
Adherence to Recovery Exercise Program of Scapulohumeral Articulation After Breast Cancer Surgery


Abstract
The adherence to the recovery exercise program is the key to the optimal results in regaining the shoulder’s full range of motion. Patients and methods: This study was carried out on 30 patients with breast cancer following mastectomy and axillary lymph node dissection. We applied The Rotterdam Symptoms Checklist and A Brief Self Report Questionnaire on the first day after breast surgery and after one, three and six months. Results: The results revealed that the poorer the quality of life is perceived by the patient, the higher is the patient’s adherence to the recovery program. Also, the higher adherence at moment zero post surgery is, the higher the chance is to be high also after one, three and six months. Patients from our study evaluate their quality of life based mostly on the presence or the lack of psychological symptoms, despite the physical symptoms. Psychological state of the patient influences her activity score and vice-versa, return to the daily activities improves the psychological symptoms.
Keywords: Breast cancersupportive carephysical exercise
1.Introduction
Exercise is commonly recommended to women after breast cancer surgery, yet it is difficult for
patients and health professionals to adopt safe and beneficial types and modes of exercise. Well-designed
exercises are effective and beneficial for improving women's physical, physiological, and psychological
health outcomes after breast cancer treatment as well as to facilitate changes in exercise behaviors
(Chung, Lee, Hwang & Park, 2013).
The most common physical effects of early exercise training after breast surgery for cancer is that
it improves central transport, regional blood flow, the autonomic nervous system, skeletal muscle
physiology, and vasculature reactivity (Whellan, 2012). Reduced stress, reduced risk of cardiovascular
disease and reduced risk of cancer recurrence are also among the many benefits of physical activity for
cancer survivors (Cuevas, Hughes, Long, Ghosh & Li, 2014). These benefits have been shown to translate
into improved overall quality of life (Breast Cancer Surv Early physiotherapy after breast cancer surgery
improves overall quality of life, 2005). Also, the psychological effects of exercise training can’t be
ignored. Psychological benefits include enhancements in mood and vigor and decreases in depression and
anxiety (Courneya & Friedenreich, 1997).
Given the physical and mental benefits of physical activity for breast cancer survivors, focusing on
the associations between exercise, stress, and understanding the motivation to engage in exercise is an
important area of research (Cuevas, Hughes, Long, Ghosh, Li & al, 2014). Poor adherence can lead to
suboptimal effectiveness of treatment regimens, threats to patient safety, and increasing healthcare costs
for disease management (Gardner, 2014).
The terms adherence or cooperation are preferred to compliance. Compliance infers that the
patient is a passive recipient-which he or she is there to do whatever the health care professional
recommends. The second is that the responsibility for the patient's inability to adhere to an exercise
regimen is a shared responsibility, and rests with the patient and the physical therapist (Chung, Lee,
Hwang & Park, 2013).
Patient adherence usually relates to attending appointments, following advice and undertaking
prescribed exercise. Patient adherence to physical therapy home exercise programs is estimated between
35 and 72% (Rizzo, 2015).
Measuring adherence to home-based physical activity intervention requires methodology that
captures activities of daily living such as housework and gardening in addition to intentional aerobic
exercises such as walking and jogging and leisure activities such as bowling and golfing. In a home-based
physical activity program, activities of daily living, aerobic exercises, and leisure activities all are
important components of physical activity (Swenson, Nissen & Henly, 2010).
Adherence to an exercise program depends on patient’s motivation at the time of behavior. The
theory of self-determination offers an explanation for differences in adherence to exercise. SDT is based
on the assumption that the choices an individual makes are driven by self-determined motives and/or
externally determined motives. Typically, when exercise goals are self- determined, they reflect intrinsic
motivation based on enjoyment, competence, and social interaction.
When goals are not self-determined, but rather, interjected or controlled, they reflect motivation
that is driven by external sources; in general, research findings have demonstrated that this kind of
motivation undermines the development of autonomy, and is therefore not optimal for sustaining an
intentional physical activity. Presumably, when individuals feel pressured to exercise, they lack the
enjoyment and inner motivation to continue, causing them to discontinue their behavior (Kohlstedt,
Weissbrod, Colangelo & Carter, 2013).
