
Study Regarding the Development of Spatial-Temporal Orientation Capacity and Kinaesthetic Sensitivity of Visually Impaired Pupils Using Differentiated Instruction

Abstract
This paper analyses the relevance of using differentiated instruction in the physical education lesson from a special school for visually impaired pupils. For this purpose, we applied an initial testing to establish the status of each pupil’s motricity regarding spatial-temporal orientation capacity and kinaesthetic sensitivity. The tests used for the assessment were: distance estimation test, ‘trilogy of sounds’ test and weight estimation test. In the research, there were included four samples, pupils in the 7th A and 8th A grades, as experimental groups, and the 7th B and 8th B grades, as control groups. Subsequent to initial testing, within the experimental groups, closed (not open) value groups were established. The differentiated activity was conducted according to motor ability and ophthalmic disease of each pupil involved in the research. In this regard, operational modules were developed, targeting the value groups A and B for both the 7th and 8th grades. At the end of the instructional program, the experimental groups and control groups were tested again. This new assessment identified a development of spatial-temporal orientation and kinaesthetic sensitivity indicators for the two experimental groups.
Keywords: Spatial-temporal orientation capacity, kinaesthetic sensitivity, visually impaired, blindness, differentiated instruction
Introduction
Through its subsystems, physical education is open to various categories of subjects. Physical
education of the young generation also integrates adapted physical education, which aims at recovery
and social integration by promoting programs designed for different types of disabilities (Bota,
Stănescu, & Teodorescu, 2003). Deficiency means the absence, loss or alteration of a structure or
function (anatomical, physiological or psychological) of an individual, as a result of an illness, an
accident or a disorder that hinders normal participation in social activities (Guvernul României, 2005).
In this research, the focus was on the categories of persons with sensory impairments, namely the
visually impaired.
International Council of Ophthalmology (2002) defines visual impairmentas any loss of visual
functions(visual acuity, visual field, etc.) of an organ. According to Preda (1993), visual impairment
presents different degrees, from total loss of visual acuity to amblyopia. Cziker (2001) defines visual
impairment as any loss or anomaly of a structure or function of the visual analyser.
From those presented, we can conclude that visual impairment is a sensory deficiency in which the
visual analyser’s poor activity leads to a decrease or loss in the subjects’ visual acuity, followed by the
onset of morphological, functional, motor, social and psychological disorders.
Available data indicate that the physical fitness performance of visually handicapped youngsters
decreases as the severity of visual impairment increases (Buell, 1966; Winnick & Short, 1982, quoted
by Winnick, 1985: 292).
The difficulties encountered in spatial orientation determine the blind people to adopt an attitude of
gradual resignation as regards moving to contact the environment, which decreases their chances of
social adaptation (Firea, 1979: 173). Spatial-temporal orientation capacity is defined as the ability of
the subject to find useful reference points in time and space. A blind, especially a congenitally blind
individual perceives the surrounding world directly by means of other senses, namely the acoustic,
tactile and olfactory ones. In perceiving the physical environment, the sense of touch has a huge
importance, because touching allows detailed research, which underpins the organized schemes of
objects, establishing spatial relationships between parts of an object and between objects (Viliey,
quoted by Firea, 1979: 138). The sense of touch develops on the basis of kinaesthetic sensitivity, which
is defined as the ability to discriminate the positions of body parts and the amplitude and direction of
one’s movements (Feder & Majnemer, 2007, quoted by Brink & Jacobs, 2011). It is said that a visually
impaired person does not show a degree of sensorial superiority compared with a healthy person,
sensations being exaggerated in order to obtain maximum of information from the environment
(Olerca, 1970, quoted by Firea, 1979), an absolutely necessary aspect in the development and evolution
of visually impaired pupils.
In order to streamline the instructional and educational process aimed at the spatial-temporal
orientation capacity and kinaesthetic sensitivity in physical education lessons, we used the
differentiated instruction method. In our study, we had two versions of this method, depending on the
pupil’s motor potential or ophthalmic deficiency. Physical education activities are usually organized
frontally, which blends sometimes with the work in pairs and groups. These forms of organization
provide a higher density of the lesson. Differentiated instruction approach in the lessons is justified by
the fact that pupils of the same age are not characterized by the same level of motricity; therefore, it is
recommended to conduct the activity using value groups in accordance with the motor potential. Also,
a distinctive particularity in the organization of the lesson is assigned to differentiated instruction,
according to visual impairments. Differentiated instruction can be achieved through objectives, content,
organization of the activity and teaching methodology.
