
A Study on the Dietary Behavior in School-aged Children


Abstract
Adopting a balanced and healthy diet is a public health system priority. The aim of this study is to identify dietary behaviors (consumption of fruit, vegetables, dairy products, pasta, meat, sweets, fast food) of a sample of pupils and whether there are significant differences in terms of demographic variables, such as age, gender and weight. In order to obtain data on the dietary behavior, a questionnaire containing 14 items was applied to a total of 234 schoolchildren, between 12 and 15 years. The field work was conducted between April and June 2014. Participation in this study was completely voluntary and the participants’ anonymity was guaranteed. There were identified significant differences of dietary behavior by gender (F(5, 228) = 4.38; p < 0.001; η2 = 2.25), respectively (F(4, 229) = 2.58; p < 0.05; η2 = 2.41). As regards age, no significant differences were found (F(5, 228) = 1.95; p > 0.05), respectively (F(4, 229) = 1.14; p > 0.05) and weight (F(5, 228) = 1.97; p > 0.05), respectively (F(4, 229) = 1.03; p > 0.05). Analyzing the post ad-hoc Bonferroni tests, significant differences were identified between dietary preferences, depending on age, gender, and weight. The consumption of sweets and fast food is high. An unbalanced diet can have severe consequences on the health condition of the school population, leading to chronic diseases, like arterial hypertension, type 2 diabetes mellitus, etc.
Keywords: Dietary behaviourfast foodstudentsdemographic variableshealth condition
Introduction
Adopting a balanced healthy dietary behaviour represents a priority of the public health system.
Both children and young people are a very important target group because the early adoption of
healthy dietary habits is the most effective method of maintaining long-term health condition. Society,
family, education organizations, the media, as well as food industry, are focused on the improvement
of the dietary behaviour. The aim is to maintain an adequate nutritional balance as required by a
normal body growth and development and avoid the occurrence of excess body weight. Diet imbalance
and overeating can lead to an excessive energy intake in children and adolescents favouring the
apparition of obesity (Krebs et al., 2007). The current dietary habits have an obesogenic character due
to their high fat and carbohydrate content. A mismatch between caloric intake and energy consumption
can bring about disturbances of the individual’s energy balance (Donald, 2002).
Most cases of overweight are the result of a caloric intake that exceeds the individual’s energy
consumption (Beers, 2006). The global increase of excess weight prevalence is generated by the
energy intake, especially due to high calorie foods rich in fats, sugars as well as reduced physical
activity as a consequence of increased sedentarism.
The frequent consumption of fast-foods has been associated with the increase of the body mass
index (Rosenheck, 2008). In the USA, both children and adult diets increasingly include fast-foods
meals (Guthrie, Biing-Hwan and Frazao, 2002). As regards children (Bowman et al., 2004),
adolescents (Bauer et al., 2009), as well as adults (Bowman and Vinyard, 2004), their consumption has
been associated, on the one hand, with increased caloric intake, based on saturated and trans fatty acids
(Asgary et al., 2011), sodium, sugar and acidulated beverages and, on the other hand, with a low
consumption of fruits, vegetables and milk. Moreover, fast-foods tend to have high energy value and
low nutritional quality in contrast with home-prepared foods and dietary recommendations (Guthrie,
Biing-Hwan and Frazao, 2002). Previous studies showed that the availability of these foods near
schools is associated with an increased body mass index in schoolchildren (Chiang et al., 2011), while
the consumption rate has increased over the last years in both children and adolescents (Demory-Luce,
2005).
As regards children with overweight in the first years of life, the risk for them of becoming
obese adults is 80% if both parents are obese and 40% if only one parent is obese (Arion et al., 1983;
Nader et al., 2006). Overweight occurring both during childhood and adolescence, increases the risks
of developing cardiovascular diseases (Ogden et al., 2002, Isganaitis and Lustig, 2005), depressions
(Hedley et al., 2004), arterial hypertension (Summerbell et al., 2005), several forms of cancer
(Kelishadi, 2006), type 2 sugar diabetes (Kelishadi, 2007), sleep apnea syndrome, orthopedic diseases,
as well as diseases of psychological and social nature (Lobstein, Baur and Uauy, 2004, Reilly et al,
2003, Bayer et al, 2011). Adolescent overweight can produce negative long-term effects on adults’
health, regardless of the ponderal status (Must et al, 1992, Bayer et al, 2011).