The most common factors motivating participants were to improve overall health, improve
functional abilities, and enhance confidence and to reduce musculoskeletal issues (Jurkiewicz, Marzolini
& Oh, 2011).
Also, when provided with supervision and support, previous sedentary men and women can
achieve and maintain high levels of aerobic activity (Cadmus-Bertram, Irwin, Campbell, Duggan &
Foster-Schubert, 2014).
Studies have shown that subjects provided with regular feedback on their progress during an
exercise program achieve higher physical activity levels and are less likely to drop out of the program
than those without such feedback (Shakudo, Takegami, Shibata, Kuzumaki & Higashi, 2011).
A grater adherence is observed in the moderate intensity programs. Prescribing a higher frequency
increased the accumulation of exercise without a decline in adherence, whereas prescribing a higher
intensity decreased adherence and resulted in the completion of less exercise (Perri, Anton, Durning,
Ketterson & Sydeman, 2001).
Patients at a higher level of education and at older ages have a greater probability to follow the
indications (Uc-Coyoc, Coello-Reyes, Perez-Reynaud & Ponce, 2014). As adults move through the life-
course, their leisure lifestyles tend to center on a decreasing number of familiar activities, with a period of
gradual disengagement from many aspects of social life and an increasing tendency towards home-
centered leisure (Thurston & Green, 2004).
Other factors that influence adherence are: demographic factors, health status, physical and
psychological factors (Picorelli, Pereira, Pereira, Felicio & Sherrington, 2014).
One study showed that the unstructured group had higher exercise adherence, increased
enjoyment, and higher self-selected exercise intensity compared to the structured group. Reflective
journal analysis revealed increased feelings of relatedness, enjoyment, competence and personal
achievements in the unstructured group. These results show that during the adoption phase of an exercise
program, less structure in daily sessions may elicit greater levels of enjoyment. This may facilitate
compliance to an exercise program in the short-term and ultimately the development motivation for long-
term adherence to exercise (Motschiedler,& Coutts, 2010).
To increase self-worth and long-term adherence to physical activity, exercise and fitness
professionals use strategies like: (a) increasing motivation and enjoyment relative to activity, (b) making
activity a high priority in a woman's life, (c) improving or deemphasizing body image, (d) increasing a
woman's ability to access support, and (e) facilitating the use of self-regulation strategies (Huberty,
Ransdell, Sidman Flohr & Shultz, 2008).
Adherence to exercise in women with breast cancer is challenged by internal and external
conditions and may be improved by attention to the impact of treatment side effects and by supporting
patient self-efficacy towards changing health behavior (Husebø, Karlsen, Søreide & Bru, 2015).
Support from health care practitioners can promote patients’ autonomous motivation and greater
long-term behavioral persistence (e.g., adherence to physiotherapists’ recommendations) (Lonsdale, Hall,
Williams, McDonough & Ntoumanis, 2012).
We believe that a group-based intervention may yield better results compared to individualized
program as it may enhance social support and increase skills in building relationship between members of
the group (Azizan, Justine & Chua, 2013).
First, the physical activity program should be physically attainable and encouraging for the
participant. In contrast to many group-based physical activity programs found in literature, home-based
physical activity programs provide an opportunity to tailor the exercise to the participant. Individual
tailoring is a means to ensure practical attainability. Such customization can be quite extensive, giving
each participant his or her own specific training conditions. It can also be more structured, by providing
levels of exercising and allowing the patients to progress through these levels at their own pace. In this
study, structured individual tailoring is provided in order to keep the exercise program well-defined
(Geraedts, Zijlstra, Zhang, Bulstra & Stevens, 2014).
2.The aim of this study
The aim of this study is to observe a possible association between engaging in an exercise program
and the general state of health including physical, psychological and kinetic condition of the patients who
had undergone breast surgery for cancer.
