
Postural Control in Down Syndrome Subjects


Abstract
Objective - The Down’s syndrome children present important motor problems which affect static and dynamic balance. Equilibrium represents the capacity of keeping the body steady in standing position as well as the ability to perform usual dynamic tasks (walking, jumping and running) without falling. The objective of this paper is to present by comparison the postural control in Down syndrome subjects and non-disabled persons. Method - Five young Down syndrome subjects, aged 8 to 15 years old, and five normal age-matched subjects were included in the study. Static equilibrium was evaluated on a posturograph (Smart Balance from NEUROCOM) which has a force-plate. Equipment allows time and frequency domain analysis of the centre of pressure of the subjects. Subjects have to maintain upright position as steady as they can for 20 seconds, on the stabilised force-plate in two conditions – eyes closed and eyes open. Results - Analysis of the postural control revealed lower performance in maintaining the upright position from time domain point of view in Down syndrome group. Conclusion - Motor control problems are present in Down syndrome children since birth (hypotonia, low joint stability and joint hypermobility) and impede upon the development of motor control if early rehabilitation is not provided. This characteristic lasts for the whole life of the Down syndrome person.
Keywords: Down syndrome, postural control, posturography
1. Introduction
Down syndrome (DS) is a chromosomal anomaly caused by an additional chromosome – trisomy 21
and is characterized by important intellectual and adaptive behaviour limitations.
Triplication of the 21st chromosome described by Jacobs and Lejeune is found in all cells of the
embryo or only in some of them (mosaicism for the latter condition).
Down syndrome (mongolism) was first described as a syndrome by Langdon Down. Its incidence is
of 1/600-700 births and it is the best known dysgenesis. It is responsible for 10% of all severe mental
retardation cases.
Significant problems are present in DS, among which neuromotor control and sensory integration.
Due to these two factors, postural control and equilibrium are impaired in DS. Children with DS have
hypotonia of the limbs (most of the DS children do not walk until the age of 3-4 years), joint
hypermobility, persistence of primitive reflexes and decrease in deep tendon reflexes (Jobling, 2004,
2006).
Primitive reflexes are spontaneous, stereotypical, which are present at birth in healthy newborn
babies, as a response to a specific stimulus. As normal development occurs, these primitive responses
disappear and are replaced by automatic responses (postural reflexes). The latter ones determine
variable responses to stimuli in order to maintain upright position and equilibrium during any
movements (they prevent falls) (Gentile, 1992).
As the child develops (until the age of 2), different postural reflexes are learnt: righting (ability to
have correct orientation of head and body), protective (reactions of the extremity to rapid body
displacements) and equilibrium (allow motor control while changing the centre of gravity) (Martin,
1989; Ayres, 1972).
Children with intellectual disability have various degrees of sensory integration. These limitations in
using the sensory information impede upon learning, and this is also the case for learning equilibrium.
In DS children, delayed motor development determines delays in postural reactions as well.
Hypotonicity disrupts the feedback loop, essential in perception of the position of the body in space,
and also affects the voluntary control of muscles (Woollacott & Shumway-Cook, 1986).
Besides these abnormalities, dysfunctionality of cerebellum and brainstem, poor coordination and
time aspects of motor control are also present (Sefort & Spreen, 1979). For this reason, individual
therapy for balance and coordination problems is needed not only in early childhood, but also in
adolescent life (Connoly & Michael, 1986; Moni & Jobling, 2000).
Sensory integration stands for “the organization of sensory input for use” (Ayres, 1979, 1989,
2005). It is a neurological process which consists in evaluating each sensory input, comparing their
congruency and integration of information in order to develop appropriate responses for equilibrium/
motor behaviour.
The Down’s syndrome children present serious deficiencies at the motor and psychomotor levels,
which have negative influences on their daily living. These deficiencies should be identified and
corrected immediately after identification, so that the children could live closer to normality as early as
assessment is available - both measurement of motor function and equilibrium and of the activities of
daily living (Uyanik & Kayihan, n.d.).
The Down’s syndrome children present important motor problems which affect static and dynamic
balance. Equilibrium represents the capacity of keeping the body steady in standing position as well as
the ability to perform usual dynamic tasks (walking, jumping and running) without falling. All these
activities, normal for unchallenged children, are real challenges for DS children whose postural control
is affected.
2. Materials and methods
The aim of the study is to evaluate the equilibrium with dedicated equipment as NEUROCOM
systems (force-platform based) in order to have an objective assessment of postural control in DS
subjects compared to unchallenged age-matched subjects.