Worldwide, the prevalence of childhood obesity has increased over the two last decades. At the
beginning of 2000, in the European countries the prevalence of childhood overweight varied between 6
and 36% (Lobstein and Frelut, 2003). In some countries an annual increase of up to 1% could be
observed (Jackson-Leach and Lobstein, 2006).
Materials and Methods
This study was conducted between April and June 2014 at the General School No 30 of Braşov.
The study has been approved by the Ethics Commission of the Transilvania University of Brașov. Also,
the research on human subjects obtained the informed consent agreement of the participating subjects and
of their parents. Participation in this study was voluntary and the anonymity of the participants was
ensured.
The study comprised a number of 234 gymnasium-cycle schoolchildren of which 116 were girls
and 118 boys with ages between 12 and 15 years
In order to acquire information regarding food hygiene, a questionnaire containing 14 items was
applied, with the title: „Dietary habits and the pleasure to practice physical activities”. The questionnaire
was set up by the authors in collaboration with the staff members from the Faculty of Physical Education
and Mountain Sports of Braşov. In order to find out whether there are significant differences between the
dependent variable (dietary behaviour) and the independent variables, the ANOVA 2 test was conducted
(age) x 2 (gender) x 2 (weight). Also, in order to find out whether there are differences among the dietary
preferences of the questioned schoolchildren, the post ad-hoc Bonferroni test was applied.