3.Research methods (Matherials and Methods)
This study was carried out on 30 patients with breast cancer following mastectomy and axillary
lymph node dissection in the Surgery Unit of the Institute of Oncology from Cluj-Napoca. In our study
we applied two questionnaires: The Rotterdam Symptoms Checklist (De Haes, van Knippenberg & Neijt,
1990; de Haes, Olschewski, Fayers, Visser & Cull, 1987) and A Brief Self-Report Questionnaire
(Ridgers, Timperio, Crawford & Salmon, 2012).
The Rotterdam Symptom Checklist (RSCL) is a well-known instrument for the assessment of
symptom-related distress among cancer patients. We applied the RSC the day 1 after surgery. This
questionnaire consists of 39 items: 23 items referring to different physical symptoms, 7 items referring to
psychological distress, 8 items regarding functional status and an item regarding overall valuation of life.
We also applied A Brief Self-Report Questionnaire which contains two questions, after we
obtained the written approval of senior researcher, Nick Ridges (Centre for Physical Activity and
Nutrition Research (C-PAN), School of Exercise and Nutrition Sciences). This questionnaire was applied
in the Validity of a brief self-report instrument for assessing compliance with physical activity guidelines
surgery, after one, three and six months.
3.1 Ethical standards
We mention that the patients provided signed informed consent prior to inclusion in the study, and
that the study was approved by the Committee on Ethics in Research of this institution.
3.2 Statistical analysis
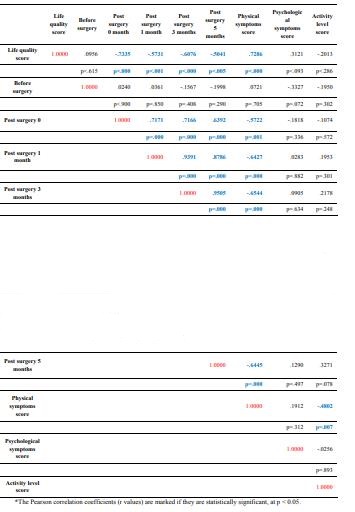
The statistical analysis was done using the
between the analyzed data block of data was probed using the Pearson coefficient r, together with normal
distribution assessment and a correlation matrix was generated to centralize the values. The statistical
level of significance was set to be p = 0.05.
4.Findings (Results)
The results of our study show a significant negative correlation between “Life quality score” and
“Post surgery 0 months” (r = -0.7335, p<0.000), as it is shown in Table 1 and Figure
quality of life is perceived by the patient, the higher is the patient’s adherence immediately after breast
surgery for cancer. Informing patients about the benefits of the recovery exercise program is essential for
obtaining patient’s adherence. It is extremely important that patients and their families to know that
complete recovery in range of motion of the shoulder after breast surgery is possible. Discussions with a
clinical psychologist may be very useful in finding self-determination and obtaining their adherence to the
exercise program.
