
Psychotherapy Intervention With Hypnosis In Patients With Type 1 Diabetes Mellitus


Abstract
Type 1 Diabetes
Keywords: PsychotherapyHypnosistype 1 diabetes mellitusglycemiaglycosylated haemoglobin
Introduction
Type 1 Diabetes
mortality risk (Ferreira, 2015). Psychological factors play a crucial role in this chronic disease (Gatchel &
Oordt, 2015). Thus, in addition to medical therapies and nutritional prescriptions, the intervention of the
psychologist is regarded as fundamental and constitutes an added value (Gatchel & Oordt, 2015).
However, in addition to interventions to increase diabetic patients adherence to treatments and lifestyle
changes, hypnotherapy may be an excellent complementary "therapeutic" tool (Trujillo, 2010).
However, given the scant investigation of the effectiveness of scientific clinical hypnosis in
T1DM, one might ask: do psychotherapy with analytical hypnosis coupled with Guided and Creative
Imagery (GCI) lower blood sugar levels?
Diabetes Mellitus
Diabetes
transformations on patients’ lifestyles (Rodrigues & Costa, 2013). It is characterized by chronic
hyperglycaemia and disruption of the metabolism of carbohydrates, fats and proteins (World Health
Organization, 2015). In Portugal, as in other developed countries, there is a true diabetes pandemic,
affecting more and more people and being recognized as a major cause of death (Rodrigues & Costa,
2013).
Type 1 Diabetes Mellitus
T1DM, or type 1 diabetes, also known as Insulin-Dependent Diabetes Mellitus, results from the
progressive selective autoimmune destruction of the beta cells of the pancreatic islets, triggering a
deficiency in the secretion of the hormone insulin produced by the pancreas (Rodrigues & Costa, 2013;
World Health Organization, 2015). T1DM represents 5% to 10% of all cases of diabetes and patients
require lifelong insulin injections to survive (World Health Organization, 2015).
The essential goals of diabetes treatment are the metabolic compensation or control and
consequent prevention of acute complications (hyperglycemia and hypoglycemia) and prevention or delay
in the development of chronic complications, which are respectively an immediate danger to the patient's
life and a slow and progressive threat to their health (Almeida, Ferrão, & Zangeronimo, 2013). Treatment
of T1DM requires a careful balance between diet, exercise and insulin injections as well as frequent self-
monitoring of blood glucose levels, self-care that tend to vary from patient to patient (Almeida et al.,
2013). Since T1DM effects inevitably have a substantial and negative impact on patients quality of life
(Ferreira, 2015), in addition to medical therapies and nutritional prescriptions, psychologist intervention
can be an advantage as far as diabetes treatment is concerned (Gatchel & Oordt, 2015).
Diabetes Mellitus, Psychology and Hypnosis
The most common psychological treatments of T1DM have been cognitive-behavioral in nature,
whose main objectives are the reduction of negative emotions and the increase in the perception of self-
efficacy, aspects considered essential for adherence to diabetes self-care and good glycemic control (Van
der Ven et al., 2005). In this sense, the increasing use of hypnosis as an adjuvant therapy in the
management of immunity, through the activation of the most powerful healer - the human mind (Trujillo,
2010). Hypnosis is one of the oldest non-medical treatments and a non-pharmacological medium, so it has
no adverse side effects or interactions, is cost-effective and can produce results in one session (Trujillo,
2010). In addition, this therapy is also a self-management tool, since self-hypnosis is easily taught and
tends to become an asset for life (Trujillo, 2010).
Hypnosis has been shown to be an effective method for the management of autoimmune diseases
such as rheumatoid arthritis (Trujillo, 2010), Osteoarthritis (Ferreira, Repolho, Ribeiro, & Sepodes,
2012), Multiple Sclerosis (Hosseinzadegan, Radfar, Shafiee-Kandjani, & Sheikh, 2017), fibromyalgia
(Picard et al., 2013) and lupus, asthma (Trujillo, 2010), and cancer (Roe et al., 2016).
