
Considerations on the Growth and Development of Children with Visual Impairments


Abstract
This paper aims to reveal whether there are significant differences between the weight and height growth rate of children with visual impairments and that of children without sensory disorders. The aim of the study is to assess some parameters of growth, physiological markers of the quantitative accumulation process by which the body increases its weight and height. We used the following research methods: bibliographic study, case study, observation, weighing, height measurement and questionnaire. The subjects were selected among pupils with visual impairments, with particular comorbidities, from Special Secondary School for Visually Impaired of Bucharest, being enrolled in the 3rd grade. Inclusion criteria for the subjects of our study were the presence of vision impairment, and exclusion criteria were related to pupils with visual blindness. The findings and results highlight that the visually impaired are malnourished, which, on the long term, influences height, and on the short term, weight. Due to the dynamic data analysis, it has been found that the height, weight and body mass index of children with visual impairments is below the average child of the same age without sensory disturbances.
1. Introduction
“The evolution of the human body from the zygote stage to adulthood is characterized by the
complex process of growth and development” (Oprișescu, 2007: 5).
Growth and development are dynamic actions involving a variety of morphological, psychological
and intellectual permanent changes, which occur in an orderly sequencing, characteristic to the species.
“Body weight is the sum of weight structures that make up the body” (Cordun, 2009: 83), and “body
height is the expression of skeletal growth” (Cordun, 2009: 71).
“Amblyopia is a fairly common disease affecting between 1% and 2% of the population of most
developed countries” (Flynn, 1991: 183).
Amblyopia refers to the unilateral or (rarely) bilateral loss of vision, whose cause is the inadequate
development of neuroretinitis during childhood, because of abnormal binocular interaction.
The weight and height growth rate varies from one child to another, depending on genetic factors
and the presence or absence of sensory disorders. Also, quantitative accumulation which increases the
body weight and height is influenced by age, gender and physical activity.
People with visual impairments give up practicing physical activities and gradually go to inactivity.
Since early ages, children with amblyopia abandon physical activity, which is reflected in the physical
development of their body, particularly at the bone and muscle levels. The general appearance of the
body reveals dull muscles.
According to Teodorescu, Bota and Stănescu (2003: 92), the results described in specialized
literature prove that, at the age of 7 years, the delays in physical development are of about 2 years, and
at the age of 17, they will be of 1 year.
Another factor influencing growth and development is represented by nutrition. It consists of
ingesting foods containing proteins, carbohydrates, lipids, vitamins, fibres and minerals, for providing
the human body with energy to carry out daily activities.
To ensure growth and development proper for their age, the child nutrition must be balanced
(quantitatively and qualitatively) and diversified, and physical activity should not be missing.
to assess some parameters of growth, physiological markers of the quantitative
accumulation process by which the body increases its weight and height.
2. Materials and methods
For this study, there were used both qualitative and quantitative research methods:
consisted in consulting informative materials referring to visual impairments, kinanthropometry and nutrition.
was conducted on a group of 5 visually impaired subjects.
was used for the subjective assessment of children’s motor behaviour, as regards the
execution of adapted exercises during physical education classes.
2.1. Assessment methods
was performed using a rod weighing, under standard conditions, in the morning, before the first meal. The subjects were completely naked.
was performed using a taliometer (height meter), which directly determines the distance between vertex and sole plane. The subjects, in standing upright position, had to reach the
taliometer with their opisthocranion (external occipital protuberance), shoulder blades, buttocks and
heels. The head was kept the chin to chest, gaze was horizontal, so that the imaginary line (Frankfurt
line) joining the upper edge of the ear canal (tragion) with the lower orbit to be perpendicular to the
graduated taliometer rod. The subjects’ height was measured in the morning, after being completely
stripped for not having major physiological changes.
targeted the ratio between current weight (in kg) and height
squared (in m2), for assessing the risk of overweight; BMI = current weight/ height2.
was applied to obtain a conclusive result regarding the eating habits of children with visual impairments. It contains 11 items with predefined responses referring to the nutrition
habits of the participants.