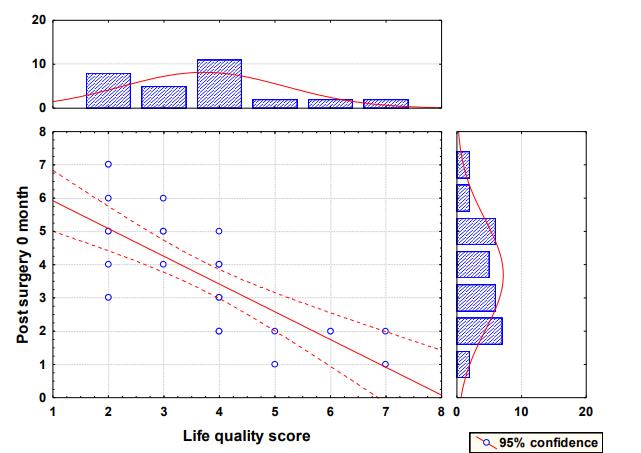
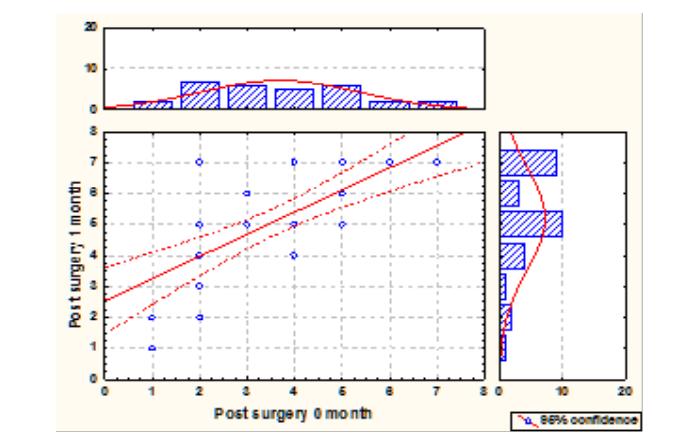
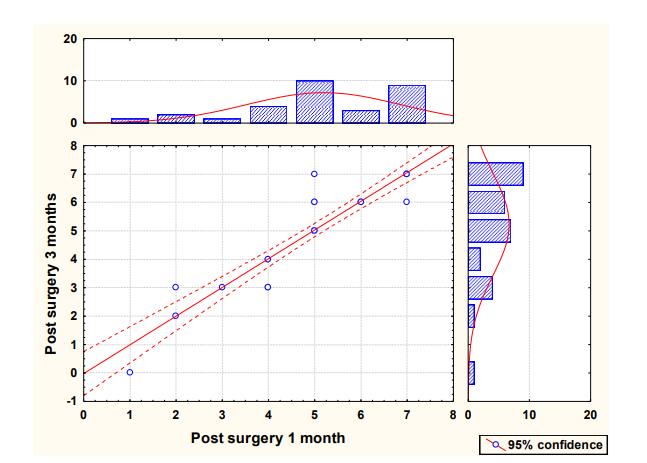
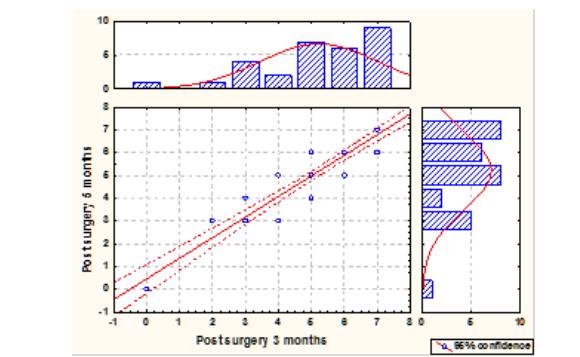
The 95% confidence interval is marked in dotted line. The distribution of the values of the
variables are plotted on the right and top axes respectively as histograms with normal distribution fitting.
Important positive correlation is observed in adherence to the recovery exercise program
immediately after surgery and in 1, 3 and 6 months after mastectomy, as it is shown in Figure
and Figure
surgery is, the higher the chance is to be high also after 1, 3 and 6 months.
There is a correlation between how the patients evaluate their life’s quality and the psychological
symptoms they have after surgery. The fact that results from statistical analysis doesn’t highlight a
correlation between life quality score and physical symptom score, indicates that patients from our study
evaluate their quality of life based mostly on the presence or the lack of psychological symptoms like
irritability, worrying, depressed mood, nervousness, despairing about the future, tension, anxiety, despite
physical symptoms like lack of appetite, soreness, pain, dizziness, tension, nausea, tiredness, digestion
problems.
The ability of taking care of herself and perform activities of daily living correlates with the life
quality score, as it is shown in the Table 1 (activity level score and life quality score). It is very important
for the patient that they regain their independence in keeping body hygiene, housework, shopping,
walking and climbing stairs by herself.
Psychological state of the patient influences her activity score and vice-versa, return to the daily
activities improves the psychological symptoms by regaining independence, trust and enhanced self-
motivation.
5.Conclusions
The evaluation of the overall state of health of the cancer patients after surgery and their activity
level is important in determining their future adherence to the exercise program and the success of the
recovery program.
