
Health behavior in the context of perceived social support in late adolescence


Abstract
The presented study is a part of a grant research project: "Health-enhancing and health-threatening behavior: determinants, models and consequences" (n° 13-19808S). It follows up on the results of foreign research on possible connections between health behavior and the perceived level of social support. The primary aim was to identify the key components of health behavior in the developmental stage of late adolescence, map their relation to perceived social support and to explore if there are also some possible significant gender differences in health behavior or in perceived social support of adolescents which would be projected into their health behavior. The quantitative research design based on one-time questionnaire survey was used to carry out the research. Health behavior was assessed by the Health behavior scale, and the level of social support was assessed by the Close relationships and social support scale. The research file contained 825 adolescents aged 15-19 years (the average age was 16.89 years and the median was 17 years); there was a slight predominance of women (457 − 55.4%) over men (368 − 44.6%). By carrying out factor analysis of Health behavior scale, 4 factors explaining the 35.2% of the overall spread were extracted and they were named as: 1. Healthy eating; 2. Health protection; 3. Positive thinking; and 4. Illness prevention. In most of these factors, statistically significant gender differences were found, which are reflected in the reported health behavior. The results have demonstrated that two of the identified components of health behavior − Positive thinking and Illness prevention − are in a positive manner statistically significantly related to the level of perceived social support. Also differences in perceived social support in the given developmental stage have been mapped, and the highest level of social support has been found in 18-year-old respondents. The results of the study highlight the importance of future research in the area of studying the mechanism of impact that perceived social support has on the reported health behavior and the changes of this relationship in ontogeny.
Keywords: Perceived social supporthealth behavior
Introduction
From historical as well as current perspectives, the scope of view on health differs significantly in individual authors − from definitions of health as mere lack of illness (Brannon & Feist, 2009) to a very broad context of intervening variables by which health is described (Rohleder, 2012; Rosen & Imperato, 2015). Even the definition of health itself has undergone a complicated evolution from a purely biological perception of the notion of health, to the integration of social and later also psychological perspective, and now based on holistic foundation, reflecting the dynamics of health condition development in time (at the level of ontogeny of an individual and the development of changes on the scale between health and illness) as well as systemic approach to health in all its key connections, based on the principles of circular causality. Even individual models of health (pathogenic model, biomedical model, social ecological model, behavioral model, holistic model, etc.) overlap and complement each other in the perception of various authors and their approaches. Current process-oriented definitions of health define it in the bio-psycho-eco-social context as a sufficient competence of a system to cope with pathogenic factors and control them effectively thanks to self-regulatory processes. In the context of current approach to health, Egger (2013) defines it as a sufficient competence of an individual to cope with whatever stressful inconvenience at any level of an incessantly changing system through self-regulation. In this understanding, health is not a result of a mere lack of pathogens and does not even mean a lack of psychological stresses or conflicts, but represents the ability of an individual to sufficiently control the above mentioned factors, and thus it is rather perceived as one´s own power (resilience or self-regulatory power). Health is therefore perceived by current specialists mainly as an unceasingly ongoing dynamic action conditioned by many circumstances, especially by the manner in which an organism manages to adjust to changing demands of the outer and the inner environment. We can therefore understand health not only as the present state but rather as a continual process, which is realized in the context of biological and personal dispositions and social relationships, and it is closely related to many other psychosocial and environmental phenomena. Especially in adolescence, social support has a quite fundamental impact on health behavior, which in the end causally influences health.
Adolescence is the key period for forming, strengthening and developing of desirable habits in the area of health behavior (Becker & Arnold, 2004; Sawyer et al., 2012) when the responsibility for one´s health, demonstrated by following desirable hygiene practices and fundamental principles of desirable health behavior, gets transferred from parents to adolescents. The study of health-enhancing behavior and lifestyle in adolescents from North Indian City draws attention to the fact that some health-enhancing types of behavior (physical exercise and healthy diet), but also those health-damaging ones (smoking and use of alcohol) adopted and adapted in the period of adolescence are often preserved until late adulthood (70% of deaths has its roots in the habits related to health behavior solidified in this crucial developmental stage (Raj, Senjam, & Singh, 2013). As opposed to later life periods, this stage also involves more health-threatening behavior and risky attitudes to one´s own health (Haskell et al., 2007; Lerdal, Celius, & Pedersen, 2013). That is why the importance of influence of social support on an individual´s health raises in this stage of development, since, apart from its indirect influence, it can be also significantly demonstrated by its direct influence during adolescence − e.g. by mutual sharing of values and attitudes to health, or displaying health-enhancing behavior in a suitable referent social group.