Result interpretation, tables, and graphs were performed and created with Microsoft Office Excel
2010.
Results
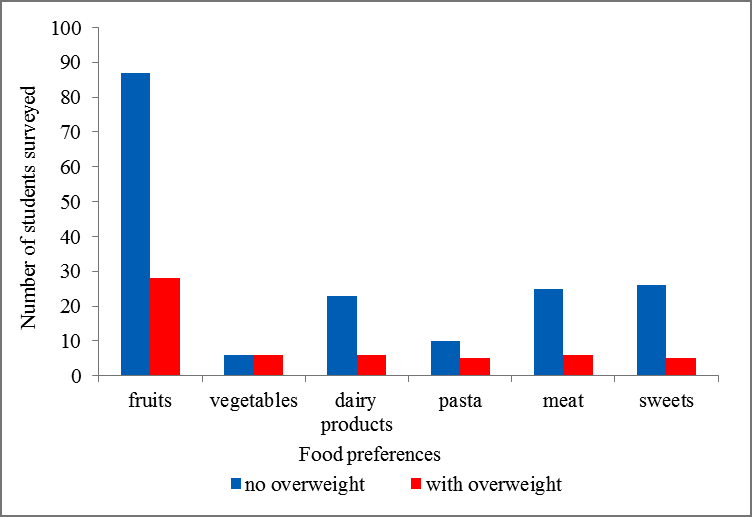
The results obtained after applying the questionnaire indicate that around 50% of the questioned
schoolchildren consume fruits, 20.34% of the boys consume meat, and 20.70% of the girls consume
sweets. Considering the two groups, the statistical analysis showed a strongly statistically significant
difference between them. The significance threshold is p = 0.0010 < 0.001 for Chi-Square = 20.50 and df
(degrees of freedom) = 5 (Table
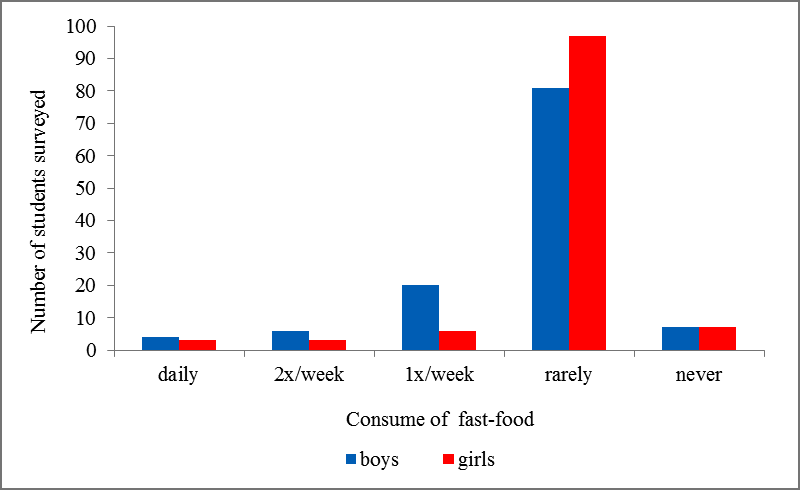
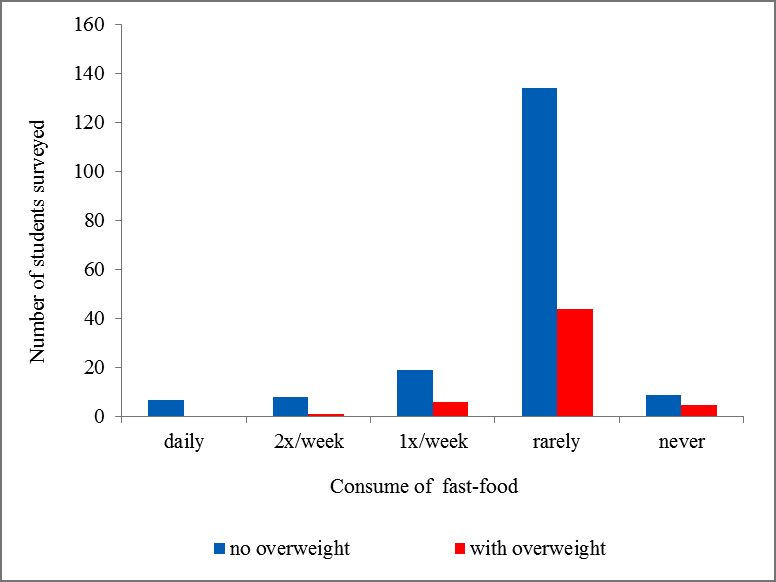
Similarly, around 75% of the questioned schoolchildren rarely consume fast-foods, 17% of the
boys consume fast-foods once a week, 6 - 7% of them don’t eat fast-foods at all, and a very low
percentage eat it every day. Considering the two groups, the statistical analysis showed a statistically
significant difference between them. The significance threshold is p = 0.0387 < 0.05 for Chi-Square =
2.51 and df (degrees of freedom) = 2 (Table
Significant differences were identified as regards the dietary behaviour depending on gender (F(5, 228)
= 4.38; p < 0.001; ƞ2 = .088) and (F(4, 229) = 2.58; p < 0.05; ƞ2 = .043), respectively. This situation indicates that girls (DS =19.55) are more careful when choosing the types of food, in contrast with boys (DS =20.15)
(Figure
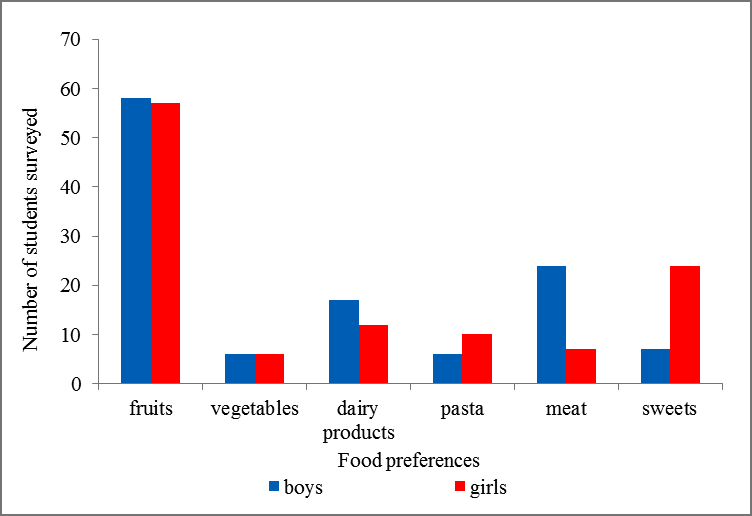
It can be ascertained that boys are less preoccupied with dietary hygiene in contrast with girls.