According to the data from our study, the higher adherence at moment zero post surgery is, the
higher the chance is to be high also after 1, 3 and 6 months.
It is important that patients benefit from psychological support and counseling to find and
enhanced self-motivation for starting the exercise program, considering that patients evaluate their quality
of life based mostly on the presence or the lack of psychological symptoms, despite physical symptoms.
Extensive information about the benefits of the exercise program of the patients who evaluate their life
quality score as poor and obtaining their families’ support is the key in accomplishing the best results
with the recovery exercise program.
Psychological state of the patient influences her activity score and vice-versa, return to the daily
activities improves the psychological symptoms.
Acknowledgements
The authors would like to thank all patients for taking time and completing the questionnaire.
References
- and adherence to dietand exercise among hypertensive patients at the Mexican Institute of Social).
- Security IMSS). Value Health, 17(3):A120, doi: 10.1016/j.jval.2014.03.697
- Azizan, A., Justine, M., Chua, S. K. (2013). Effects of a behavioral program on exercise adherence and exercise self-
- efficacy in community-dwelling older persons. Curr Geront Geriatr Res, doi:10.1155/2013/282315
- Breast Cancer Surv Early physiotherapy afterbreast cancer surgery improves overall quality of life.
- (2005). Obesity, Fitness & Wellness Week, 112
- Cadmus-Bertram, L., Irwin, M., Alfano, C., Campbell, K., Duggan, C., Foster-Schubert, K., Wang, C.Y.
- et al. (2014). Predicting Adherence of Adults to a 12-Month Exercise Intervention. J. Phys Activ Health, 11(7) Chung, C. W., Lee S., Hwang S. W., Park E. H. (2013). Systematic Review of Exercise Effects on Health Outcomes in Women with Breast Cancer. Asian Nurs Res, 7(3):149-159.
- doi:10.1016/j.anr.2013.07.005 Courneya, K. S., Friedenreich C. M. (1997). Relationship between exercise during treatment and current quality of life among survivors of breast cancer. J Psychosoc Oncol, 15(3/4), 35-57 Cuevas,B. T., HughesD. C., Long Parma D., Treviño-Whitaker R. A., Ghosh S., Li R. et al. (2014).
- Motivation, exercise, and stress in breast cancer survivors. Support Care Cancer 201322:2038, doi: 10.1007/s00520-013-2038-6 de Haes, J. C., Olschewski, M., Fayers, P., Visser, M., Cull, A., Hopwood, P et al. The Rotterdam Symptom Checklist (RSCL): A manual. Second revised edition, UMCG / University of Groningen, Research Institute SHARE, 1987 de Haes, J. C., van Knippenberg, F. C., Neijt, J. P. (1990). Measuring psychological and physical distress in cancer patients: structure and application of the Rotterdam Symptom Checklist. Br J Cancer, 62(6):1034–1038 Gardner, C. L. (2014). Adherence: A Concept Analysis. Int J Nurs Knowledge. 26:96–101.
- doi: 10.1111/2047-3095.12046 Geraedts, H., Zijlstra, W., Zhang, W., Bulstra, S., Stevens, M. (2014). Adherence to and effectiveness of an individually tailored home-based exercise program for frail older adults, driven by mobility monitoring: Design of a prospective cohort study. Bmc Public Health, 14(1),570, doi:10.1186/1471-2458-14-570.
- Huberty, J. L., Ransdell, L. B., Sidman, C., Flohr, J. A., Shultz, B., Grosshans, O., et al. (2008).