Health behavior
An important role in health behavior practiced by an individual is played by key personality disposition factors as well as cognitive factors (Otonari et al., 2012; Allen, Vella, & Laborde, 2015), the type of parenting in the family, models in one´s social environment, etc. (Lippke, Nigg, & Maddock, 2012), which are in the end combined. Health behavior can thus move on the continuum from health-enhancing behavior (e.g. regular adequate physical activity or healthy diet) to health-threatening behavior (e.g. excessive physical activity, or restrictions in food, or overeating). In various phases of development of each individual, on the one hand, up to a certain degree, there are protection factors in health behavior (such factors of behavior which have positive influence on health). On the other hand, appear risk factors, or negative factors (which have negative influence on health in their consequence). Some of these factors cannot be simply classified in only one of these categories and most of them do not even influence health unilaterally, but they can influence it in both positive and negative manners.
The authors Flay & Petraitis based their relatively complex health behavior theory, Theory of Triadic Influence, on the assumption that individual variables can be organized at various levels of their influence on health behavior (Flay, Snyder, & Petraitis, 2009), and they are sorted into three basic areas, which to a certain extent correspond with fundamental determinants of health: 1. Intrapersonal influences (qualities contributing to self-efficacy related to behavior; 2. Interpersonal influences (social context contributing to the formation of a belief of particular behavior); and 3. Culturally-environmental influences (socio-cultural context forming attitudes to particular behavior). Some of the above mentioned variables have direct influence on health, and therefore are its immediate cause (for example an intention). Others are mediated by other variables − they are therefore more distal and at the same time also predisposing. Social support is then classified as a direct influence.
Social support
Social support expresses the state when people who have something in common provide help to each other. This could mean sharing a household, school, workplace, membership in an organization or a place of stay, and it includes the awareness of an individual that people in his or her social environment are ready to help (Ferlander, 2007). Brannonová & Feistová (2009) postulate that social support refers to a variety of material and emotional support which we receive from others. What they see as its opposite is social, or societal, isolation, or the absence of specific and meaningful relationships. In a broader context, social support is perceived and assessed in the context of society, when individuals from various social spheres can have differing conditions in reaching health care and possibilities of learning about their health condition (Lourel et al., 2013). A term superior to social support is a social network, which represents connectedness and links among social relationships surrounding an individual (Heaney & Israel, 2008).
A rather complex view of the influence of social support on health behavior was presented by Umbersonová, Crosnoe & Reczek (2010), who managed to construct a Model of social links to health behavior, based on the analysis of present studies. Their model shows that social relationships can influence health behavior in two basic manners: directly and indirectly − and there are a great number of indirect influences. Social relationships can influence, for instance, even norms and symbolic meanings of health for an individual, and thus can instill in him or her, for example, a norm of responsibility for one´s own health, which in combination with raising self-control can lead to preventive, health-enhancing behavior. In case of insufficient social support, such mechanisms of behavior can start working which are not health-enhancing in their consequence, e.g. use of narcotic drugs, which is related to escapist strategies in terms of coping with stressful (intrapsychic and interpersonal) situations. However, health-threatening, or risky forms of behavior can be even influenced when a sufficient amount of social support is provided − in connection with adopting inadequate models of behavior of a referent group (Umberson, Crosnoe, & Reczek, 2010).
Social support in adolescence
As it was stated before, a great number of influences play a role in forming health behavior in adolescents (Sawyer et al., 2012), and active building of strong friendships and the influence of friends, intimate partners, and close referential groups become more and more important in this developmental stage (Helsen, Vollebergh & Meeus, 2000). Social relationships are undoubtedly one of the important aspects of lives of teenagers, who use them to seek and consolidate their position in the society, lifestyle, abilities, and many other important conditions for becoming adults. They also use them to look for support and understanding for their models, norms, aspirations and behavior. Their peers have a strong influence even on adolescents´ health behavior, and many studies illustrate both positive and negative aspects of such an influence. Camara, Bacigalupe and Padilla (2014) carried out qualitative research of the role of interpersonal relationships in adolescents and they reached the conclusion that adolescents perceive interpersonal relationships as a source of stress and conflicts as well as a source of support. The positive signs of social support most frequently reported by adolescents are trustworthiness, maturity and friendly attitude, and they consider social support the most important of all. During late adolescence, the social network is restructured, and the central position becomes occupied by peers as well as parents. If an adolescent perceives his or her peer social support as more important, parents´ influence can decrease (2013). A significant role in the social network of adolescents can be played by school environment, where social support is mediated by interpersonal relationships (Reddy, Rhodes & Mulhall, 2003; Turner & Patrick, 2004; Cotterell, 2007) and also by another referent group.
