
Cardiovascular Health and Physical Capacity in Student and Elite Basketball Players


Abstract
Taking into account the features of contemporary approach to trainings in team sports, and basketball in particular, issues of cardiovascular health are under consideration. The purpose of the study was to evaluate health issues and physical capacity of amateur high school and professional basketball players in order to prescribe exercise programs to increase their athletic performance without medical risks. The study involved two groups of basketball players of different levels – student team of UrFU (n = 11, age 19,55 ± 1,57 years) and the professional club team of Sverdlovsk region (n = 12, age 24,17 ± 4,76 years). Methods: multifrequency bio-impedance analysis of body composition, 12-lead ECG, the hemodynamic monitoring during the orthostatic and сlinostatic tests), and cycle exercise testing (ET) with heart rate monitoring and gas-exchange measurement, statistical analysis. Findings: despite the observed normal physical status of subjects, disorders of cardiovascular adaptation were found. The research revealed the insufficient hemodynamic indices (SI & EDI) in students, that lead to higher HR at rest and during ET regardless of the level of intensity. Professional basketball players demonstrated higher ET results (AT = 83.5±6.77 %, Pmax = 381.5 ± 41.44 W, VE=141.4±38.14) in comparison to students (73.7±8.93%, = 317.09 ± 49.18 W and 115.8±31.9 accordingly). So the development of the cardiovascular system must be the first priority for healthsaving even in basketball, which is basically not considered as endurance sport.
Keywords: Basketball playersathletes’ healthcardiovascular systemhemodynamicsphysical capacity
Introduction
Basketball is a very challenging sport. The success of the game depends on a number of physical and psychological abilities: strength, coordination, general and special endurance, technical competence, psychological stability, etc. Whereas physical inactivity leads to cardiovascular diseases and health issues (Chandra et al. 2013; Corrado et al. 2005; Mekhdieva et al. 2015), can we esteem an athlete trying to improve their performance in sports as a healthy person? Intense training and the strain of competition may affect the athletes’ health, especially, when athletes are physically underdeveloped (Mann, 2013).
Thus the aim of the research was to evaluate health issues and physical capacity of amateur high school and professional basketball players in order to suggest exercise programs to increase their athletic performance without medical risks.
Research methods
Twenty-three young healthy sportsmen were recruited for the study. The first group was distributed by elite basketball players (n = 12) of professional team “Uralmash” (Yekaterinburg, Russia), the second – by high performance student team of Ural Federal University (Yekaterinburg, Russia), members of International Student Basketball League and the main leaders of Student Basketball Association. All participants were informed of the purpose of the research, methods and any possible risks, before their written consent was obtained. The study design had been previously approved by The Ural Federal University Ethics Committee. Testing was carried out in the laboratory "Technologies of recovery and selection in sport" at Ural federal university, Russia. The schedule of investigations matched the training period of athletes and was conducted after 24 hours of recovery from the previous training. Athletes’ examination in both groups started from personal and family history data collection of cardiovascular diseases. Physical examination was based on anthropometric measurements (Table.
The cardiovascular examination included 12-lead resting ECG registration with professional electrocardiograph Schiller AG AT-104 (Schiller AG, Switzerland), followed by interpretation of the results in line with international standards (ACC / AHA 2002 Guidelines) and hemodynamic monitoring during active orthostatic test.
The hemodynamic monitor of anesthetists and reanimatologist MARG 10-01 "Microlux" (Cheliabinsk, Russia) operation is based on such noninvasive methods of hemodynamic monitoring as impedance cardiography and spectrophotometry, electrocardiogram monitoring (ECG), pulse oximetry monitoring, reography and central hemodynamics monitoring, blood pressure and temperature. Thus monitor provides the researcher with the a whole range of important sport-relevant parameters such as the heart and breathing rate, the stroke and end-diastolic volume, ejection fraction, the vascular tone and etc.
To evaluate the aerobic capacity of athletes, the stress-system Schiller AG Cardiovit AT-104 (Schiller AG, Switzerland) was used. Each subject performed cycle exercise testing (ET). The maximal ramp ET protocol was developed according to ACC/AHA 2002 guideline update for exercise testing (2006) to estimate peculiarities of cardiovascular adaptation to increasing exercise loads. Maximum oxygen uptake (VO2max) as a measure of aerobic capacity was determined by indirect calorimetry with the use of portable desktop metabolic system FitmatePro (COSMED, Italy). After a 1 min warm-up, subjects started at zero load, continuously increasing by 40 W per minute and were maintaining the pedaling frequency of 80 cycles per minute until volitional exhaustion in order to determine HRmax, VO2max, maximum attained load (Pmax), minute ventilation (VEmax, l/min), anaerobic threshold (AT). Heart rate monitoring was carried out simultaneously with Garmin Forerunner 305 (Garmin, USA) during the test and the following 3 minutes of post-exercise recovery period.
The statistic software package “SPSS Statistics 17.0” (IBM) was used for statistical analysis. Mean value (M) and standard deviation (SD) for the used parameters were calculated, t-test was applied for comparative analysis. The level of significance was set at P < 0.05.