Thus the size of the effect (ƞ2 = .088) explains a difference of 14.31% as regards the boys’ preference for
meat consumption (Table
Also, as regards fast-foods consumption, boys consume more than girls. The size of the effect (ƞ2
= .043) shows a difference of 12.64% regarding the preference of the former for fast-foods of around
2x/week (Table
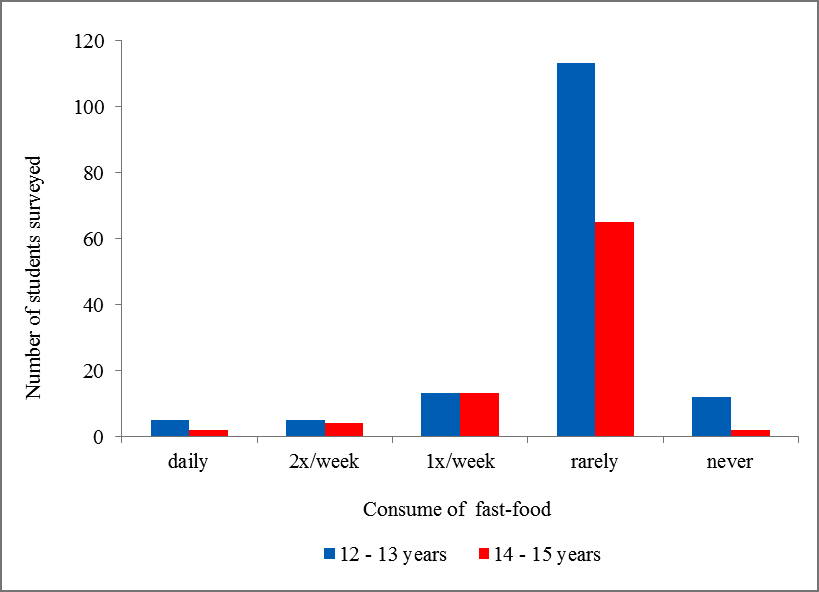
No significant differences were observed in terms of age) = 1.14; p > 0.05) (Figure
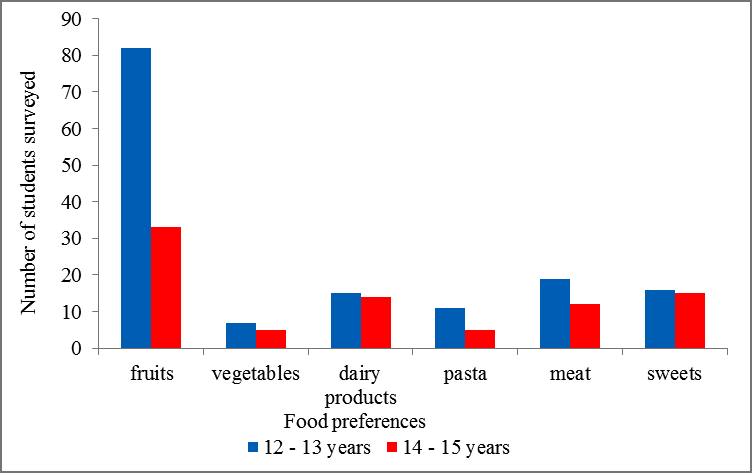
After analyzing the responses obtained from the questioned schoolchildren it was found that there
are differences as regards their dietary preferences. For p < 0.001, after applying the Bonferroni test, a
significant difference was recorded among dietary preferences in terms of gender, as regards meat and
sweets. Also, for p < 0.05, significant differences were observed among schoolchildren’s preference for
meat and dairy products, as well as for meat and fruits. No significant differences were observed as
regards schoolchildren’s dietary preferences depending on age or weight (Table
Discussions
To the question „What kind of food do you like best?”, around 50% of the questioned
schoolchildren declared to have a preference for fruits , 5% for vegetables, between 10.30 and 14.41%,
for dairy products, 8.66% of the girls prefer pasta, 20.34% of the boys prefer meat and 20.70% of the
girls prefer to consume sweets. Although nutrition guides do not specify the dose of sugar that can be
consumed per day, these recommend a diminished sugar intake. Children and adolescents tend to have
diets rich in carbohydrates with additional sugar of around 18% of the total of daily calories. Acidulated
beverages contain a large amount of sugar and contribute with around 8% to the daily caloric intake of
children and youths aged between 2 and 18 (Reedy & Krebs-Smith, 2010).