The influence of social support on health
As it has been stated above, social support has an undeniable influence on health and health behavior of adolescents − in both positive and negative sense. The connections between social support (perceived, or actually provided) and the reported health behavior has been explored in many contexts by a number of research studies. The newest studies of the significance of social support did not substantially differ from the previous ones in their results (Viner et al., 2012). Kahneman & Krueger (2006) summarize the conclusions of the studies on well-being, and state that people are simply happier and more content when they are close to other people, which is in its consequence reflected in their attitudes and expectations as well as health behavior. Carter et al. (2007) arrived at the conclusion that adolescents with many friends use safety equipment more actively and more often prevent illnesses. The connections between risky behavior and the influence of peers was studied, for example, by Gecková & Van Dijk (2001), who concluded that the more friends who support and practice risky behavior an adolescent has, the bigger possibility there is he or she will start to behave in the same manner. Potard, Courtois & Rusch (2008) describe the influence of peers on the riskiness of sexual relationships of adolescents − those surrounded by more sexually active individuals start to seek intimate activities earlier than they would on their own, and if there are peers who prefer random sexual relationships in their surroundings, they are probably more likely to look for such activities than if they were only surrounded by individuals with more conventional preferences. Social support also indisputably plays an important role in the context of health behavior in the so called risky phases of ontogeny, such as adolescence. Cheng et al. (2014) have demonstrated a lower level of depression, suicidal tendencies, and less serious post-traumatic stress symptoms in adolescents who have received adequate social support from their family and surroundings. Gecková et al. (2003) in this context state that consistent social support has a great influence on the overall quality of life of adolescents, and those who have nobody to turn to describe their physical and mental health as worse than those who have somebody close to them.
Problem statement
The study is a part of an extensive grant project "Health-enhancing and health-threatening behavior: determinants, models and consequences", whose primary research aims cover the following areas: Optimism model and its relation to health behavior; Health-enhancing and health-threatening behavior model; Neuropsychological markers of health-enhancing behavior and neuropsychological markers as indicators of health-threatening behavior; and Age as a mediator of key influences projected into health behavior. The last research topic included cross-selectional research, which helped to describe and compare health behaviors and mapped its fundamental intrapersonal and interpersonal influences from adolescence to old age, highlighting the identification of main health-enhancing behavior predictors for individual stages of ontogeny. In accordance with the current psychological approaches to health, which find it important to link individual aspects of health and see it as a whole (Coleman, Hendry, & Kloep, 2007), the presented study maps the level of perceived social support in late adolescence and its impact on health behavior.
Purpose of the study
The study therefore explores possible connections between health behavior and the perceived level of social support in late adolescence, since, as well as other authors, we regard this developmental stage not only as crucial but also critical in creating, developing and solidifying habits in health behavior (Blatný et al., 2006; Bonino, Sawyer et al., 2012). Adolescents are especially sensitive to external incentives, and environmental factors like family, school, peers or social institutions can either support or undermine their approach to health. Moreover, in adolescence, strong friendships are created and the influence of peers and close friends and gradually also partners becomes more and more important (Helsen, Vollebergh, & Meeus, 2000). The presented study is based on conclusions of Umberson, Crosnoe & Reczek (2010), who claim that social support positively influences health of individuals and is an integral part of their healthy lifestyle not only during adolescence but also during their whole lives.
Research questions
Based on the above mentioned theoretical standpoints, the research part of the study aimed to map the relationship between perceived social support and health behavior in the given developmental stage, and also possibly determine in which components of health behavior this relationship is demonstrated. We have also monitored whether there are any gender differences in health behavior between adolescents and in perceived social support. Moreover, we have paid attention to possible differences in perceived social support in the context of late adolescence.
Research methods
With regard to the aim of the research and the formulated hypotheses, the quantitative research design was used, and it was carried out in the form of cross-selectional research with the use of one-time questionnaire survey. It was a correlation and partly also comparative study, which was searching for the connections between health behavior and the level of perceived social support in the developmental stage of late adolescence. The methods used were based on subjective statements of respondents about their behavior (see further). The research team administered the questionnaire battery in selected schools using the paper-pencil method, and it took one lesson (45 minutes) to fill in the questionnaire, which was entirely anonymous. For ethical reasons, only those students who provided informed agreement to participate in the study (signed by their parents) took part in the research. The respondents had the right to withdraw from the research study and after the data had been analyzed, school leaders and individual classes participating in the research were informed about the results by educational advisors.
Research file
The research file contained 825 adolescents with the average age of 16.89 years and the median of 17 years. There were 139 (16.8%) fifteen-year-old adolescents, 189 (22.9%) sixteen-year-old adolescents, 220 (26.6%) seventeen-year-old adolescents, 174 (21.2%) eighteen-year-old adolescents and 103 (12.5%) nineteen-year-old adolescents in the research file. There were 457 (55.4%) women and 368 (44.6%) men − the respondents were chosen by conventional sampling method.