Specifically in DM, are ancient studies with hypnosis has shown beneficial effects, notably in the
decrease of blood glucose levels and Glycosylated or Glycated Hemoglobin (HbA1c), in the spontaneous
reduction in their daily dose of insulin, in the metabolic control of diabetes, increased blood flow to the
extremities, and reduced diabetic foot problem, as well as the reduction of diabetes-related stress (Xu &
Cardeña, 2008). That is, hypnosis appears to be an adjunct to diabetes management and monitoring as
well as metabolic control (Xu & Cardeña, 2008).
The most recent definition of the American Psychological Association's Division 30 (Society of
Psychological Hypnosis) argues that
and reduced peripheral awareness, characterized by a strengthened ability to respond to suggestion"
(Elkins, Barabasz, Council, & Spiegel, 2015) and
of a medical act, disorder or psychological concern" (Elkins et al., 2015).
Given the relationships between behavior, psychosocial factors and the nervous, endocrine and
immune systems, with the emergence of diseases, Ader and Cohen (1975) developed the concept of
involvement of the neuroendocrine pathways in the immune responses –
to the multiple interrelationships between the organic systems involved in the process, it can also be
called Psychoneuroimmunoendocrinology (Ader & Cohen, 1975).
Thus, hypnosis seems to produce concrete and measurable positive changes in the immune
system, being this system fully open and operational from Theta waves (4-7 cycles per second (cps))
(Bastarache & Bastarache, 2014). According to the six levels of the
be noted that the simple eye-closure process releases approximately 80%
approximately 80% passes to the
most programming (Bastarache & Bastarache, 2014).
Guided and Creative Imagery
Since the mind does not distinguish a real image from that which is imagined (Rossi, 1995),
making it possible to perceive a non-existent object simply by believing in it. This is a process of
orienting thought patterns during the practice of the imagination, in which the mind, through thoughts,
images, beliefs, memories and emotions, can alter the biochemical structure of the nervous system and
induce the body to react to the mental image as if it were real, and this interaction is constant and
involuntary (Rossi, 1995).
Direct suggestion may affect a change in patient behavior and result in symptomatic cure, at least
temporarily (Rossi, 1993). However, "healing" is simply a response to suggestion and does not imply the
reassociation and reorganization of ideas, which are essential for real healing. It is this experience of
reassociation and reorganization of his own experiential life that enables healing (Rossi, 1993). Therefore,
relaxation and attention focused on the thoughts and ideas that can help a person achieve the desired
outcome in their life, highly enhances the chances of success (Petruzzi, 2016). With a strong motivating
desire change, the direct suggestions and post-hypnotic suggestions may be enough to provide a lasting
benefit to some clients during some of the time (Hunter & Eimer, 2012).
Suggestibility
Suggestibility refers to the way an individual learns and the means to which he/she is most
receptive to learning, which varies with the individual (Kappas, 2001). Hypnosis gets results when the
induction and suggestions made during the process are based on the client's suggestibility characteristics.
John Kappas (2001) determined that there are three types of suggestibility, or styles of learning /
communication: emotional, physical, and somnambulist.
The above mentioned types of suggestibility are equally valid, they only help to know the style
of processing and communication for a better relationship with others (Kappas, 2001). When a client's
type of suggestibility is known and used, hypnosis achieves results with the least effort and least amount
of time (Kappas, 2001).
Hypnotherapy Without (or With) Hypnosis
All behavior, thought, or habit is motivated by something, has a purpose and this is positive
(Hunter & Eimer, 2012). There is an enormous wealth of material stored in the Nonconscious Mind
(NCM) and in the psychosomatic problems such as eczema, irritable bowel, colitis, asthma, allergies,
rheumatoid arthritis and some types of autoimmune diseases, such as T1DM, the "reason" is usually "not
conscious" (Ewin & Eimer, 2007). Since these "reasons" are not conscious, the patient cannot consciously
know them or verbalize them, apart from being "protective" or at least having a positive purpose (Ewin &
Eimer, 2007).