According to a national study „Youth Risk Behavior Survey” (YRBS) conducted in 2009, 22.9%
of the schoolchildren from 9th to 12th grade declared consumption of fruits and vegetables at least 3
times per day (CDC, 2010). The study conducted in 2015 indicates that 20% of these declared the
consumption of fruits and vegetables. Nutrition guides recommend for youths between 9 and 18 a daily
consumption of three cups of milk or dairy equivalents with low fats content (US Department of
Agriculture, Agricultural Research Service; 2010). Around 15% of the 9th-12th grade schoolchildren
were consuming in 2009 at least 3 cups of milk per day yet this percentage decreased in 2015, to 10.2%
(US Department of Agriculture, Agricultural Research Service, 2010, CDC, 2010, 2016). Between 2007 –
2008 it was found that girls aged between 12 – 19 years showed an insufficient calcium intake, around
878 mg of calcium per day, which is only 67% of the recommended daily dose (US Department of
Agriculture, Agricultural Research Service, 2010). Also, since 1970 and until the mid 1990s, milk
consumption of female adolescents has decreased by 36% (Sacks et al., 2010).
As regards children and adolescents, nutrition guides recommend a consumption of integral
cereals of at least half of the daily intake, depending on age and gender. Children and youths aged
between 4 and 18 years do not consume the mínimum daily amount of integral cereals as is
recommended. Between 2001 - 2004, the intake of integral cereals for this age group varied between 0.26
oz. and 0.48 oz., much less than the recommended amounts (US Department of Agriculture, Agricultural
Research Service, 2010).
When asked „Do you eat fast-foods on a regular basis?” 2.59% of the girls and 3.39% of the
boys declared to eat fast foods on a daily basis, 2.60% of the girls and 5.08% of the boys consume fast-
foods 2 – 3 times per week, 83.60% of the girls and 68.64% of the boys rarely consume fast-foods, 4.31%
of the girls and 16.95% of the boys consume fast-foods once a week, while 6 - 7% of the schoolchildren
do not eat fast-foods. Youths who admitted frequent consumption of fast food (at least three times per
week) are most likely to maintain that healthy foods taste bad, that they didn’t have time to eat healthy
foods, and they were not interested in a healthy diet (Neumark-Sztainer et al., 2003; Zabinski et al.,
2006). Between 1994 and 1998, about three out of ten children and adolescents have consumed at least
one fast-foods meal per day, these having a higher calorie intake than those who did not consume this
type of meal (Bowman, 2004).
Empty calories from foods and beverages with added sugars and saturated fats contribute with
40% to the daily calorie intake in children and adolescents aged between 2 and 18 years thus affecting the
quality of their diet (Reedy and Krebs-Smith, 2010). Young people consume daily more calories from
acidulated beverages than from milk. Boys aged between 12 and 19 years consume on average 22 g of
acidulated beverages/day, twice as much than their milk intake (10 g). On average, girls consume 14 g of
acidulated beverages and only 6g of milk/day (Forshee et al., 2006).
Between 2007 - 2008, the frequency of calories originating in saturated fats, consumed by
children and youths aged between 6 and 19 years, was 33%. Even if this percentage is similar with the
value suggested by the nutrition guides for daily fats consumption (25% - 35% of the total amount of
calories), persons aged between 6 and 19, consume more than the recommended daily amount of
saturated fats (10% of the total amount of calories), varying between 11% and 12% (US Department of
Agriculture, Agricultural Research Service, 2010).
Certain behaviours and attitudes encountered in children and adolescents relate with healthy
diets. E.g., setting certain goals as regards the consumption of fruits and vegetables or offering rewards
for fruits and vegetables consumption as well as the pleasure related to their taste are important predictors
for the consumption of such foods (Zabinski et al., 2006). The family environment strongly influences the
youths’ dietary behaviour. The family’s readiness to consume healthy foods is one of the most important
hypotheses as regards the consumption of fruits, vegetables, and dairy products (Larson et al., 2006;
Neumark-Sztainer et al., 2003). Menus that are specific to each family, the rules of a healthy diet
established in each family as well as the parents’ healthy lifestyle influence the youths’ consumption of
fruits, vegetables, dairy products and fats (Neumark-Sztainer et al., 2003; Zabinski et al., 2006; Larson et
al., 2007; Van der Horst et al., 2007).
Conclusions
Meat consumption (20.34% of the boys) and sweets consumption (20.70% of the girls) are high in
schoolchildren aged between 12 – 15 years.