Methods used
The respondents were asked to provide basic demographic data (sex, age, nationality and type of school attended). In order to observe health behavior, Health behavior scale (Slováčková, Klimusová & Dosedlová, 2013) was employed, which uses 42 items assessed on a five-level Likert-type scale to map individual areas of lifestyle and preventive healthcare (eating, drinking, sleep, regular daily regime, level of physical activity, use of addictive drugs, preventive measures and selected elements of mental hygiene). The inner consistence reliability of the test was verified by Cronbach alpha quotient (0.85).
In order to map the perceived level of social support, the Close relationships and social support scale was used (Cefai & Camilleri, 2009), which is a part of an extensive test battery created by authors for determining physical and mental health, social and emotional well-being, and aspects of academic life in university students. Seven items of the scale aim to determine the number of close persons as well as the level of content with relationships, and to identify the feeling of loneliness (In order to verify the test´s reliability, the authors of the method used a test-retest with fifty randomly chosen university students. The test administration was done twice with a week´s gap. In order to determine the reliability, Pearson´s correlation was used, which varied between 0.78 and 0.96 in individual variables − based on these values, we found the test sufficiently reliable.) . When filling in the questionnaire, there was a possibility to choose one out of four or five options in most of the questions, and in one question, respondents could mark their answers on a four-point scale from "easy" to "very difficult". The authors of this method claim that its Cronbach´s alpha is between 0.78 and 0.96. The inner reliability consistence of the scale verified by Cronbach´s alpha was determined as 0.58 for the research data of the presented study. This value is relatively low and shows a rather low reliability of the test, which could have been caused by the isolated use of the scale.
Findings
The demographic data was processed with the help of descriptive statistics. The respondents who took part in the research were students of grammar schools (18.7%), high schools (40.9%) and the last years of elementary schools (10.3%). The information about the type of studies was not filled in by 248 (30.1%) respondents. As regards their place of residence, the respondents mostly stated a village − in 394 cases (47.8%) and then 232 (28.1%) of them stated that they live in a small town up to 20 thousand inhabitants, 105 of the respondents (12.7%) stated that they live in a relatively big town up to 100 thousand inhabitants, 43 (5.2%) in a big town up to 500 thousand inhabitants, and only 4 (0.5%) stated their place of residence was a city which has more than 1 million inhabitants (The information about the place of residence was not provided by 8 respondents.) . In the results presented below, the respondents do not differ in either type of school or the reported place of residence.
Health behavior
With the help of factor analysis, the final components of health behavior were reduced from the Health behavior scale to 4 factors, which were defined by Scree Plot. To extract individual items, rotation Varimax was used. The extracted factors altogether explained 35.2% of the overall spread and were marked as:
1. Healthy eating (items related to eating, avoiding unhealthy food and eating healthy food fall into this group) − this factor on its own explains 10.2% of the overall spread;
2. Health protection (this factor contained items determining the use of safety equipment and adjusting of daily regime to one´s current state) − overall it explains 9% of the spread;
3. Positive thinking (questions related to mood and relationship to yourself and others, to ways of spending free time, and to stress were included here) − the factor explains 8.9% of the overall spread; and
4. Illness prevention (items determining the level of resistance to cold, mental hygiene and illness prevention were in this category) − the factor explains 7.1% of the overall spread.
Gender differences in health behavior
We were also interested in gender differences in individual extracted factors of health behavior from the Health behavior scale (Healthy eating, Health protection, Positive thinking, and Illness prevention). Therefore, we compared scores in individual factors between sexes and used T-tests for independent selections. By using Levene´s homogeneity test (F-test), we verified that the spreads in both observed groups can be considered the same. A statistically significant difference was found in the Healthy eating factor (t=-4.182; df=732; p<0.01) − the average value of males was -0.175 (N=312; sd=0.986) and the average value of females was 0.137 (N=398; sd=0.99), which shows that adolescent girls care about healthy eating more than adolescent boys. A statistically significant difference was also identified in the Health protection factor (t=-4.393; df=708; p<0.01) − the average value of males was
-0.184 (N=312; sd=1.039) and the average value of females was 0.144 (N=398; sd=0.944). Significant differences in these results demonstrate that adolescent women focus on health protection more than men. The last statistically significant difference appeared in the Positive thinking factor (t=-4.393; df=708; p<0.01) − the average value of males was 0.135 (N=312; sd=1.021), the average value of females was -0.106 (N=398; sd=0.971). Men from the research file in this developmental stage keep themselves in good mood and spend time in the company of their close friends more than women.