- Explaining long-term exercise adherence in women who complete a structured exercise program. Res Quart, 79(3),374-84 Husebø, A. M. L., Karlsen, B. A. H., Søreide, J. A., Bru, E. (2015). Factors perceived to influence exercise adherence in women with breast cancer participating in an exercise programme during adjuvant chemotherapy: a focus group study. J Clin Nurs, 24:500–510, doi: 10.1111/jocn.12633 Jurkiewicz, M. T., Marzolini, S., Oh, P. (2011). Adherence to a home-based exercise program for individuals after stroke. Top Stroke Rehabil, 18(3):277-284. doi:10.1310/tsr1803-27 Kohlstedt, S. S., Weissbrod, C. S., Colangelo, A.M., Carter, M. M. (2013). Psychological Factors Influencing Exercise Adherence among Females. Psychology, 4(12) :917-923
- Lonsdale, C., Hall, A.M., Williams, G. C., McDonough, S. M., Ntoumanis, N., Murray, A., et al. (2012).
- Communication style and exercise compliance in physiotherapy (CONNECT). A cluster randomized controlled trial to test a theory-based intervention to increase chronic low back pain patients adherence to physiotherapists recommendations: Study rationale, design, and methods. BMC Musculoskel Dis, 13(1),104-104, doi:10.1186/1471-2474-13-104 Motschiedler, M., Coutts, M. (2010). The influence of exercise program structure on motivation and adherence. J Sci Med Sport, 13(1): e28-e29, doi:10.1016/j.jsams.2010.10.521 Perri, M.,G., Anton, S.D., Durning, P.E., Ketterson, T.U., Sydeman, S. J., Berlant, N. E., et al. (2001).
- Adherence to exercise prescriptions: Effects of prescribing moderate versus higher levels of intensity and frequency. Health Psychol, 21(5):452-458, doi:10.1037//0278-6133.21.5.452 Picorelli, A. M. A., Pereira, L. S. M., Pereira, D. S., Felicio, D., Sherrington, C. (2014). Adherence to exercise programs for older people is influenced byprogram characteristics and personal factors: a systematic review. J Physiotherapy, 60(3):151 – 156, doi: 10.1016/j.jphys.2014.06.012 Ridgers, N. D., Timperio, A., Crawford, D., Salmon, J. (2012). Validity of a brief self-report instrument for assessing compliance with physical activity guidelines amongst adolescents. Journal Sci Med Sport, 15(2), 136-141, doi:10.1016/j.jsams.2011.09.003 Rizzo, J. (2015). Patients' mental models and adherence to outpatient physical therapy home exercise programs. Physiotherapy. 31(4): 253-259, doi: 10.3109/09593985.2014.1003117 Shakudo, M., Takegami, M., Shibata, A., Kuzumaki, M., Higashi, T., Hayashino, Y. et al. (2011). Effect of feedback in promoting adherence to an exercise programme: a randomized controlled trial. J Eval Clin Pract, 17:7–11, doi: 10.1111/j.1365-2753.2009.01342.x Swenson, K. K., Nissen, M. J., Henly, S. J. (2010). Physical Activity in Women Receiving Chemotherapy for Breast Cancer: Adherence to a Walking Intervention. Oncol Nurs Forum, 37.3, 2010:321-30 Thurston, M.; Green, K. (2004). Adherence to exercise in later life: how can exercise on prescription programmes be made more effective? Health Promot Int, 19 (3):379-387, doi: 10.1093/heapro/dah311 Uc-Coyoc, R.O., Coello-Reyes, L. A., Perez-Reynaud, A. G., Ponce, R. D. (Drug prescription Whellan, D. J. (2012). Long-Term Exercise Training and Adherence. J Am Coll Cardiol, 60(16):1529-1530. doi:10.1016/j.jacc.2012.07.018
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
25 May 2017
Article Doi
eBook ISBN
978-1-80296-022-8
Publisher
Future Academy
Volume
23
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-2032
Subjects
Educational strategies, educational policy, organization of education, management of education, teacher, teacher training
Cite this article as:
Puscas, D., Achimas-Cadariu, P., Vlad, C., Pop, F., & Tache, S. (2017). Adherence to Recovery Exercise Program of Scapulohumeral Articulation After Breast Cancer Surgery. In E. Soare, & C. Langa (Eds.), Education Facing Contemporary World Issues, vol 23. European Proceedings of Social and Behavioural Sciences (pp. 69-78). Future Academy. https://doi.org/10.15405/epsbs.2017.05.02.10