In the present paper an innovative and promising psychotherapeutic mind - body approach was
used, which seeks the solution of internal conflicts or the "cure" of psychosomatic diseases through the
communication of internal processes.
Subliminal Therapy, Analytical Hypnotherapy and Transactional Analysis. The analytical techniques we
have followed in this research are person-centered and focused on solutions, since people have all the
resources they need and that the answers to their problems lie within their mind (Hunter & Eimer, 2012).
These techniques help to "un-cover" (in the sense of "un-covering", making visible) the reason
(intention/purpose) behind the problem and re-meaning the patients’ underlying pathogenic factors and
symptoms. In this way, it is possible to adequately reinterpret the need underlying the presence of this
dysfunctional behavior and replace the symptom with a more appropriate behavior (Oliveira, 2015).
In this sense, Yager (2011, pp. 17-20), creator of
the mental superstructure of NMC: [1] In our mind, there is an intelligent capacity that is nonconscious,
which we call Nonconscious Intelligence NCI); [2] communication between the NCM and the Conscious
Mind (CM) is possible in several ways (visual, auditory, kinesthetic); [3] NCM consists of a set of parts
(subsystems) that can operate autonomously; [4] in the NCM there is an entity that can be considered and
described as "superior intelligence" (NCI) that is not clearly definable consciously but easily subjectively
authenticated. The NCI, the smarter part of nonconscious mental life, is set up as a bank of memories, like
a computer, in which the NCM creates, stores, and keeps everything that happens to us, and through
hypnotic regression it is possible to explore the deposit of memories that may be forgotten by the NCM
(Hunter & Eimer, 2012). This instance of the mind regulates involuntary functions of the Autonomic
Nervous System (like the heart, breathing, among others), is the seat of emotions and imagination,
controls habits and is a kind of dynamics, a directed energy that motivates us (Hunter & Eimer, 2012).
Problem Statement
Despite investigations and theoretical rationale for using hypnosis in DM, studies to evaluate the
efficiency of hypnotherapy in the management and monitoring of diabetes, namely in T1DM have not yet
been performed.
Research Questions
Given the scant investigation of the effectiveness of scientific clinical hypnosis in T1DM, one
might ask: do psychotherapy with analytical hypnosis coupled with Guided and Creative Imagery (GCI)
lower blood sugar levels?
Two groups were randomly assigned: an experimental group (EG) in which the participants were
submitted to said protocol of HWH an GCI, and a control group (CG) in which participants only saw a
film about the human body, but without any reference to the pancreas and DM.
Thus, we hypothesized that:
�H1 - Patients with T1DM of EG are expected to lower blood sugar and HbA1c levels
compared to CG.
H2 - It is expected that in patients with T1DM the decrease in blood glucose will be greater from
the 2nd needle prick (during GCI) to the 3rd needle prick (after the posthypnotic suggestions and the
command for self-hypnosis.
Purpose of the Study
In this sense, the present study seeks to investigate the efficiency of analytic hypnotherapy in a
person-centered and solution-focused approach, called HWH - Hypnotherapy Without (or With)
Hypnosis, combined with Guided and Creative Imagery, in the monitoring of diabetes in patients with
T1DM (glycemia and glycosylated hemoglobin).
Research Methods
Participants
In order to select the individuals in the study, they had to fulfill the following inclusion criteria:
diagnosis of T1DM, users and/or members of the Ovar Diabetic Association, diagnosed for at least one
year, on an outpatient basis (not hospitalized), without any acute disease and non-pregnant.
Participation of the individuals was voluntary and they signed a consent and voluntary agreement for
participation in the study.
