
Who are those healthy behaved? The analysis of the relationship between personality and health-related behavior


Abstract
The paper is focused on health-related behavior. The study forms part of a large research project with the title “Health-Enhancing and Health-Threatening Behavior: Determinants, Models, and Consequences“ (GA13-19808S). The purpose of this study is to find a relationship between personality variables (measured using GPP-I questionnaire) and health-related behavior (
Keywords: Health-related behaviour; personality traits; responsibilityemotional stabilitysociability
Introduction
The study is patterned on two essential principles of contemporary health psychology, which are based on the fact that an individual way of life (manifested in specific forms of behavior) is a determinant that affects the individual’s health – positively or negatively (for example, Becker, Glascoff, Mitchell, Durham & Arnold, 2007). According to currently valid knowledge, the share of genetic predisposition in general health is approximately 10-20%; that of factors following from the environmental setting is 10-20%; that of availability and quality of health care services is 5-15%; but that of the behavior is about 45-60% (Conner & Norman, 1996; Mlčák, 2007; Burešová et al., 2016, etc.). Behavior is thus a crucial determinant of human health.
The study is, thus, constructed on models describing personality as the agent mediating health-beneficial or health-risky behavior (Smith & Williams, 1992). The study maps personality traits associated with healthy or on the contrary with unhealthy behavior (objective characteristics of health are not measured). The role of personality traits related to health-related behavior has been documented in a number of research studies (for example, Raynor & Levine, 2009). Most studies focused on the relationship between personality and health-related behavior are based on the Big Five theory (for example, Booth-Kewley & Vickers, jr, 1992; Hudek-Knežević & Kardum, 2009; Jerram & Goleman, 2010). The presented study provides the added value of (1) a different initial concept of personality created by Leonard Gordon (1967), used in practice as a supplement to the Big Five model, especially in the field of professional counselling or for the seeking and studying of talented individuals (see SOSIE measurement tool, Honey, 2016) as used in traffic psychology (for example, Šucha et al., 2013); this tool is also used in psychological research (e.g. Nunes et al., 2015); (2) an expanded health-related behavior model with the classic dyad (e.g. Kaptein & Weinma, 2004 or former studies of our research team, e.g. Burešová et al., 2016a,b),
Aim of the research
The paper deals with the issue of health-related behavior. The study is part of an extensive research project “
Method
Research design
The research is designed as an extensive quantitative research study. All respondents will participate based on their voluntary consent to participate. A battery of paper-and-pencil type instruments will be administered to the respondents; the instruments are used to measure the followed constructs (personality, well-being, optimism, health complaints and health-related behavior). A part of the research set is used in this study; the set includes precisely and only those research participants who were active university students at the time of administration of the instruments, and the acquired data are processed using the Health-Related Behavior Scale (Dosedlová & Slováčková, 2013).
Research instrument
For the purposes of the study, results acquired using two research methods were processed:
Global Gordon's Personal Profile Inventory: GPP-I (Czech version: Gordon, 1982) used to measure personality variables;
Health-Related Behavior Scale – HRBS (Dosedlová & Slováčková, 2013) used to measure behavioral variables.
GPP-I:
HRBS:
Research sample
The research sample of this substudy consisted of N = 650 undergraduates (61.1% women and 38.9% men) aged 18-26 years. Of the total number of 650 respondents, 11.7% lived with a partner (0.6% in a marriage, others unmarried), 15.4% were living with a housemate of the same age (a same-age peer) and 35.5% reported believing in God. All respondents were students.
Results
The first phase of data processing: a two-step cluster analysis was undertaken at first. Based on its results, the respondents were assigned to one of three clusters.