Five young Down syndrome subjects, aged 8 to 15 years, and five normal age-matched subjects
were included in the study. Static equilibrium was evaluated by Smart Balance (NEUROCOM) system.
Subjects have to maintain upright position as steady as they can for 20 seconds on the stabilised force-
plate in two conditions – eyes closed and eyes open. The posturograph has a 45cm x 45cm force-
platform which evaluates in real time the anterior and posterior displacement of the centre of gravity
(COG) during 20-second stance. Feet are placed by the operator on specific landmarks, depending on
subject’s height. Comparison with normative data is available, since the system has normal database
results from age 3.
Three tests were performed for each subject included in the study – Sensory Organisation test
(SOT), Limits of Stability (LOS) test and Rhythmic Weight Shift test. We chose these two tests since
SOT offers information regarding ability of the subjects to maintain upright position, an essential
prerequisite of normal balance. This is a method of quantitative evaluation of the individual’s ability to
process different sensory cues in order to maintain balance. LOS test reveals and quantifies reductions
in the limits of normal sway of the subject during daily movements.
SOT test requires the subject to stand still for 20 seconds in different conditions (1 to 6; for this
study, only conditions 1 and 2 were compared between Down syndrome subjects and unchallenged
ones-fixed platform, eyes open and eyes closed, respectively). These specific conditions require
different sensory inputs to be active in order to maintain stance and by progressively isolating each
sensory system we can evaluate the individual’s use of each sensory system for balance control.
Besides this Sensory Organisation test (SOT) results in graphical and numerical system,
NEUROCOM equipment offers Raw Data analysis which represents time and frequency domain
analysis of the centre of pressure movements of the tested subjects – amplitude, frequency, direction
and regularity of patient’s sway by measuring the action forces.
All subjects were evaluated with two more tests – Limits of Stability (LOS) and Rhythmic Weight
Shift. During the last two tests, subjects had to follow as soon as possible, by means of their voluntary
control, the own COG movement of a moving target. Both target and COG projection are shown on a
display placed in front of subject’s eyes.
3. Results
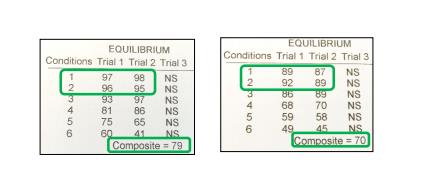
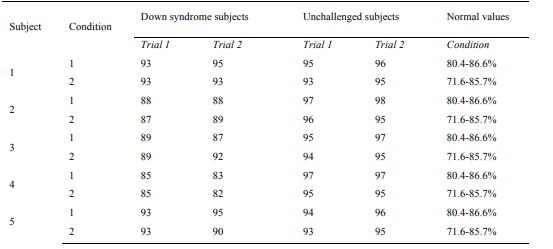
For SOT, each condition was tested twice to evaluate the ability of learning in order to obtain better
balance. Individual scores were compared with normal values for each subject. Intergroup comparison
was performed for equilibrium scores in the two conditions tested – stable platform with eyes open and
closed. SOT scores were normal for all subjects included in the study, with or without Down
Syndrome, from graphic and numeric point of view (Fig. 1, condition 1 and 2) (table 1), but Raw Data
analysis showed important differences in the amplitude and frequency of the oscillations of the COG
during 20 seconds stance both with eyes open (EO) or eyes closed (EC) (Fig. 2).
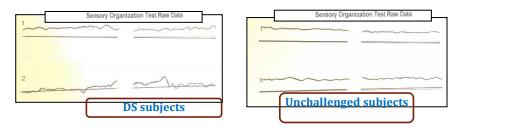
SOT Raw Data report shows both the anterior and posterior displacement of the COG and shear forces traces generated during each trial. Type and frequency of sway pattern is useful in evaluating individual way of balancing. The lighter line represents the patient’s sway direction and amplitude (anterior = up, posterior = down). H = the heavier line represents the horizontal shear forces produced at the feet level
The numeric data report provides the absolute values for each trial. They are used for comparison
with normative value range, for research and monitoring patient’s evolution under recommended
treatment.
COG is placed approximately at half of subject’s height, around umbo. Good balance is equivalent
with normal mobility while balancing, expressed as COG oscillations in a cone shape, top down during
quiet stance. Oscillations in this region of stability are as large as 12.5 degrees in anterior-posterior
direction and 16 degrees in lateral direction, and are considered as normal LOS values.