The sample consisted of 30 participants, 19 (63.30%) female and 11 (36.70%) male, between 11
and 51 years, with a mean age of 31.73 years (SD = 11.47). The CG comprised 15 participants, 10
females and 5 males, with a mean age of 34.00 (SD = 12.80). The EG, intervention with HWH and GCI,
consisted of 15 participants, 9 females and 6 males, with a mean age of 29.47 years (SD = 9.88). During
the investigation, it was found that two female subjects had an Insulin Infusion Pump and were therefore
excluded, making up a final sample of 28 participants.
The sociodemographic characteristics are presented in Table 1.
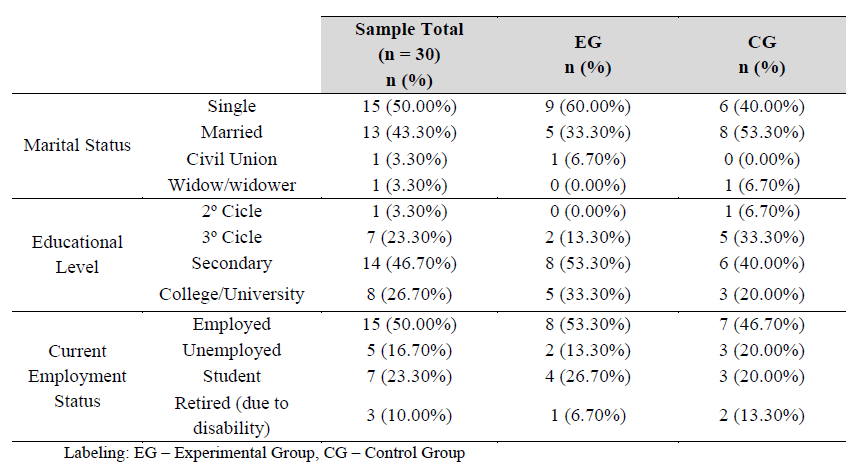
Labeling: EG – Experimental Group, CG – Control Group
Materials
Kappas Physical and Emotional Suggestibility Tests (Kappas, 2001), with permission. This instrument
serves to distinguish the profiles of suggestibility: physical and emotional. It consists of two
questionnaires, one for each profile, each with 18 affirmations, with a dichotomous "yes / no" answer.
In order to know the suggestibility of each participant, the following procedure is followed,
according to the original version: [1] the number of answers "Yes" is counted in each one of the
questionnaires and 10 points are assigned to questions 1 and 2 and five points to questions 3 to 18; [2]
questionnaire scores are added together to get the combined score. [3] the combined score is located on
the upper horizontal line of the double-entry matrix; [4] the score for Questionnaire # 1 is located to the
left of the vertical column of the double entry matrix; [5] a horizontal line is drawn across the score page
of Questionnaire #1 and a vertical line down the combined score; [6] the number where the two lines
intersect represents the percentage score adjusted for Questionnaire #1. That is, the value indicates the
percentage of physical suggestibility; [7] subtract at 100 the value of the percentage of physical
suggestibility to determine the percentage of emotional suggestibility (Kappas, 2001). This procedure
allows to infer the suggestibility profile.
A benchmarking study was not carried out to obtain the percentiles for the Portuguese population,
since it would be unaceptable in terms of time and in financial terms, within the scope of a master's thesis.
This fact is an obvious limitation, even though validity was guaranteed by the judges' method and the
spoken reflection with 20 diabetics who did not participate in the study.
To measure glucose, we used disposable lancets, test strips, glucometer, cotton and registration
sheet. In the control group we used the computer, the film and the structured script.
Procedure
Initially, informed consent was given to the participants, which contained relevant information
such as the purpose of the study, benefits to the participants, risks, among others. All the participants
signed this consent, filling in the Sociodemographic Questionnaire.
The research was conducted in three face-to-face sessions, each lasting approximately 60 minutes.