Based on visual data inspection (see the graph) it was found out regarding the individual clusters that metric values acquired by the clusters for values of individual health-related behavioral factors directly corresponded to three different life styles and differentiated these different life styles well (with the exception of factors:
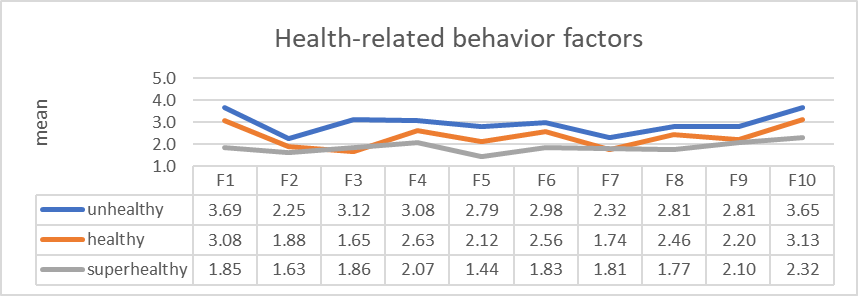
In terms of numbers, individual clusters are represented as follows: unhealthy
The second phase of data processing: scores were calculated for individual followed personality traits. Mean values for individual clusters are shown in Graph
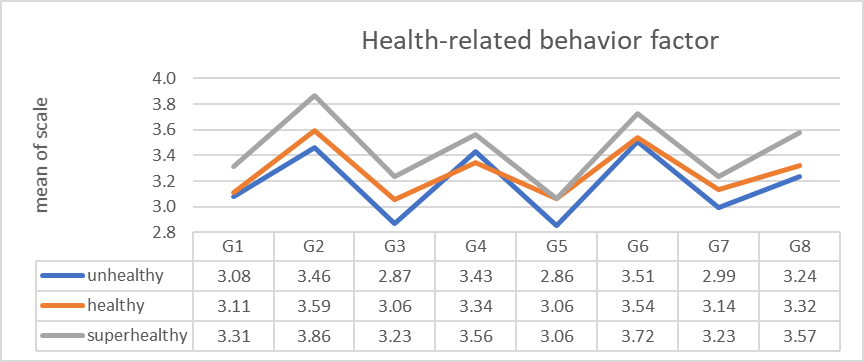
The analysis of variance was conducted to examine whether students with different health-related lifestyles significantly differ in the chosen personal characteristics. All 8 followed characteristics indicated statistically conclusive differences among the groups (F=3.61 to 18.59;df=2; p<0.05) while post hoc tests (Bonferroni) indicated statistically conclusive differences among 34 of the 48 tested couples of relationships. Exceptions where no significant differences were found include differences in personality traits G1 (unhealthy-healthy), G4 (unhealthy compared to both remaining ones), G5 (healthy-super-healthy), G6 (unhealthy-healthy), G7 (healthy-super-healthy), G8 (unhealthy-healthy), while most are predictable already based on visual inspection of Graph
Discussion
Based on the values obtained for the Health-Related Behavior Scale, three groups of respondents / behavior types were revealed using the two-step cluster analysis: unhealthy, healthy and super-healthy. Approximately one half of the respondents represented the healthy cluster where persons produce healthy behavior in a normal range, and both beyond the norm clusters were represented approximately by one quarter of the respondents. Sociodemographic data differ for the three groups.
The form of health-behavior shows a certain link connection to some personality traits. The existing research (especially in the university population) confirms a close relationship, for example, between health-promoting behavior in the form of reduced binge drinking and drug use, and the trait of agreeableness; between health-promoting behavior in the form of increased fruit and vegetable consumption and the personality traits of extraversion and openness; on the other hand, neuroticism was linked to health-deterring behaviors that included a lack of exercise and drug use (Cauchi & DeGiovanni, 2015, p. 56). Results of another research showed that low conscientiousness and high neuroticism correlate with health-behavior (were the best predictors of poor sleep hygiene, low sleep quality, and increased sleepiness, Duggan, Friedman, McDevitt & Mednick, 2014). Some studies expand the relationship between personality and behavior; for example, Cheng, Weiss & Siegel (2015, p. 21) specify that: “
In our study, we decided to analyze the followed relationship between health-behavior and personality on the background of Leonard Gordon’s personality model (1999). As indicated by our results, essentially the healthier the behavior, the higher was the score achieved in the personality trait (cluster on average). This trend was most clearly confirmed (and statistically conclusively for all the followed groups) for the traits G2 responsibility and G3 stability.