Materials and methods
2.1. Purpose of the research
The purpose of this research targets the efficiency of physical education lessons focused on the
development of spatial-temporal orientation capacity and kinaesthetic sensitivity of visually impaired
pupils from the 7th and 8th grades using differentiated instruction.
2.2. Hypothesis of the research
In the physical education lesson, the use of differentiated instruction in accordance with the motor
potential and visual impairments of pupils with amblyopia and blindness from the 7th and 8th grades
will determine an improvement of their performances regarding spatial-temporal orientation capacity
and kinaesthetic sensitivity.
2.3. Participants
The subjects involved in this study are visually impaired pupils from secondary education, in the 7th
and 8th grades at the Special Secondary School for Visually Impaired Pupils from Bucharest. This
school enrols in grades 1 to 7 preschool and school age children suffering from visual impairments,
living in Bucharest or throughout the country. For each year of study, there were chosen two
classrooms: A and B. Classrooms noted with A are the experimental groups, while the classes noted
with B are the control groups. In this research, the two classrooms noted with A (7th and 8th)
represented the experimental group, and the two classrooms noted with B (7th and 8th) were accounted
as the control group. The study included 30 pupils who were assigned as follows: •7th A: 4 boys and 3 girls;
•7th B: 3 boys and 4 girls;
•8th A: 2 boys and 7 girls;
•8th B: 4 boys and 3 girls.
The subjects included in the research have both amblyopia and blindness. The ophthalmic diseases
most commonly found are represented by: myopia, retinal detachment, nystagmus, strabismus,
hyperopia, cataracts and optic atrophy.
From the associated diseases encountered in the experimental group and the control group, we
remind: attention deficit hyperactivity disorder, mental retardation, congenital heart disease, epilepsy,
hypomnesis and allergic asthma. We mention that there are cases of subjects that do not present such
an associated pathology.
2.4. Methods
During this research, we used as methods: directed observation, experimental method and statistical
indicators – mean, standard deviation and coefficient of variance.
2.5. Content of the research
During the lessons, the experimental classrooms worked by value groups resulted from the initial
assessment, in accordance with the motor potential and eye disorders of the pupils. Value groups had a
closed character, which did not allow the pupils to migrate from one group to another while running the
instruction program. Division into value groups was made according to the obtained performances and
the assessment scale shown in Table 1:
According to the scale, the performances were converted into points, which determined the value
group in which each pupil of the experimental group was distributed. The split was possible after
calculating the mean of the points obtained for all four tests(maximum 10 points and minimum 0
points for each test), as follows: value group I (40-21 points) and value group II (20-0 points).
Subsequent to the distribution into value groups, the work was differentiated within groups.
Differentiated instruction consisted in developing operational modules for each experimental group, as
follows:
•Value group I: increase in the intensity of effort, execution of varied structures of exercises, decrease in the volume of effort, progress in the complexity of effort.
•Value group II: decrease in the intensity of effort, execution of standard exercises, skill decomposition and analytical learning, increase in the volume of effort, increase in the amount of
information.
For example, pupils performed different motor tasks as movements all over the court, blindfolded,
guided by a sound stimulus emitted by various objects (whistle, bell, bouncing ball) or clapping. They
had to cover predetermined distances (3, 5, 7, 10 meters) with suppression of visual analyser, by
memorizing topography, moving inside diverse figures (square, circle, rectangle, diamond), performing
various left or right turns (180°, 360°, 540°, 720°), followed by walking on different distances,
arranging in order of size and weight objects such as table tennis, tennis, handball, volleyball, football,
basketball and oina balls, arranging in order of weight weightlifting discs of the same size (the
differences in weight were between 0.05 grams and 100 grams), placing a strip on a table and giving
the pupils (blindfolded) the instruction to place a finger left, right, above and below the strip, and in the
end to touch the strip.
The control group was not divided into value groups, but had the same initial and final assessments
as the experiment one.