The were selected among pupils with visual impairments from Special Secondary School
for Visually Impaired of Bucharest, being enrolled in the 3rd grade. They were 5 in number, and the
group was made up based on inclusion and exclusion criteria.
Inclusion criteria:
child diagnosed with amblyopia; secondary comorbidities to the diagnosis of amblyopia; age of participants: 9-11 years; mental and physical ability to decode the instructions and perform the required activities; attendance of the educational unit where the research was to take place.
Exclusion criteria:
total blindness; mental and physical incapacity to cooperate during the study; age under 9 years; age over 11 years; participation in a previous study.
Table 1 presents the diagnosis of subjects included in the study.
We mention that the research was conducted based on the informed consent of the parents and the
school management. According to the research ethics, we committed to keep confidential the identity
of the subjects.
3. Results
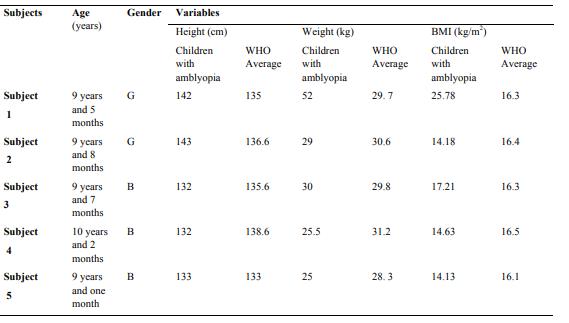
Table 2 shows the individual characteristics of the subjects. Anthropometric measurements were
compared with the growth charts made by the World Health Organization (WHO) (2007),
corresponding to the age of participants included in the study. We have not found values for visually impaired children in national or international studies.
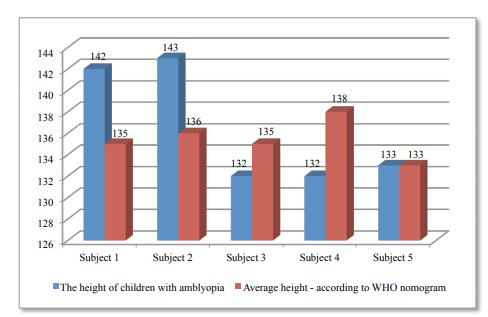
In Chart 1, we see that, related to subjects’ age, the girls are taller than average WHO nomogram,
and two of the boys have a height lower than WHO standards. One subject has an average height, according to WHO nomogram.
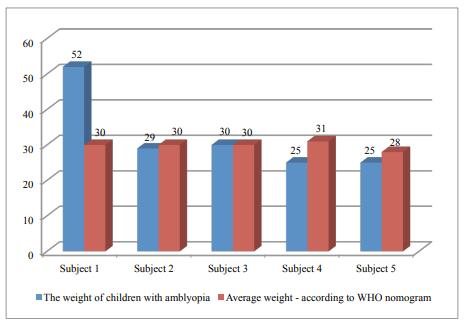
Chart 2 shows the weight of children with amblyopia. We find that one subject weighs 70% more
than the average, one subject falls within the average, and 3 subjects are underweight, according to average weight of WHO nomogram.
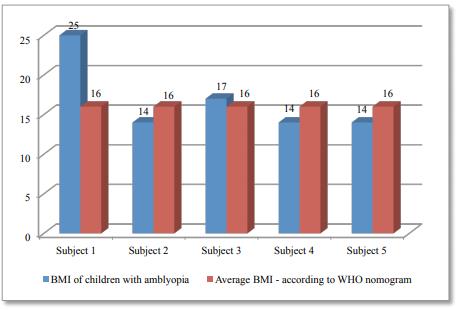
Chart 3 shows the body mass index of investigated subjects: Subject 1 is overweight, having a body mass index of 25.78 (kg/m2).
Subject 2 is underweight, having a body mass index of 14.18 (kg/m2).
Subject 3 is slightly above average, having a body mass index of 17.21 (kg/m2).
Subject 4 is underweight, having a body mass index of 14.63 (kg/m2).