The relationship between social support and health behavior
So as to be able to work with the results of perceived social support as with one factor, we combined all the seven items of the Close relationships and social support scale, and thus computed the overall reached score in social support for each individual. The method was completed by all the 825 respondents − the minimal score was 3 points and the maximal score was 29. The lowest value was 4 points and it was reached by one individual. The highest value was 29 points and it was reached by 4 individuals. Therefore, only a minimal number of respondents reached extreme values in perceived social support. The average of the values was 19.8 (SD=4.3) and the modus was 20 (10.1%). Most respondents scored around the average.
Afterwards, when processing the data, we used correlation analysis to determine the level of closeness of the relationship of perceived social support and the four factors extracted from the Health behavior scale. The distribution of the observed file was normal, so we used Pearson´s correlation coefficient to quantitatively express closeness of the relationship. There was a statistically significant relationship only in two factors of health behavior. From all the factors, the Positive thinking factor correlated most strongly with perceived social support (N=720, r=0.394, p<0.01). This relationship was medium strong in individuals who stated a higher level of perceived social support and the reported health behavior component Positive mood. The second factor in which a relationship with perceived social support was demonstrated was Illness prevention (N=720, r=0.113, p<0.01). This relationship was shown as not very close, but it cannot be denied. Contrary to our assumptions, no statistically significant relationship appeared between other factors (Healthy eating and Health protection) and the level of perceived social support (see Table
Gender differences at the level of perceived social support
We used T-test for independent selections to verify these relationships. In order to verify the match of spreads in both genders, we did Levene´s homogeneity test again, which turned out to be statistically irrelevant − therefore we could not prove any significant difference between men (t=-0.576; df=823; p>0.05) and women (t=-0.571; df=758.2; p>0.05) at the level of perceived social support.
Differences in levels of perceived social support in late adolescence
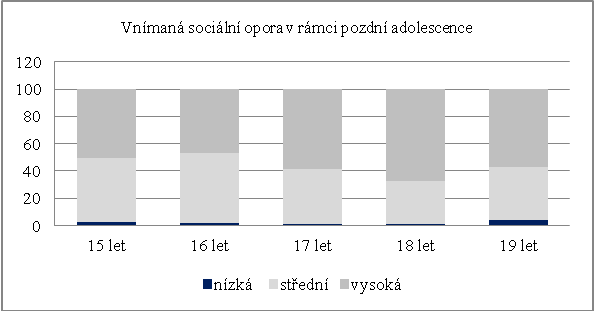
When mapping possible differences in levels of perceived social support in the developmental stage of late adolescence, we focused on the classes of 15-year-old (N=139), 16-year-old (N=189), 17-year-old (N=220), 18-year-old (N=174) and 19-year-old (N=103) adolescents. We determined the existence of differences between these classes with the help of Chi-squared test. By adding the scores of variables in individual respondents on the Close relationships and social support scale, we gained the total score of social support for each respondent. Subsequently, we used the Compute Variable function to create three groups and further worked with perceived social support divided into three variables: Low level of social support (score 3-11 points); Medium level of perceived social support (score 12-20 points); and High level of perceived social support (score 21-29 points). It turned out that the difference in levels of social support between individual classes is statistically significant (χ2=24.77; df=12; p<0.05) and that individuals who were 18 years old showed the highest level of social support.
Perceived social support in late adolescence
Limits
One of the fundamental limits of the study surely is the use of conventional sampling method. This manner of respondent selection does not guarantee even distribution of the sample with the tested population. Nevertheless, a more appropriate method (e.g. random selection) would not secure such an amount of research data in the same time period and it would be substantially more financially demanding. Following the ethics of research also entails some further limitations (only those participants took part in the research who wished to participate). Moreover, some other limits were caused by the use of self-evaluation questionnaire methods and a rather low reliability of the Close relationships and social support scale.