2.6. Description of assessment tests
To assess the spatial-temporal orientation capacity, we used two tests: distance estimation and
‘trilogy of sounds’. The distance estimation test requires the subjects to cover a 7-meter distance (from
point A to point B) with suppression of visual analyser. Any sound source should be avoided, and the
subjects must be explained the test before starting it. Each subject will stop when they estimate that the
finishing point (point B) has been reached. The place where the subject has stopped will be marked
with an X, and the distance will be measured from point X to point B. Two situations are possible:
underestimation (when the subject has stopped before point B, the value will be noted with minus) or
overestimation (when the subject has stopped after passing the point B, the value will be noted with
plus). By assessing this, we will obtain the subject’s kinaesthetic coordination. Also, the subject’s left
and right deviation will be assessed by measuring the distance from point X, perpendicular to the line
drawn from point A to point B. This value will give us information about the subject’s vestibular-motor
coordination (Horghidan, 1997: 140-141).
In the ‘trilogy of sounds’ test, specially designed for pupils with visual impairments, an equilateral
triangle with 5m sides is drawn on the ground. From every angle of the triangle, sound signals will be
emitted: from the first angle, a pupil will dribble a basketball ball without running (first sound signal);
from the second angle, another pupil will clap hands while standing (second sound signal), and from
the third angle, another pupil will ring a bell (third sound signal). The sounds will be emitted one by
one, in the order presented before. The subject will have to cover the 3 sides of the triangle walking or
running, being helped by the sound signals. The time will be recorded.
To assess kinaesthetic sensitivity, we used the weight estimation test. There are 10 boxes with the
same external characteristics (dimension and colour), but with different weights. The lightest weights
have 15 grams, and the heaviest weights, 60 grams. The difference between two consecutive boxes is 5
grams. The subject has to put them in ascending order.
Results
Results obtained after applying the initial testing gave us information about the distribution within
the value group of all subjects in the experimental group, but also about the migration of subjects from
one group to another, after applying the final assessment (Table 2).
Comparing the initial and final assessments of experimental groups, we have concluded the
following: •7th A: othe mean is 5.71 mistakes, moderate dispersion (29.82%) at the initial assessment (2.85) and excessive dispersion (42.52%) at the final assessment. We can observe an improvement in
favour of final assessment by 2.86 mistakes.
ofor the first item - underestimation/overestimation, the mean is ±103 cm, while for the second item - left/right deviation, 66.42 cm at the initial assessment. At the final
assessment, for the first item, the average is ±42.16 cm and, and for the second item, 35.71 cm. We
notice an improvement equal to ±60.84 cm for the first item and 30.71 cm for the second item.
o the mean is 17.35 seconds, standard deviation 9.57, excessive dispersion (55.15%) at the initial assessment and 12.94 seconds at the final one. Values achieved at the final assessment are better than those achieved at the initial assessment - the performance has improved by
4.41 seconds.
•8th A: o the mean is 3.87 mistakes, standard deviation 1.80, excessive dispersion (46.65%) at the initial assessment and 1.25 mistakes at the final assessment. We can observe an improvement in
favour of final assessment by 2.62 mistakes.
ofor the first item - underestimation/overestimation, the mean is ±90.87 cm, while for the second item - left/right deviation, 69.75 cm at the initial assessment. At the final
assessment, the results are ±40.25 cm and 32.62 cm respectively. We notice an improvement equal to
±50.62 cm for the first item and 37.13 cm for the second item.
o the mean is 17.97 seconds, standard deviation 3.35, moderate dispersion (18.69%) at the initial assessment and 12.96 seconds at the final one - the performance has improved
by 5.01 seconds.
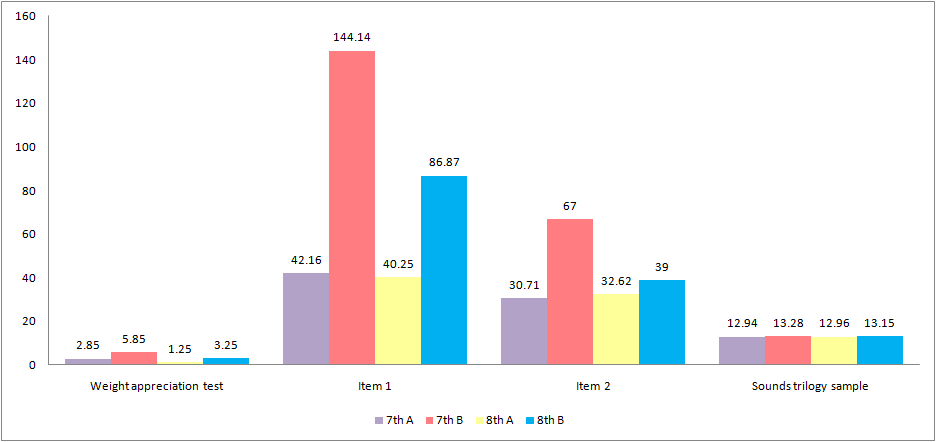
Comparing the final assessments of experimental group and control group, we can state that the
performances of the first group are better than those of the control group (Fig. 1).