In this session, when the prerequisites for participation in the investigation were fulfilled, the
questionnaire of sugestibility was submitted to fill in and the value of HbA1c of the last blood test (pre-
intervention) was requested. In the first session, the participants were educated for the hypnosis process,
using metaphors and hypnotizability tests, and a communication set-up was made with the NCI. The
second session took place in the following two weeks, in which the participants went through their
respective conditions. The EG was submitted to the structured intervention (HWH) proposed by Oliveira
(2015) and GCI, according to the protocol of intervention, while the CG visualized a film about the
human body. Considering that the NCI listened and worked without the conscious consent of the patient,
we paid particular attention to the neutral content of the film, since any suggestion related to the pancreas
and/or T1DM could constitute a parasite variable. After a week, the third session was held, where a
debriefing was held. Three months after the last blood test, having already passed the condition, the
HbA1c value of the respective blood test (post-intervention) was requested.
The intervention protocol is outlined in Table 2.
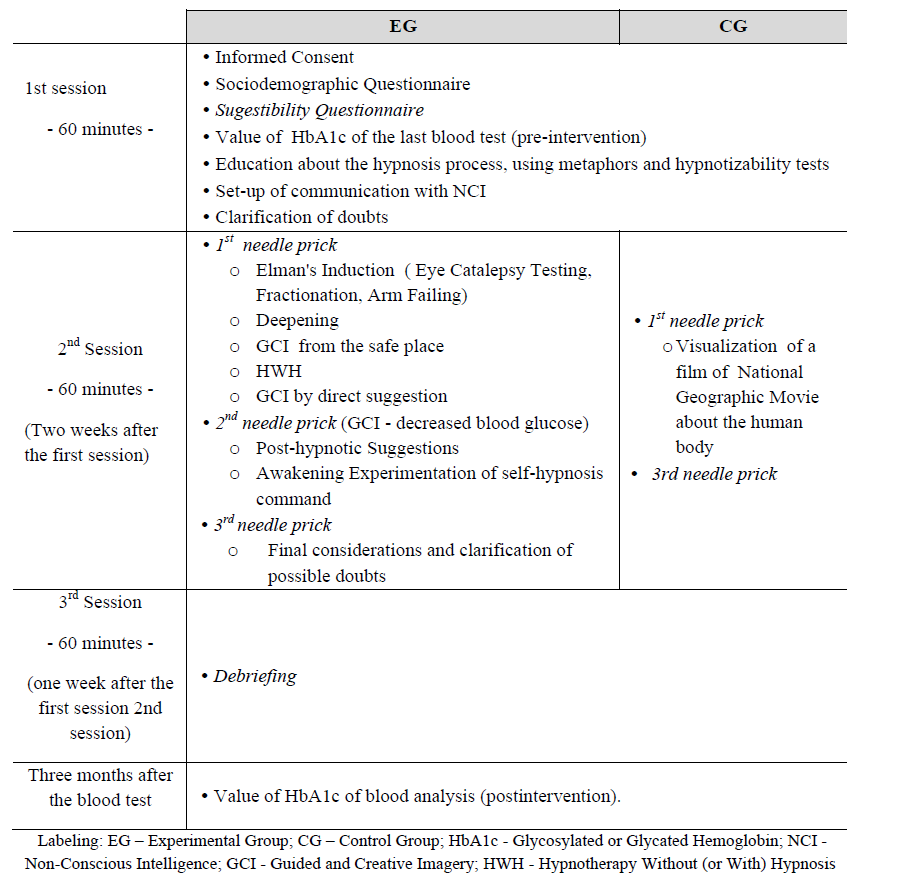
Labeling: EG – Experimental Group; CG – Control Group; HbA1c - Glycosylated or Glycated Hemoglobin; NCI - Non-Conscious Intelligence; GCI - Guided and Creative Imagery; HWH - Hypnotherapy Without (or With) Hypnosis
Data Analysis
The data were entered into the Statistical Package for the Social Sciences ® (SPSS Software) and
a data analysis was performed in the first instance to standardize all results with the transformation of the
Table 1.raw scores into Z scores, in order to facilitate the comparing of performances between the experimental
and control groups, as well as between the different stages of intervention.