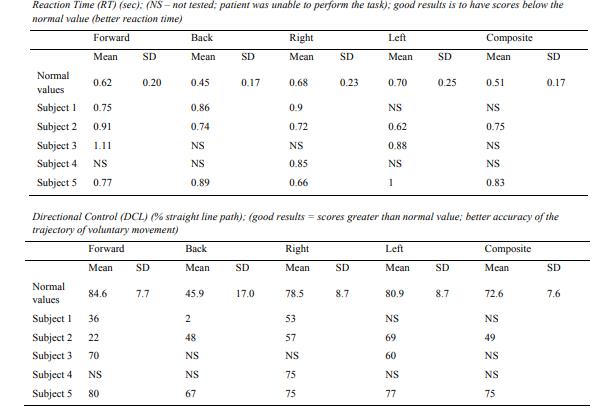
Two parameters were taken into consideration when comparing DS and normal subjects – reaction
time (RT) and Directional Control (DCL).
RT represents the time interval between movement of the target and voluntary movement of the
COG by the tested subject. If all of the subject’s movement is directly toward the target or the intended
direction (a straight line), then the amount of extraneous movement would equal zero, and the perfect
directional control score is 100%.
For LOS test, most of the DS subjects could not perform the test in all directions (reaction time
could not be measured), and when they could perform the test, poor direction control was demonstrated
(Table 2).
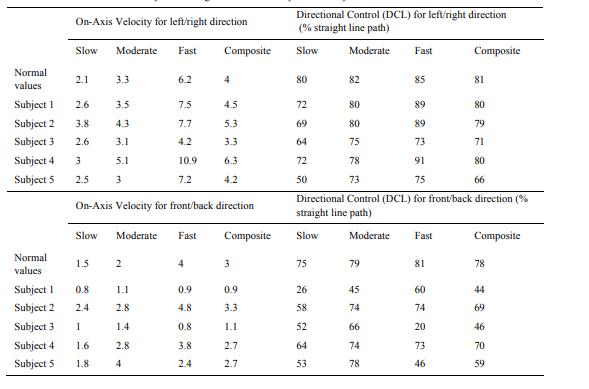
For Rhythmic Weight Shift test performed both laterally and in the anterior-posterior direction at
three specific velocities (slow, moderate and fast), DS subjects showed poor control direction as well
as accuracy, compared with normal values (Table 3).
Analysis of the postural control revealed a lower performance in maintaining the upright position
from time domain point of view in Down syndrome group, as well as a low reaction time and voluntary
direction control in DS subjects compared to unchallenged ones.
4. Discussions and conclusions
Evaluation of equilibrium is based on evaluating independently the three sensory systems involved
in balance (somatosensory, visual and vestibular ones) and also to evaluate their congruency and
central integration.
The vestibular system is one of the first sensory systems that develop prenatally (Shumway-Cook,
1992), but it takes the newborn one year to learn to use this information. Learning process is highly
correlated with experience – more motor activity the child has, faster and better development of
vestibular function is obtained.
For DS children, hypomobility and lack of cerebellum function impedes upon motor experience and
this will delay vestibular system’s normal functioning.
Since the subjects included in the study are more than 12 years old, we focused in our postural
control evaluation on the third chronological type of postural reactions – equilibrium.
SOT scores evaluate the equilibrium score for each trial by comparing the angular difference
between the patient’s maximum COG displacements, from anterior to posterior with theoretical
maximum displacement (12.5 degrees). The result is expressed as an inverse percentage between 0 and
100, with scores approaching 0 that indicate sway amplitude closely to limits of stability (risk of
falling), and 100 value indicating perfect stability. The software is based on comparison between
subject’s scores and normal values for different age groups, starting from age 3.
As already demonstrated (Shumway-Cook, 1985), children with DS have a higher than normal
latency in initiating and executing goal-directed movements. Time needed for executing high accuracy
movements, but also for standing and walking is also longer than unchallenged peers. Sensorimotor
deficits present in DS children also include perceptual-motor slowness (Elliott & Bunn, 2004: 137),
limb control problems and impaired motor efficiency (Wuang et al., 2000). LOS test and rhythmic
weight shift scores showed similar abnormal results compared with normal values (Table 3), with
increased reaction time and non-straight direction of voluntary displacement of the COG when trying
to follow the target.
Postural control in DS children is important and affects daily activities: disequilibrium, late walking
age (3-4 years), enlarged base of standing, falling easiness when running, difficulty and fear in going
downstairs, difficulty and fear in biking learning and difficulty to stop support wheels, fear or even
panic while standing alone on an oscillating surface (Haley, 1986, 1987). This latter problem seems to
be specific to DS children, as opposed to other mental retardation subjects.