An exception in the described trend (the higher the GPP-I score, the healthier the behavior) is represented by the trait of
Conclusion
The results indicate a close relationship between personality and health-related behavior or lifestyle. Approximately one half of the followed students aged 18-26 years produce healthy behavior, and the beyond the norm forms of behavior (unhealthy and super-healthy) are represented by one quarter each. The personality traits of responsibility and emotional stability are the most reliable indicators of the health-behavior (the stronger the trait, the healthier the behavior). The trait of sociability shows an interesting relationship to health-behavior: based on the results of our study, persons with a stronger sociability trait exhibit an increased probability of producing one of the beyond the norm forms of health-related behavior (unhealthy or super-healthy). The healthiest behavior is produced by women and persons living in a partnership. One of the interpretations explains this fact in connection with a higher probability of conception and with the pressure of the current society exerted on responsibility (especially of women) for their own and their potential children’s health and the necessity of taking care of their health already before conception. Some hypothesis were also formulated regarding the effect of the primary family and remaining “embraced“ by the primary family on health-related behavior of young people. Undoubtedly, the topic has not been exhausted.
Acknowledgements
This study was supported by Czech Science Foundation project number GA13-19808S “Health-Enhancing and Health-Threatening Behaviour: Determinants, Models, and Consequences”.
References
- Booth-Kewley, S. & Vickers, R. R. jr. (1992). Associations between Major Domains of Personality and Health Behavior. Technical report 91-34. San Diego, CA: Naval Health Research Center.
- Burešová, I., Klimusová, H., Dosedlová, J. & Dacerová, V. (2016). Health-Related Behaviour of Czech Adolescents. Procedia - Social and Behavioral Sciences, 217, 1146-1152. doi:
- Burešová, I., Klimusová, H., Jelínek, M. & Dosedlová, J. (2016). Subjective Health Problems in the Context of Personality Characteristics and Health-Related Behavior in Czech Adolescents. In Pracana, Clara. Psychology Applications & Developments II. Advances in Psychology and Psychological Trends Series. Lisboa, PT: InScience Press, p. 155-162. ISBN 978-989-99389-4-6.
- Cauchi, Ch. & DeGiovanni, K. (2015). The influence of personality traits on the wellbeing of Maltese university students: a quantitative study. Malta Journal of Health Sciences, 2(2), 55-60.
- Cheng, C-H. E., Weiss, J. W., & Siegel, J. M. (2015). Personality traits and health behaviors as predictors of subjective wellbeing among a multiethnic sample of university-attending emerging young adults. International Journal of Wellbeing, 5(3), 21-43. doi:
- Chrisler, J. C., Golden, C. & Rozee, P. D. (2012). Lectures on the Psychology of Women. 4th Edition. Long Grove, IL: Waveland Press.
- Colman, A. M. (2015). Theory of reasoned action. In Colman, A. M. A Dictionary of Psychology. 4th ed. Oxford, UHK: Oxford University Press. ISBN 9780199657681.
- Conner, M. & Norman P. (Eds.) (1996). Predicting Health Behaviour. Buckingham, UK: Open University Press.
- Dosedlová, J. & Slováčková, Z. (2013). Optimismem ke zdraví? : kognitivní a osobnostní determinanty zdraví podporujícího chování. Brno, CZ: Tribun EU. ISBN 978-80-263-0386-2
- Dosedlová, J., Burešová, I., Havigerová, J. M., Slezáčková, A. & Vašina, L. (2016, in print). Zdraví podporující chování: moderátory, mediátory, konsekvence. Brno, CZ: Munipress.
- Duggan, K. A., Friedman, H. S., McDevitt, E. A. & Mednick, S. C. (2014). Personality and Healthy Sleep: The Importance of Conscientiousness and Neuroticism. PLoS One, 9(3): e90628.
- Fishbein, M. & Ajzen, I. (1975). Belief, attitude, intention, and behavior. Reading, MA: Addison-Wesley.
- Gordon, L. (1967). Survey of Personal Values. Chicago, IL: Science Research Associates.
- Gordon, L. (1999). Gordonův osobnostní profiů – inventorium (GPP-I). Globální vydání. Brno, CZ: Psychodiagnostika.