Whenever normality assumptions (Kolmogorov-Smirnov test "p" values greater than .05) were
guaranteed we used parametric tests, but confirmed with non-parametric tests, given that, despite the
normality of the distributions, the sample N is lower than N.
We determined averages, standard deviations, minimum and maximum and median values. We
performed Student's t-tests to compare the two groups, the respective non-parametric version of Mann-
Whitney U, the Wilcoxon Z test for non-parametric comparison of repeated measures in the experimental
group.
As alphas to determine statistical significance, we used the value of .05 for statistically significant
differences (CI = 95%), the value of .01 for statistically very significant differences and .001 for
statistically significant differences.
Findings
In this section we present the test results of the two hypotheses.
Thus, in relation to the first hypothesis, according to which "patients with T1DM of the EG are
expected to lower blood sugar and HbA1c levels in comparison with the CG", we compared the two
groups in terms of the magnitudes of variations between 1st and 3rd needle pricks. Table 3 (Student's t-test)
shows that there is a decrease in standardized blood glucose (z-scores) from the 1st to the 3rd needle pricks
and in CG there is an increase.

However, the variation between the two groups is not statistically significant (t = -1.165; gl = 26; p
= .255). That is, we did not confirm the first hypothesis regarding glycemias. The non-parametric Mann-
Whitney U test was in the same direction (U = 72; p = .240).
In relation to the variation of the normalized values (z-scores) of HbA1c, in order to test the first
hypothesis, we found in table 4 (Student's t-test) that in the experimental group there was an increase in
HbA1c and in the control group there was a decrease.

Yet, the variation between the two groups is not statistically significant (t = 2.129, gl = 14, p =
.051). That is, we did not confirm the first hypothesis regarding HbA1c. The non-parametric Mann-
Whitney U test, however, suggests a statistically significant difference between the EG and the CG (U =
12; p = .036), with the EG presenting a median of +36 (increase in HbA1c) and CG a median of -18
(decrease in HbA1c).
In sum, the first hypothesis was not confirmed for both measures.
Regarding the second hypothesis, according to which "it is expected that in the patients with
T1DM of EG the decrease of the glycemia is greater from the 2nd needle prick (during the GCI) to the 3rd
needle prick (after the post-hypnotic suggestions and the command for self-hypnosis "), Table 5 shows
that in the 3rd needle prick, the median of the standardized blood glucose levels is lower than the median
of the blood glucose obtained at the 2nd needle prick (GCI moment at which the participants felt decreased
glycemia).

That is, in the 3rd needle prick the blood glucose decreased (in the EG) in relation to the glycemia
of the 2nd needle prick, the same happened with the minimum and maximum values. In relation to the
decrease in medians, the difference is statistically significant (Z = -2.272, p = .023).
In sum, the second hypothesis was confirmed.
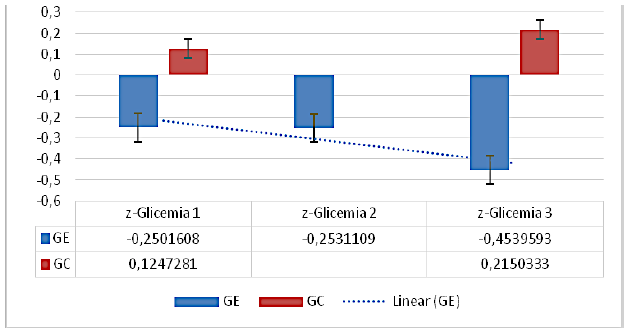
In summary, and as can be seen in Figure
glycemia values above the sample mean (N = 28), the glycemia from the 1st to the 3rd needle prick
increased. The participants of the experimental group started with blood glucose values below the sample
mean (N = 28), increased from 1st to 2nd needle prick but decreased from 2nd to 3rd needle prick.