Findings
Results of physical examination of athletes are distributed in Table
One can see that generally, anthropometric parameters corresponded to the athletic physiologic norm. Although, major indices varied within a certain range in both groups, there no significant differences between values of BMI, fat free mass, leg lean mass and percentage of fat in groups of professionals and student-athletes. Thus, body composition of studied athletes irrespective of their professional level was comparable.
According to investigation of personal and family history of athletes, no positive data of previous cardiovascular events or chronic disease in both groups were obtained. Analysis of 12-lead resting ECG observations showed no pathologic changes in all studied subjects. Major ECG changes were considered as training related normal variants in reference to refined criteria (Sheikh, 2014). These findings were as follows in all studied athletes: sinus bradycardia (17 % of all studied subjects; n = 4), incomplete RBBB (30 %; n = 7), early repolarization (65%; n = 15). Moreover, no training unrelated ECG changes (P-wave, QRS or QT-interval changes, the rhythm or conduction abnormalities etc.) were defined.
Thus, in most cases the decrease of HR was observed (less than 60 beats per minute), which indicated the physiological adaptation of the heart to physical stress and corresponded to the adequate reaction of the cardiovascular system. In all cases mentioned above, at the time of the survey, there were no clinically significant arrhythmias and conduction abnormalities, which confirms the normal functional condition of the heart based on the ECG data. All registered ECG changes (ST-segment changes, the T-wave (amplitude increase) in the chest leads) were considered as the consequence of the normal heart reaction to intense long-term physical activity (over 5 years).
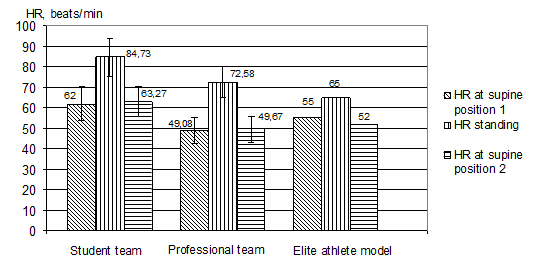
Hemodynamic monitoring during orthoclinostatic test (supine position1 – standing – supine position2) allowed to evaluate the cardiovascular health of the subjects (Shishkina, 2014). The most informative indicators of athletes hemodynamics were selected for observation (table
The heart rate at rest (RHR) in professional basketball players corresponded to that of high performance endurance sport representatives whereas RHR in students were normal for healthy people in supine. During active orthostatic test, an HR increase after transition from supine to the vertical body position must be less than 18 in ordinary people and 10 in advanced athlete as it is demonstrated by the elite athlete model in fig.
The correlation rhythmogram is a set of points which have coordinates defined by two adjacent cardiointervals values RRi and RRi+1 (fig.
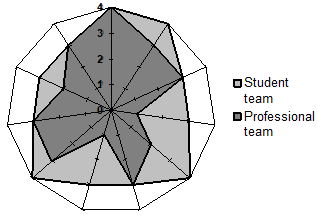
Radar chart of correlation rhythmogram distribution among the basketball student team and professional club players is displayed with athletes represented on axis (spokes). The data length of a spoke is proportional to the rhythmogram rank (table
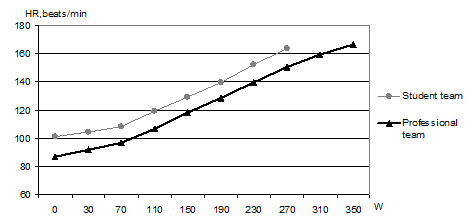
Heart rate monitoring during ET (fig.
The higher values of HR in students than that in professional basketball players at the similar pedaling power regardless the physical load intensity. Insufficient development of athletes’ cardiovascular system and low hemodynamic indices of students basketball players (table
2 ) causes the higher HR during any physical activity than in endurance athletes.The greater average values of attained load (Pmax, W) in professional team Pmax = 381.5 ± 41.44 W in comparison with students’ Pmax= 317.09 ± 49.18 W.
The longer trajectory of professional basketball players than that of students. It is due to better strength abilities and overall endurance of professional players than that in student team.
Athletes of both teams refused to continue ET or were stopped by the researcher because of their inability to maintain the necessary pedaling rate at moderate HR (below 180 bpm). In maximal stress-test, HRmax lower than 180 bpm, which serves an indicator of the priority in the cardiovascular fitness over muscles.
Gas-exchange measurements during ET allowed us to compare major indicators of aerobic performance between athletes depending on qualification. Fig.
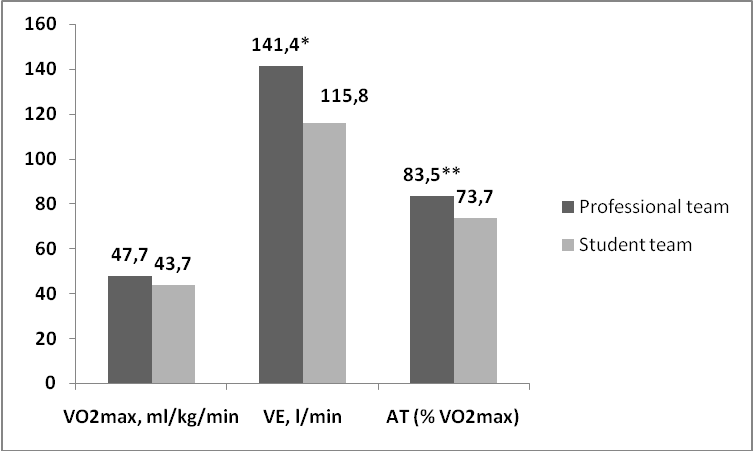
VO2max – maximum oxygen uptake; VE – minute ventilation; AT – anaerobic threshold; * statistical significance at P < 0.05 and **P < 0.01.