Vegetables consumption is low in schoolchildren aged between 12-15 years, 5.08% in boys and
5.17% in girls.
A significant percentage of the questioned boys (5,08%) consume fast-foods 2 – 3 times per week.
Significant differences were identified with regard to the dietary behaviour depending on gender,
whereas no differences were observed regarding the age and weight of the questioned subjects.
References
- Arion C., Dragomir D., Popescu V. (1983) Obezitatea la sugar, copil şi adolescent, Ed. Medicală Bucureşti.
- Asgary S., Nazari B., Sarrafzadegan N. et al. (2011). Evaluation of fatty acid content of some Iranian fast foods with emphasis on trans fatty acids, Asia Pacific Journal of Clinical Nutrition, vol.70, no. 1, pp. 82–91.
- Bauer K., Larson N., Nelson M., Story M., Neumark-Sztainer D. (2009). Fast food intake among adolescents: secular and longitudinal trends from 1999 to 2004. Prev Med; 48: 284–287.
- Bayer O., Kruger H., Von K.R., et al. (2011). Factors associated with tracking of BMI: a metaregression analysis on BMI tracking. Obesity (Silver Spring);19:1069–76.
- Beers M.H. & coord.(2006) Manualul Merk de diagnostic şi tratament, Edit. a XVIII-a, Ed. All, Bucureşti.
- Bowman S., Gortmaker S., Ebbeling C., Pereira M., Ludwig D. (2004). Effects of fast-foods consumption on energy intake and diet quality among children in a national household survey. Pediatrics; 113: 112–118.
- Bowman S., Vinyard B. (2004). Fast food consumption of U.S. adults: impacts on energy and nutrient intakes and overweight status. J Am College Nutr; 23: 163–168.
- CDC (2010). Youth risk behavior surveillance—United States. MMWR 2009;59(No. SS-5). Available online at http://www.cdc.gov/mmwr/pdf/ss/ss5905.pdf. Accessed on 27.07.2016
- CDC (2016). Youth risk behavior surveillance—United States. MMWR 2015;59(No. SS-5). Available online at https://www.cdc.gov/healthyyouth/data/yrbs/pdf/2015/ss6506_updated.pdf. Accessed on 27.07.2016
- Chiang P.H., Wahlqvist M.L., Lee M.S. et al. (2011). Fastfood outlets and walkability in school neighborhoods predict fatness in boys and height in girls: a Taiwanese population study. Public Health Nutrition, vol. 14, no. 9, pp. 1601–1609.
- Demory-Luce D. (2005). Fast food and children and adolescents: implications for practitioners. Clinical Pediatrics, vol. 44, no. 4, pp. 279–288.
- Donald D., Hensrud D., traducător: Călimăneanu, G. (2002). Clinica Mazo–despre menţinerea unei greutăţi sănătoaseǁ, Editura All, Bucureşti.
- Guthrie J., Biing-Hwan L., Frazao E. (2002). Role of food prepared away from home in the American diet, 1977–78 versus 1994–96:changes and consequences. J Nutr Educ Behav; 34: 140–150.
- Hedley A.A., Ogden C.L., Johnson C.L. et al (2004). Prevalence of overweight and obesity among US children, adolescents, and adults, 1999-2002. JAMA;291(23):2847-2850.
- Isganaitis E. & Lustig R.H. (2005). Fast food, central nervous system insulin resistance, and obesity. Arteriosclerosis, Thrombosis, and Vascular Biology, vol. 25, no. 12, pp. 2451–2462.
- Jackson-Leach R., Lobstein T. (2006). Estimated burden of paediatric obesity and comorbidities in Europe. Part 1. The increase in the prevalence of child obesity in Europe is itself increasing. Int J Pediatr Obes;1:26–32.
- Kelishadi R. (2006). Childhood obesity in the Eastern Mediterranean region. In: Flamenbaum RK. Global dimensions of childhood obesity. 1st ed. New York, NY: NOVA Science Publishers,71-89.
- Kelishadi R. (2007). Childhood Overweight, Obesity, and the Metabolic Syndrome in Developing Countries, Epidemiol Rev.,29:62-76.