Visual analysis (Figure
However, we did not find any statistically significant differences between the groups in the 1st
needle prick (U = 74.5, p = .289) and in the 3rd needle prick (U = 66.0, p = .147).
Conclusion
T1DM is a chronic disease and one of the major public health problems, given the high risk of
mortality and high morbidity, affecting milliions of people worldwide. Failure to monitor glycemia
results in the early onset of late complications of the disease, affecting Quality of Life (Ferreira, 2015).
Psychological factors play a crucial role (Martinez et al., 2016), psychological intervention is
fundamental (Gatchel & Oordt, 2015), making hypnotherapy constituting a tool Potentiating and
complementary psychotherapeutics (Trujillo, 2010). Due to the lack of investigation of the efficiency of
hypnotherapy in T1DM, there is a great need to investigate the influence of hypnotherapy, in an analytical
approach with HWH, and of GCI, in glycemia, in HbA1c.
We emphasize that, from the beginning to the end of the intervention, the hypnotic group
decreased the standardized blood glucose levels, while the group that visualized the film increased.
Therefore, hypnosis seems to contribute to good glycemic control.
Regarding HbA1c, we found that the variation of HbA1c between the two groups is also not
statistically significant, with EG having an increase in HbA1c and a decrease in CG. However, when
using the non-parametric Mann-Whitney U test, a statistically significant difference between the EG and
CG is suggested.
Regarding the glycemia between the 2nd and 3rd needle prick, the results found allow us to verify
that the hypnosis group decreased the glycemia in the 3rd bite (after the hypnotic suggestions and
command of self-hypnosis) in relation to the 2nd needle prick. The moment of GCI in which the
participants felt the glycemia to be decreased), as well as the minimum and maximum values. Moreover,
we verified the difference is statistically significant between the groups in the decrease of the medians.
These results may be partially corroborated by Petruzzi (2016), in the sense that when a person is relaxed
and with their attention focused on the thoughts and ideas that can help them achieve the desired result in
their life, Your chances of success are greatly increased.
Finally, although initially it appeared that both groups increased the glycemia, in the EG there was an inflection, with increase of the 1st to the 2nd needle prick, beginning the glycemia to descend from the 2nd to the 3rd needle prick. The tendency of glycemia (although not significant, from the 1st to the 2nd
needle prick) in the hypnosis group can be related to the regression, revision and revival process,
ressignification, reintegration, remission and reprogramming / relearning. In the same sense, given that
the NCM works without the participant's knowledge, the NCI causes the body to feel what the mind
imagines (Erickson et al., 1976), when suggesting regression to the moment of entry of T1DM into the
body, may have had an influence on the increase of blood sugar levels. Inflexion suggests a dose-response
problem (Oliveira, 2009). Considering the results obtained, it is possible to suggest that hypnotherapy
allows the decrease of glycemic, ie a good glycemic control, being a greater reduction as with GCI by
direct suggestions, with post-hypnotic suggestions and with self-hypnosis.
It should be noted that the study has some limitations such as not having controlled the
participants' lifestyle between the intervention sessions, such as diet or non-compliance with the diet plan,
physical exercise, or insulin administration, different moments of the day they were performed, the time
of insulin action since it is imagined is variable between subjects, and may have biased the results. This
study also suffers from limitations inherent in the evaluation instrument, namely the
Questionnaire.
Considering the results obtained, although limited, it seems important to carry out studies with
children and adolescents with T1DM in a larger sample so that more generalizable and consistent
conclusions can be drawn. On the other hand, it would be relevant to develop a longitudinal study, whose
intervention included more sessions / trials, in addition to the three sessions conducted in this study and
follow-up sessions. The purpose of this study was to study the effect of hypnosis on the variation of
blood glucose between sessions, the variation in the amount of insulin administered and changes in
lifestyles, minimizing chronic complications of the disease and the well-being of people. In addition, we
suggest the study of the regression to the moment of entry of T1DM into the body and its influence on
blood glucose.