- Gutnik, A. L., Hakimzada, A. F., Yoskowitz, N. A. & Patel, V. L. (2006). The role of emotion in decision-making: a cognitive neuroeconomic approach to towards understanding sexual risk behavior. Journal of Biomedical Informatics 39(6), 720–736. doi:
- Honey, P. (2016). Pearson Talent Lens. Oxford, UK: Pearson Assessment. Retrieved from: https://www.talentlens.co.uk/
- Hudek-Knežević, J. & Kardum, I. (2009). Five-factor Personality Dimensions and 3 Health-related Personality Constructs as Predictors of Health. Croatian Medical Journal, 50(4), 394–402. doi:
- Jerram, K. L. & Goleman, P. G. (2010). The big five personality traits and reporting of health problems and health behaviour in old age. British Journal of Health Psychology, 4(2), 181-192. doi:
- Kaptein, A. A. & Weinman, J. (2004). Health psychology: some introductory remarks. In A. A. Kaptein & J. Weinman (Eds.). Health Psychology (3 - 18). Oxford, UK: The British Psychological Society and Blackwell Publishing Ltd.
- Kučera, D. & Haviger, J. (2012). Using Mood Induction Procedures in Psychological Research. Procedia - Social and Behavioral Sciences, 69(24), 31-41.
- Lašek, J., Loudová, I., Vondroušová, J., Kalibová, P. & Květenská, D. (2015). Čtyři pohledy na rodinu. Hradec Králové, CZ: Gaudeamus. ISBN 978-80-7435-531-8.
- Mlčák, Z. (2007). Psychologie zdraví a nemoci. Ostrava, CZ: Filozofická fakulta Ostravské univerzity v Ostravě.
- Nunes, R., Duarte, I., Santos, C. & Rego, G. (2015). Education for values and bioethics. Springerplus, 4(45). doi:
- Pokladníková, J. & Désirée, L. (2011). Pharmacy Students' Self-reported Health Behaviours and Spiritual Practices and Attitudes toward Complementary and Alternative Medicine. Pharmacy Education, 11 (1), 16-20.
- Raynor, D. A., & Levine, H. (2009). Associations Between the Five-Factor Model of Personality and Health Behaviors Among College Students. Journal of American College Health, 58(1), 73-81. doi:
- Ropponen, A., Narusyte, J., Alexanderson, K. & Svedberg, P. (2011). Stability and change in health behaviours as predictors for disability pension: a prospective cohort study of Swedish twins. BMC Public Health, 11(1), 678. doi:
- Simons-Morton, B. & Farhat, T. (2010). Recent Findings on Peer Group Influences on Adolescent Substance Use. Journal of Primary Prevention, 31(4), 191-208.
- Smith, T. W. & Williams, P. G. (1992). Personality and Health: Advantages and Limitations of the Five-Factor Model. Journal of Personality, 60(2), 395–425. doi: 10.1111/j.1467-6494.1992.tb00978.x
- Speirs Neumeister, K. L. (2015). Perfectionism in High-Ability Students: Relational Precursors and Influences on Achievement Motivation. Gifted Child Quarterly, 50(3), 238–251. doi:
- Stašová, L., Slaninová, G. & Junová, I. (2015). Nová generace. Vybrané aspekty socializace a výchovy současných dětí a mládeže v kontextu medializované společnosti. Hradec Králové, CZ: Gaudeamus. ISBN 978-80-7435-567-7.
- Stotland, N. L. & Steward, D. E. (2001). Psychological Aspects of Women's Health Care. 2nd ed. Washington, DC: American Psychiatric Press.
- Šucha, M., Rehnová, V., Kořán, M. & Černochová, D. (2013). Dopravní psychologie pro praxi: výběr, výcvik a rehabilitace řidičů. Praha, CZ: Grada.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
22 November 2016
Article Doi
eBook ISBN
978-1-80296-015-0
Publisher
Future Academy
Volume
16
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-919
Subjects
Education, educational psychology, counselling psychology
Cite this article as:
Havigerová, J. M., Dosedlová, J., & Burešová, I. (2016). Who are those healthy behaved? The analysis of the relationship between personality and health-related behavior. In Z. Bekirogullari, M. Y. Minas, & R. X. Thambusamy (Eds.), ICEEPSY 2016: Education and Educational Psychology, vol 16. European Proceedings of Social and Behavioural Sciences (pp. 140-148). Future Academy. https://doi.org/10.15405/epsbs.2016.11.15