Discussions and conclusions
Following the application of the differentiated program to secondary school pupils, the research
hypothesis, according to which approaching the lesson themes by value groups created depending on
the motor potential and ophthalmic deficiency has positive effects on the process of developing the
spatial-temporal orientation capacity and kinaesthetic sensitivity, has been validated. The instruction
and education process is recommended to include a combination between the activity carried out using
value groups and frontal activity. Application of the initial and final assessments highlighted the
heterogeneity of the groups regarding the level of motor abilities.
As a result of the research study on the efficiency of using differentiated instruction for pupils in the 7th and 8th grades during the physical education lesson in special education schools, it can be asserted
that spatial-temporal orientation capacity and kinaesthetic sensitivity have improved, and consequently
the pupils’ biomotor performance has also increased.
Acknowledgements
This paper is made and published under the aegis of the National University of Physical Education and Sports from Bucharest, as partner of a programme co-funded by the European Social Fund within the Sectoral Operational Programme for Human Resources Development 2007-2013 through the project Pluri- and interdisciplinarity in doctoral and post-doctoral programs, Project Code: POSDRU/159/1.5/S/141086, its main beneficiary being the Research Institute for Quality of Life, Romanian Academy.
References
Bota, A., Stănescu, M., & Teodorescu, S. (2003). Educaţie fizică şi sport adaptat pentru persoane cu deficienţe senzoriale, mintale şi defavorizate social. Bucureşti: Semne.
Brink, A., & Jacobs, A. B. (2011). Kinesthetic sensitivity and related measures of hand sensitivity in children with nonproficient handwriting. Pediatr Phys Ther., 23(1), 88-94.
Buell, C. (1982). Physical Education and Recreation for the Visually Handicapped (Revised edition). Washington, DC: American Alliance for Health, Physical Education, Recreation and Dance.
Cziker, R. (2001). Educaţia şi stimularea vizuală la copilul cu deficienţe de vedere. Cluj-Napoca: Presa Clujeană.
Firea, E. (1979). Metodica educaţiei fizice şi sportului în învăţământul liceal, professional, superior, special. Bucureşti: IEFS.
Guvernul României. (2005). Hotărârea nr. 1251/2005 privind unele măsuri de îmbunătăţire a activităţii de învăţare, instruire, compensare, recuperare şi protecţie specială a copiilor/elevilor/tinerilor cu cerinţe educative speciale din cadrul sistemului de învăţământ special şi special integrat. Retrieved from http://lege5.ro/en/Gratuit/haydgojw/hotararea-nr-1251-2005-privind-unele-masuri-de-imbunatatire-aactivitatii-de-invatare-instruire-compensare-recuperare-si-protectie-speciala-a-copiilor-elevilor-tinerilorcu-cerinte-educative-speciale- Horghidan, V. (1997). Metode de psihodiagnostic. București: Editura Didactică și Pedagogică, R.A.
International Council of Ophthalmology. (2002). Visual standards. Aspects and ranges of vision loss with emphasis on population surveys. Retrieved from http://www.icoph.org/downloads/visualstandardsreport.pdf Preda, V. (1993). Elemente de psihopedagogia intervenţiei precoce. Cluj-Napoca: Editura Universităţii Babeş-Bolyai.
Winnick, J. (1985). The performance of visually impaired youngsters in physical education activities: Implication for mainstreaming. Adapted Physical Activity Quarterly, 2(4), 292-299.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
10 June 2016
Article Doi
eBook ISBN
978-1-80296-010-5
Publisher
Future Academy
Volume
11
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-509
Subjects
Sports, sport science, physical education
Cite this article as:
Tudora, V., Mujea*, A., & Vărzaru, C. (2016). Study Regarding the Development of Spatial-Temporal Orientation Capacity and Kinaesthetic Sensitivity of Visually Impaired Pupils Using Differentiated Instruction. In V. Grigore, M. Stanescu, & M. Paunescu (Eds.), Physical Education, Sport and Kinetotherapy - ICPESK 2015, vol 11. European Proceedings of Social and Behavioural Sciences (pp. 455-461). Future Academy. https://doi.org/10.15405/epsbs.2016.06.63