Subject 5 is underweight, having a body mass index of 14.13 (kg/m2). Interpretation of the questionnaire survey results has revealed the following:
Regarding breakfast, only 2 subjects mention that they always take this meal before going to school; one subject eats breakfast sometimes, and one never eats breakfast;
At lunch, all children eat soup 2-3 times per week; 4 out of the 5 subjects mention they consume milk every day; One out of the 5 subjects (number 4) does not eat vegetables, having a BMI indicating underweight; Only one subject eats fish 2-3 times a week; 2 subjects never eat fish; one subject sometimes eats
fish;
3 out of the 5 children eat fruits every day; 2 subjects eat fruits 2-3 times a week; 3 out of the 5 subjects consume sodas daily, including subject no. 1, who is overweight; 3 participants eat sweets every day, also including subject no. 1, who is overweight; 3 subjects do not consume fast food products; 4 out of the 5 children with amblyopia consider they have healthy eating habits, including subject
no. 1, who is overweight.
4. Discussions and conclusions
After assessing the subjects’ height, related to age, we have found that the participants have average
values which correspond to the growth charts made by the World Health Organization. Regarding the
girls’ height, it is higher than the average WHO nomogram. This may be due to the fact that the values
of World Health Organization nomogram are achieved in 2007, and it is possible that, in the meantime,
the secular trend have had an impact on the somatic development, and data may not be consistent with
current individual characteristics of children without sensory disorders.
As regards the average weight of children with amblyopia compared to the average values of WHO
nomogram, we can say that subject no. 1 has a weight notably higher than the average, and one subject
is within the WHO average. For the other 3 subjects of the study, we find that the values obtained by
anthropometric measurements are below the average indicated by WHO, results being confirmed by
calculating the body mass index.
We believe that visual impairment causes changes in the anthropometric values compared to
subjects of the same age without sensory disturbances. Therefore, we consider that the diet of visually
impaired children requires special attention, both quantitatively and qualitatively.
The novelty of the study resides in the fact that we have not found research studies on this topic.
The values of anthropometric measurements performed for children with amblyopia are below the
average values provided by WHO for healthy children of the same age.
The phenomenon of accelerated growth may be the cause of differences regarding the inconsistency
with the reference values, according to the growth charts provided by WHO.
The underweight present in most of the children studied might be a consequence of the unbalanced
diet, both quantitatively and qualitatively.
Acknowledgements
This paper is made and published under the aegis of the National University of Physical Education and Sports, from Bucharest, as a part of program co-funded by the European Union within the Operational Sectoral Program for Human Resources Development 2007-2013 through the project for Pluri- and interdisciplinarity in doctoral and post-doctoral programs Project Code: POSDRU/159/1.5/S/141086, its main beneficiary being the Research Institute for Quality of Life, Romanian Academy.
References
Cordun, M. (2009). Kinatropometrie. București: CD Press.
Flynn, J. (1991). Amblyopia revisited. J Pediatr Ophthalmol Strabismus, 28(4), 183-201.
Oprișescu, I. (2007). Kinetoprofilaxia primară la vârsta evolutivă. București: Bren.
Teodorescu, S., Bota, A., & Stănescu, M. (2003). Educaţie fizică şi sport adaptat pentru persoane cu deficienţe senzoriale şi defavorizate social. București: Semne.
World Health Organization. (2007). The WHO Child Growth Standards. Retrieved from http://www.who.int/childgrowth/en/
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
10 June 2016
Article Doi
eBook ISBN
978-1-80296-010-5
Publisher
Future Academy
Volume
11
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-509
Subjects
Sports, sport science, physical education
Cite this article as:
Cordun, M., Ionescu, O., & Ghezea, A. (2016). Considerations on the Growth and Development of Children with Visual Impairments. In V. Grigore, M. Stanescu, & M. Paunescu (Eds.), Physical Education, Sport and Kinetotherapy - ICPESK 2015, vol 11. European Proceedings of Social and Behavioural Sciences (pp. 306-312). Future Academy. https://doi.org/10.15405/epsbs.2016.06.42