their coordination abilities and removal of muscle hypertonus. During physical exercises, it is recommended to focus on stretching, to enhance power quality of lower extremities. This approach will improve their motor adaptation.
Hemodynamic disorders of the main group, revealed in the study of hemodynamic values, are most likely due to lower level of physical activity (hypokinesia). The results show, that children with disabilities have dysfunction of the peripheral part of the circulatory system in lower extremities. At rest, it is expressed mainly in hips and revealed by increased pulse blood filling and blood flow and their asymmetry, combined with the decrease in venous outflow. After locomotor load in the main group, there is an increase of pulse blood filling, blood flow and its velocity in hips, whereas healthy children have an increase in shins. Children with disabilities have also problems with the venous outflow on the background of locomotion.
Thus, children with special needs have a decreased vegetative maintenance mostly in distal extremities; in proximal extremities, there exists a specific functional reserve. It enables us to recommend loading hip muscles and unloading shin muscles while forming locomotion adaptive stereotypes.
Acknowledgement
This research was conducted owing to the grant, issued by the Russian Science Fund (Project No. 16-18-00016).
References
- Bredikhina, Y. P., Baranova, E.A. & Kabachkova, A.V. (2015). Balance and steadiness correction of the upright posture of patients having withstood an ischemic stroke with the help of stabilographic rehabilitation training equipment with biofeedback. SHS Web of Conferences, 28. 01017.
- Davletjarova, K.V., Kapilevich, L.V & Ovchinnikova, N.A. (2016). Life Quality Increase Using Locomotion in Students with Disabilities. SHS Web of Conferences 28, 01024.
- Davlet'yarova, K. V., Korshunov, S. D. & Kapilevich, L. V. (2015). Biomechanical Bases of Rehabilitation of Children with Cerebral Palsy. AIP Conference Proceedings. 1688, Article number 030015, 1-5.
- Geisser, M.E. (2015). Тhe Journal of Pain, 6(11).
- Imms, C. (2008). Disabil. Rehabil. 11/30; 30(24), 1867–1884.
- Marret, S., Vanhulle, C.& Laquerriere, A. (2013). Handb Clin Neurol. 111,169-76.
- Mawase, F, Bar-Haim, S, Joubran, K, Rubin, L, Karniel, A & Shmuelof, L (2016). Increased Adaptation Rates and Reduction in Trial-by-Trial Variability in Subjects with Cerebral Palsy Following a Multi-session Locomotor Adaptation Training. Front Hum Neurosci. 10: 203.
- Platt, M.J. (2016). Counting cases of cerebral palsy. Dev Med Child Neurol.
- Summa, A, Vannozz, G, Bergamini, E, Iosa, M, Morelli, D & Cappozzo, A (2016). Multilevel Upper Body Movement Control during Gait in Children with Cerebral Palsy. PLoS One. 11(3): e0151792.
- Wang, TM, Huang, HP, Li, JD, Hong, SW, Lo, WC & Lu, TW. (2016). Leg and Joint Stiffness in Children with Spastic Diplegic Cerebral Palsy during Level Walking. PLoS One; 10(12): e0143967.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
20 July 2017
Article Doi
eBook ISBN
978-1-80296-025-9
Publisher
Future Academy
Volume
26
Print ISBN (optional)
Edition Number
1st Edition
Pages
1-1055
Subjects
Business, public relations, innovation, competition
Cite this article as:
Davlet’yarova, K., Kapilevich, L., Korshunov, S., & Ovchinnikova, N. (2017). Biomechanical control-based locomotor function rehabilitation technology for children with cerebral palsy. In K. Anna Yurevna, A. Igor Borisovich, W. Martin de Jong, & M. Nikita Vladimirovich (Eds.), Responsible Research and Innovation, vol 26. European Proceedings of Social and Behavioural Sciences (pp. 183-191). Future Academy. https://doi.org/10.15405/epsbs.2017.07.02.24