Acknowledgments
To the Association of Diabetics of Ovar for the trust and availability for this work, and other
elements of its Youth Nucleus, who gave their time to participate in this study.
References
- Ader, R., & Cohen, N. (1975). Behaviorally conditioned immunosuppression. Psychosomatic Medicine,
- 37(4), 333–340.
- Almeida, M., Ferrão, A., & Zangeronimo, M. (2013). Aspectos farmacológicos da insulinoterapia no
- Diabetes Mellitus Tipo 1. NOV@: Revista Científica, 2(2).
- Bastarache, R., & Bastarache, R. (2014). Modern hypnosis: Advanced hypnotherapy workbook. American
- School of Hypnosis.
- Ewin, D., & Eimer, B. (2007). Ideomotor Signals for Rapid Hypnoanalysis: A How-To Manual. American Journal of Clinical Hypnosis, 49(3).
- Ferreira, L. (2015). Sociedade Portuguesa de Diabetologia. Retrieved December 10, 2015, from http://www.spd.pt/index.php/qualidade-de-vida-e-diabetes-mainmenu-107 Ferreira, P., Repolho, M., Ribeiro, M. J., & Sepodes, B. (2012). Diagnóstico e abordagem terapêutica da Osteoartrite. Revista Portuguesa de Farmacoterapia, 4, 15–28.
- Kappas, J. (2001). Professional hypnotism manual: Introducing physical and emotional suggestibility and sexuality (4th ed.). Van Nuys, CA: Panorama Publishing Company.
- Oliveira, C. (2015). HSH - Hipnoterapia Sem (ou com) Hipnose: Manual de Apoio ao Curso Básico de HSH.
- Roe, K., Visovatti, M., Brooks, T., Baydoun, M., Clark, P., & Barton, D. (2016). Use of complementary therapies for side effect management in breast cancer: evidence and rationale. Future Medicine.
- Rossi, E. (1993). The psychobiology of mind-body healing: New concepts of therapeutic hypnosis.
- U.S.A.: W. W. Norton & Company, Inc.
- Trujillo, T. (2010). Hypnotherapy for Immune Disorders. (A. H. Association, Ed.). American Hypnosis
- Association.
- van der Ven, N., Lubach, C., Hogenelst, M., van Iperen, A., Tromp-Wever, A., Vriend, A., … Snoek, F.
- (2005). Cognitive behavioural group training (CBGT) for patients with type 1 diabetes in persistent poor glycaemic control: Who do we reach? Patient Education and Counselling, 56(3), 313–322.
- World Health Organization. (2015). Diabetes Programme. Retrieved October 1, 2015, from http://www.who.int/diabetes/action_online/basics/en/index1.html Xu, Y., & Cardeña, E. (2008). Hypnosis as an adjunct therapy in the management of Diabetes. International Journal of Clinical and Experimental Hypnosis, 56(1), 53–72.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
08 May 2017
Article Doi
eBook ISBN
978-1-80296-021-1
Publisher
Future Academy
Volume
22
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-283
Subjects
Psychology, clinical psychology, psychotherapy, abnormal psychology
Cite this article as:
Rodrigues, F., Oliveira, C., Silva, C. F., & D’Almeida, A. (2017). Psychotherapy Intervention With Hypnosis In Patients With Type 1 Diabetes Mellitus. In Z. Bekirogullari, M. Y. Minas, & R. X. Thambusamy (Eds.), Clinical & Counselling Psychology - CPSYC 2017, vol 22. European Proceedings of Social and Behavioural Sciences (pp. 76-88). Future Academy. https://doi.org/10.15405/epsbs.2017.05.10