Conclusions
By carrying out factor analysis of the Health behavior scale, 4 factors, explaining 35.2 % of the overall spread, were extracted, and named as: 1. Healthy eating; 2. Health protection; 3. Positive thinking; and 4. Illness prevention. These factors correspond with individual components of health behavior, as they are described by many authors (Steptoe & Wardle, 2004; Brannon, Feist & Updegraff, 2014). Statistically significant gender differences, which are reflected in the reported health behavior, were found in most of these factors. Adolescent women, for example, care more about healthy diet than men. This result is in agreement with the results of the study by McCabe and Ricciardelli (2001), who postulate that girls watch their diet more and avoid unhealthy food due to the current cult of beauty, which puts more pressure on them than on boys (see also Ata et al. 2007). A statistically significant difference between male and female sex also turned out to be in the Health protection factor. Women are more focused on health protection, which is reflected in their use of safety equipment when doing sport or using means of transport, adjusting their daily regime to their current health condition and protecting themselves against sunshine. This result is in accordance with conclusions of other authors, who ascribe women greater conscientiousness in their attitude to health, which is reflected in their health behavior (Ghanbarzadeh & Mohamadi, 2012; Mathur, Stigler, Erickson, Perry, & Forster, 2014). The last statistically significant gender difference in health behavior appeared in the Positive thinking factor. In this case, the result shows that men, as opposed to women, keep themselves in good mood and spend their time in the company of their close friends. Bothmerová a Fridlund (2005) in this context state that adolescent girls are much more often stressed and face more mental stress than adolescent boys. It is therefore possible that this fact prevents them from keeping themselves in a good mood and positively disposed. There was no significant gender difference in the Illness prevention factor in the reported health behavior, which is displayed as, for example, regular building of resistance to cold, keeping one´s diet balanced, regular relaxation and mental hygiene, etc. Therefore, no differences have been found between respondents, which is probably caused by the attitude of both sexes to preventive health measures following from the given developmental stage, when most of them feel in very good physical condition and do not feel the need to care about prevention, which requires a considerable amount of self-regulation, since these activities need to be performed regularly and long-term (Harris & Jenkins, 2006; Steptoe, Wright, Kunz-Ebrecht, & Iliffe, 2006).
The presented results further lead us to the conclusion that perceived social support influences certain aspect of health behavior in adolescents. A statistically significant positive relationship was confirmed in respondents between perceived social support and some components of health behavior, namely, Positive thinking (including a positive attitude to oneself, relaxation, spending time with friends and keeping oneself in a good mood) and Illness prevention (partially including also mental hygiene and building up resistance to cold) − even though in this case the relationship was weaker. In this context, Kahneman & Krueger (2006) claim that people are happier if they perceive social support from their surroundings, which is in its consequence reflected in their attitudes to and expectations about health as well as in their health behavior. In the Healthy eating factor, no statistically significant relationship was found, which corresponds with the conclusions of Fitzgerald et al. (2013), who states that peer support causes a more frequent consumption of unhealthy food, specifically fast food and sweets. Considering that the compared Healthy eating factor mostly consisted of questions about consumption of fried meals, sweetened lemonades and eating in fast food restaurants, it is possible that individuals who scored high (i.e. they avoided such unhealthy food and drinks) had a lower social support. Also the relationship between social support and the Protection of health factor was statistically insignificant. Similarly, no statistically significant gender differences have been found in the level of social support, but it is possible that this result was influenced by unidirectionally oriented questions on the Close relationships and social support scale. We also found out that there are differences in perceived social support in the context of the given developmental period − the highest level of social support was demonstrated by 18-year-old respondents. It is possible that at this breakthrough age, which is in the Czech republic considered the beginning of maturity, respondents gain social support not only from their parents and friends but also from their romantic partners, since interest in intimate relationships and searching for a suitable partner increases, and the age of first sexual experience is, on average, at this particular age (Wellings et al., 2001; Weiss & Zvěřina, 2009). Moreover, we should not forget that the age of 18 years is also the borderline for alcohol consumption and entrance to nightclubs where there are many opportunities to start new relationships.
The presented results prove the validity of researching mutual relationships between social support and health behavior, including relevant mechanisms of the given effect and developmental trends, and they can be incorporated into relevant intervention programs.
Acknowledgments
The study is a part of an extensive research project "Health-enhancing and health-threatening behavior: determinants, models and consequences", which started under the patronage of Grant Agency of the Czech Republic (no. 13-19808S).
References
- Allen, M. S., Vella, S. A., & Laborde, S. (2015). Health-related behavior and personality trait development in adulthood. Journal of Research in Personality, 59, 104-110.
- Ata, R. N., Ludden, A. B. & Lally, M. M. (2007). The Effects of Gender and Family, Friend, and Media Influences on Eating Behaviors and Body Image During Adolescence. Journal of Youth and Adolescence. 36(8), 1024-1037.
- Becker, C. M. & Arnold, W. (2004). Health Promoting Behaviors of Older Americans versus Young and Middle Aged Adults. Educational Gerontology, 30, 10, 835-844.
- Blatný, M., Hrdlička, M., Sobotková, V., Jelínek, M., Květoň, P., & Vobořil, D. (2006). Prevalence antisociálního chování českých adolescentů z městských oblastí. [Prevalence of antisocial behavior in Czech adolescents from urban areas.] Československá psychologie [Czechoslovak psychology], 50(4), 297-310.
- Bonino, S., Cattelino, E. & Ciairano, S. (2005). Adolescents and Risk: Behavior, Functions, and Protective Factors. Milano: Springer.