- Krebs F.N., Himes H.J., Jacobson D., Nicklas A.T., Guilday P., Styne D. (2007). Assessment of Child and Adolescent Overweight and Obesity. Pediatrics;120, Suppl. 4: S193-S228.
- Larson N.I., Neumark-Sztainer D., Hannan P., Story M. (2007). Family meals during adolescence are associated with higher diet quality and healthful meal patterns during young adulthood. J Am Diet Assoc;107(9):1502-1510.
- Larson N.I., Story M., Wall M., Neumark-Sztainer D. (2006). Calcium and dairy intakes of adolescents are associated with their home environment, taste preferences, personal health beliefs, and meal patterns. J Am Diet Assoc; 106(11):1816-1824.
- Lobstein T., Baur L., Uauy R.(2004). Obesity in children and young people: a crisis in public health. Obes Rev; 5 ((Suppl. 1):4–104.
- Lobstein T., Frelut M.L. (2003). Prevalence of overweight among children in Europe. Obes Rev;4:195–200.
- Must A., Jacques P.F., Dallal G.E., et al. (1992). Long-term morbidity and mortality of overweight adolescents. A follow-up of the Harvard Growth Study of 1922 to 1935. N Engl J Med;327:1350–5.
- Nader P.R., O'Brien M., Houts R. Et al. (2006). Identifying risk for obesity in early childhood. Pediatrics; 118:e594–e601.
- Neumark-Sztainer D., Wall M., Perry C., Story M. (2003). Correlates of fruit and vegetable intake among adolescents. Findings from Project EAT. Prev Med;37(3):198-208.
- Ogden CL, Flegal KM, Carroll MD, Johnson CL. (2002). Prevalence and trends in overweight among US children and adolescents, 1999-2000. JAMA;288(14):1728-1732.
- Olds T., Maher C., Zumin S., et al. (2011). Evidence that the prevalence of childhood overweight is plateauing: data from nine countries. Int J Pediatr Obes;6:342–60.
- Reedy J., Krebs-Smith S.M. (2010). Dietary sources of energy, solid fats, and added sugars among children and adolescents in the United States. J Am Diet Assoc;110(10):1477-1484.
- Reilly J.J., Methven E., McDowell Z.C., et al. (2003). Health consequences of obesity. Arch Dis Child;88:748–52.
- Rokholm B., Baker J.L., Sorensen T.I. (2010). The levelling off of the obesity epidemic since the year 1999—a review of evidence and perspectives. Obes Rev;11:835–46.
- Rosenheck R. (2008). Fast food consumption and increased caloric intake: a systematic review of a trajectory towards weight gain and obesity risk. Obes Rev; 9: 535–547.
- Sacks F.M., Svetkey L.P., Vollmer V.M., et al. (2001). Effects of blood pressure on reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med; 344:3–10.
- Swallen K.C., Reither E.N., Haas S.A., et al. (2005). Overweight, obesity, and health-related quality of life among adolescents: the National Longitudinal Study of Adolescent Health. Pediatrics; 115:340–7.
- U.S. Department of Agriculture, U.S. Department of Health and Human Services (2010). Dietary Guidelines for Americans. 7th Edition. Washington, DC, US Government Printing Office; 2010. Available online at http://www.health.gov/dietaryguidelines/dga2010/dietaryguidelines2010.pdf Accessed on 25.07.2016
- Van der Horst K., Oenema A., Ferreira I. et al. (2007). A systematic review of environmental correlates of obesity-related dietary behaviors in youth. Health Educ Res; 22:203-226.
- Zabinski M.F., Daly T., Norman G.J. et al. (2006). Psychosocial correlates of fruit, vegetable, and dietary fat intake among adolescent boys and girls. J Am Diet Assoc; 106(6):814-821.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
25 May 2017
Article Doi
eBook ISBN
978-1-80296-022-8
Publisher
Future Academy
Volume
23
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-2032
Subjects
Educational strategies, educational policy, organization of education, management of education, teacher, teacher training
Cite this article as:
Scurt, C., & Scurt, M. D. (2017). A Study on the Dietary Behavior in School-aged Children. In E. Soare, & C. Langa (Eds.), Education Facing Contemporary World Issues, vol 23. European Proceedings of Social and Behavioural Sciences (pp. 1667-1675). Future Academy. https://doi.org/10.15405/epsbs.2017.05.02.204