Maximum oxygen uptake (VO2max) is an indicator of maximal aeropic capacity (Bassett, 1997), pointing at the athletes’ ability to transport oxygen to working muscles as well as to utilize it with this skeletal muscles at maximum load. Thus, VO2max affected by overall endurance factors (cardiovascular and respiratory systems) and Pmax affected by strength factors are the main characteristics of an athlete’s integral readiness. The following recommendation for student basketball team was developed: at first it was necessary to provide sufficient SV and end-diastolic volume in athletes, then enhance their strength. As the professional team players had sufficient heart volume parameters and thereby low RHR, appropriative HR dynamics during ET and the HRmax below 180 bmp, the evident way for them to improve performance is strength training.
Thus, analising the obtained data on the VO2max value with full details about cardiovascular health allowed us to determine the limiting factors of athlete’s performance and to explain the top-priority importance of cardiovascular development in training of basketball playersof any professional level.
Conclusions
The research of cardiovascular health in basketball-players allowed us to identify the absence of abnormalities in the cardiovascular system of athletes. Along with normal anthropometric and ECG parameters, the insufficient hemodynamic indices (SI and EDI) were revealed in students, especially in a vertical body position. These hemodynamic peculiarities caused the high HR during athletes’ training and competitive activity. So the development of cardiovascular system must be the first priority for healthsaving even in basketball, which is basically not considered as endurance sport.
Acknowledgements
The work was supported by Act 211, the Government of the Russian Federation, contract № 02.A03.21.0006
References
- ACC / AHA 2002 guideline update for exercise testing: summary article: a report of the American College of Cardiology / American Heart Association Task Force on Practice Gudelines (2006). J Am Coll Cardiol, 48, 1731 pp.
- Bassett, DR. J., & Howley, E.T. (1997). Maximal oxygen uptake: “classical” versus “contemporary” viewpoints. Med Sci Sports Exerc, 29(5), 591-603.
- Chandra, N., Bastiaenen, R., Papadaki ,M., & Sharma, S. (2013). Sudden Cardiac Death in Young Athletes. Practical Challenges and Diagnostic Dilemmas. J Am Coll Cardiol, 61(10), 1027-1040.
- Corrado, D., Pellicia, A., & Bjornstad, H.H. et al. (2005). Cardiovascular pre-participation screening of young competitive athletes for prevention of sudden death: proposal for a common European protocol. Eur Heart J, 26(5), 516-524.
- Mann, T., Lamberts, R.P., & Lambert, M.I. (2013). Methods of prescribing relative exercise intensity: physiological and practical considerations. Sports Med, 43(7), 613-25.
- Mekhdieva, K., Timokhina, V., Sokolov, S., & Blyakhman, F. (2015). Cardiac regional function of young sportsmen with false tendons in the left ventricle. J Mech Med Biol , 15(2), 1-6.
- Sheikh. N et al. (2014). Comparison of electrocardiographic criteria for the detection of cardiac abnormalities in elite black and white athletes. Circulation,129,1637–1649.
- Shishkina, A., Tarbeeva, N., Alimpieva, O., Berdnikova, A., Tarbeeva, A., & Miasnikova, T. (2014). Hemodynamics Monitoring in Sport – Using Hemodinamics Monitor for Sport Training Planning. icSPORTS 2014: In Proceedings of the 2nd International Congress on Sports Sciences Research and Technology Support, Rome, Italy: 103-110.
- Stickland, M.K., Welsh, R.C., &Petersen, S.R. (2006). Does fitness level modulate the cardiovascular response to exercise? In J Appl Physiol, 100, 1895-1901.
- Vilikus, Z. (2012). Functional Diagnostics. Col Phy Edu and Sport Palestra, 12-15.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
20 July 2017
Article Doi
eBook ISBN
978-1-80296-025-9
Publisher
Future Academy
Volume
26
Print ISBN (optional)
Edition Number
1st Edition
Pages
1-1055
Subjects
Business, public relations, innovation, competition
Cite this article as:
Zakharova, A., Mekhdieva, K., & Smirnov, V. (2017). Cardiovascular Health and Physical Capacity in Student and Elite Basketball Players. In K. Anna Yurevna, A. Igor Borisovich, W. Martin de Jong, & M. Nikita Vladimirovich (Eds.), Responsible Research and Innovation, vol 26. European Proceedings of Social and Behavioural Sciences (pp. 1032-1039). Future Academy. https://doi.org/10.15405/epsbs.2017.07.02.133