- Bothmer, M. I .K. von & Fridlund, B. (2005). Gender differences in health habits and in motivation for a healthy lifestyle among Swedish university students. Nurishing and Health Sciences, 7, 107-118.
- Brannon, L., & Feist, J. (2009). Health Psychology: An Introduction to Behavior and Health. Belmont, CA: Wadsworth.
- Brannon, L., Feist, J. & Updegraff, J. A. (2014). An Introduction to Behavior and Health, Eighth Edition. Belmont, CA: Cengage Learning.
- Camara, M., Bacigalupe, G. & Padilla, P. (2014). The role of social support in adolescents: are you helping me or stressing me out? International Journal of Adolescence and Youth, 1-14.
- Carter, M., McGee, R., Taylor, B. & Williams, S. (2007). Health outcomes in adolescence: Associations with family, friends and school engagement. Journal of Adolescence, 30(1), 51-62.
- Coleman, J., Hendry, L. B. & Kloep, M. (2007). Adolescence and Health. West Sussex: John Wiley & Sons Ltd.
- Cotterell, J. (2007). Social Networks in Youth and Adolescence. London: Routledge.
- Egger, J. W. (2013): Biopyschosocial Medicine and Health – the body mind unity theory and its dynamic definition of health. Psychologische Medizin, 24, 24 – 29.
- Ferlander, S. (2007). The Importance of Different Forms of Social Capital for Health. Acta Sociologica, 50(2), 115-128.
- Fitzgerald, A., Heary, C., Kelly, C., Elizabeth, N. & Shevlin, M. (2013). Self-efficacy for healthy eating and peer support for unhealthy eating are associated with adolescents food intake patterns. Appetite, 63, 48-58.
- Flay, B. R., Snyder, F. J., Petraitis, J. (2009). The Theory of Triadic Influence. In: Emerging theories in health promotion practice and research (2nd ed., pp. 451-511). San Francisco, CA: Jossey-Bass.
- Furman, W. & Buhrmester, D. (1992). Age and Sex Differences in Perceptions of Networks of Personal Relationships. Child Development, 63(1), 103-115.
- Gecková, A., & Van Dijk, J. (2001). Peer impact on smoking, alcohol consumption, drug use and sport activities in adolescents. Studia psychologica, 43(2), 113-121.
- Gecková, A., Van Dijk, J. P., Stewart, R., Groothoff, J. W. & Post, D. (2003). Influence of social support on health among gender and socio-economic groups of adolescents. European Journal of Public Health, 13, 44-50.
- Ghanbarzadeh, M., & Mohamadi, A. (2012). Aerobic exercise on mental health of prisoner people. Journal Of Physical Education & Sport, 12(2), 217-221.
- Harris, C. R., & Jenkins, M. (2006). Gender Differences in Risk Assessment: Why do Women Take Fewer Risks than Men? Judgment and Decision Making, 1 (1), pp. 48-63.
- Haskell, W., Lee, I., Russel. R., Powell, K., Blair, S., Franklin, B. et al. (2007). Physical Activity and Public Health. Medicine, 39(8), 1423-1434.
- Heaney, C. A. & Israel, B. A. (2008). Social networks and social support. In Glanz, K., Rimmer, B. K. & Viswanath, K. Health behavior and health education: Theory, Research and Practice. San Francisco: John Wiley & Sons.
- Helsen, M., Vollebergh, W. & Meeus, W. (2000). Social Support from Parents and Friends and Emotional Problems in Adolescence. Journal of Youth and Adolescence. 29(3), 319-335.
- Cheng, Y., Li, X., Lou, Ch., Sonenstein, F. L., Kalamar, A., Jejeebhoy, S., Delany-Moretlwe, S., Brahmbhatt, H., Olumide, A. O. & Ojengbede, O. (2014). The Association Between Social Support and Mental Health Among Vulnerable Adolescents in Five Cities: Findings From the Study of the Well-Being of Adolescents in Vulnerable Environments. Journal of Adolescent Health, 55(6), 31-38.
- Kahneman, D. & Krueger, A. B. (2006). Developments in the Measurement of Subjective Well-Being. The Journal of Economic Perspectives, 20(1), 3-24.
- Kenny, R., Dooley, B. & Fitzgerald, A. (2013). Interpersonal relationships and emotional distress in adolescence. Journal of Adolescence, 36(2), 351-360.
- Lerdal, A., Celius, E. H., & Pedersen, G. (2013). Prescribed exercise: A prospective study of health related quality of life and physical fitness among participants in an officially sponsored municipal physical training program. Journal of Physical Activity & Health, 10(7), 1016-23.
- Lippke, S., Nigg, C. R., & Maddock, J. E. (2012). Health-promoting and health-risk behaviors: Theory-driven analyses of multiple health behavior change in three international samples. International Journal of Behavioral Medicine, 19(1), 1-13.
- Lourel, M., Hartmann, A., Closon, C., Mouda, F., & Petric - Tatu, O. (2013). Social Support and Health: An Overview of Selected Theoretical Models for Adaptation. In: Social support and health: theory, research, and practice with diverse populations, pp. 2-19. Hauppauge, New York: Nova Science Publishers, Inc.
- Mathur, C., Stigler, M., H., Erickson, D., J., Perry, C., L., Forster, J., L. (2014). Transitions in smoking behavior during emerging adulthood: a longitudinal analysis of the effect of home smoking bans. American Journal of Public Health, 104(4), 715-20.
- McCabe, M. & Ricciardelli, L. A. (2001). Parent, peer, and media influences on body image and strategies to both increase and decrease body size among adolescent boys and girls. Adolescence, 36(142), 225-240.
- Otonari, J., Nagano, J., Morita, M., Budhathoki, S., Tashiro, N., Toyomura, K., & ...Takayanagi, R. (2012). Neuroticism and extraversion personality traits, health behaviors, and subjective well-being: the Fukuoka Study (Japan). Quality Of Life Research, 21(10), 1847-1855.
- Potard, C., Courtois, R. & Rusch, E. (2008). The influence of peers on risky sexual behavior during adolescence. The European Journal of Contraception and Reproductive Health Care, 13(3), 264-270.
- Raj, S., Senjam, S., Singh, A. (2013). Assessment of Health-Promoting Behavior and Lifestyle of Adolescents of a North Indian City. International Journal of Preventive Medicine, 10(4), 1189-1194.
- Reddy, R., Rhodes, J. E. & Mulhall, P. (2003). The influence of teacher support on student adjustment in the middle school years: A latent growth curve study. Development and Psychopathology, 1, 119-138.
- Rohleder, P. (2012). Critical Issues in Clinical and Health Psychology. London: SAGE.
- Rosen, G. & Imperato, P. J. (2015). A History of Public Health: Revised Expanded Edition. Baltimore: Johns Hopkins University Press.
- Sawyer, S., Afifi, R. A., Bearinger, L. H., Blakemore, S. J., Dick, B., Ezeh, A. C. & Patton, G. C. (2012). Adolescence: a foundation for future health. Adolescent Health, 1, 397, 1630-1638.
- Steptoe, A. & Wardle, J. (2004) Health related behavior: prevalence and links with disease. In A. A. Kaptein & J. Weinman (Eds.), Health Psychology (21 - 51). Oxford: The British Psychological Society and Blackwell Publishing Ltd.
- Steptoe, A., Wright, C., Kunz-Ebrecht, S., & R. Iliffe, S. (2006). Dispositional optimism and health behavior in community-dwelling older people: Associations with healthy aging. British Journal of Health Psychology, 11, 71-84.
- Turner, J. C. & Patrick, H. (2004). Motivational Influences on Student Participation in Classroom Learning Activities. Teachers College Record, 106(9), 1759-1785.
- Umberson, D., Crosnoe, R. & Reczek, C. (2010). Social Relationships and Health Behavior Across Life Course. Annual Review of Sociology, 36, 139-157.
- Viner, R. M., Ozer, E. M., Denny, S., Marmot, M., Resnick, M., Fatusi, A., & Currie, C. (2012). Adolescence and the social determinants of health. The Lancet. 379, 1641-1652.
- Weiss, P. & Zvěřina, J. (2009). Sexuální chování české populace. [Sexual behavior in Czech population]. Urologie pro praxi [Urology for practice] 10(3), 160-163.
- Wellings, K., Nanchahal, K., Macdowall, W., McManus, S., Erens, B., Mercer, C. H., Johnson, A. M., Copas, A. J., Korovessis, Ch., Fenton, K., A. & Field, J. (2001). Sexual behavior in Britain: early heterosexual experience. The Lancet, 358, 1843-1850.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
22 November 2016
Article Doi
eBook ISBN
978-1-80296-015-0
Publisher
Future Academy
Volume
16
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-919
Subjects
Education, educational psychology, counselling psychology
Cite this article as:
Burešová, I., & Cahová, M. (2016). Health behavior in the context of perceived social support in late adolescence. In Z. Bekirogullari, M. Y. Minas, & R. X. Thambusamy (Eds.), ICEEPSY 2016: Education and Educational Psychology, vol 16. European Proceedings of Social and Behavioural Sciences (pp. 288-301). Future Academy. https://doi.org/10.15405/epsbs.2016.11.30