Troubles in balance are common to DS children, but the impact varies from child to child. Felicioli
and Moretti (1984) found a varying percentage (41.4 to 48.9%) of disequilibrium in their small number
casuistry. They think that the smaller percentage, as related on subject persons born a five-year period
later, is already the result of a wider and earlier neuro-psychomotor rehabilitation intervention. This is
the method of choice that should be available for DS newborn-sensory integrative intervention,
vestibular stimulation, neurodevelopmental therapy are effective methods to be used in children with
an intellectual disability (Harris, 1981; Henderson, 1981).
SOT evaluation, mainly of the shear force ratio, demonstrates abnormal sway pattern in DS subjects
compared to age-matched unchallenged subjects. More than that, we could demonstrate by LOS test
and Rhythmic Weight Shift evaluation pathological differences in time reaction and directional
voluntary control in DS subjects when asking them to perform a motor task. Perception difficulties are
common in Down syndrome subjects and explain their standing and walking difficulties – higher
postural sway velocity during standing and broad base of support during walking, fear of going down
or up the stairs without bar support or another person.
Motor control problems are present in Down syndrome children since birth (hypotonia, low joint
stability and joint hypermobility) and impede upon both development of motor control and vestibular
system function development if early rehabilitation is not provided. This characteristic lasts for the
whole life of the DS person. It is essential that therapeutic programs based on the stimulation of
postural reactions to be utilized in the intervention program.
Acknowledgements
The research is achieved and published under the aegis of the National University of Physical Education and Sports of Bucharest, as a partner of the programme co-funded by the European Social Fund within the Operational Sectoral Programme for Human Resources Development 2007-2013 through the project Pluri- and interdisciplinarity in doctoral and post-doctoral programmes Project Code: POSDRU/159/1.5/S/141086, its main beneficiary being the Research Institute for Quality of Life, Romanian Academy.
References
Ayres, A. J. (1972a). Sensory Integration and Learning Disorders. Los Angeles: Western Psychological
Services.
Ayres, A. J. (1972b). Southern California Sensory Integration Tests. Los Angeles: Western Psychological
Services.
Ayres, A. J. (1979). Sensory Integration and the Child. Los Angeles: Western Psychological Services. Ayres, A. J. (1989). Sensory Integration and Praxis Tests. Los Angeles: Western Psychological Services. Ayres, A. J. (2005). Sensory Integration and the Child. Understanding Hidden Sensory Challenges (25th
Anniversary Edition). Los Angeles: Western Psychological Services.
Connoly, B. H., & Michael, B. T. (1986). Performance of retarded children, with and without Down
syndrome, on the Bruininks Oseretsky Test of Motor Proficiency.Physical Therapy, 66(3), 344-348.
Elliott, D., & Bunn, L. (2004). Motor disorders in children with intellectual disabilities. In Developmental
Motor Disorders. A Neuropsychological Perspective. New York: The Guilford Press.
Felicioli, F., & Moretti, A. (1984). Sviluppo motorio, comunicazionale linguistico ed evoluzioni dei livelli di apprendimento. In Aspetti epidemiologici, genetici, clinici, riabilitativi e sociali della Sindrome di Down. Genova: Ce.Pi.M., 307-342.
Gentile, A. M. (1992). The nature of skill acquisition: Therapeutic implications for children with movement disorders. In H. Fossberg & H. Hirschfeld (Eds.), Movement Disorders in Children (pp. 32-40), Basel: Karger.
Haley, S. M. (1986). Postural reactions in infants with Down syndrome. Relationship to motor milestone development and age.Physical Therapy, 66(1), 17-22.
Haley, S. M. (1987). Sequence of development of postural reactions by infants with Down syndrome. Developmental Medicine and Child Neurology, 29(5), 674-679.
Harris, S. R. (1981). Effects of neurodevelopmental therapy on motor performance of infants with Down’s syndrome. Developmental Medicine and Child Neurology, 23(4), 447-483.
Henderson, S. E., Morris, J., & Frith, U. (1981). The motor deficit in Down’s syndrome children: A problem of timing? Journal of Child Psychology and Psychiatry, 22(3), 233-245.
Jobling, A., & Virji-Babul, N. (2004). Down syndrome: Play, Move and Grow. Vancouver: Down Syndrome Research Foundation.
Jobling, A., & Cuskelly, M. (2006). Young people with Down syndrome: A preliminary investigation of health knowledge and associated behaviours. Journal of Intellectual and Developmental Disabilities, 31(4), 210-218.
Martin, T. (1989). Normal development of movement and function: Neonate, infant, and toddler. In Physical Therapy. Philadelphia, J.B.: Lippincott.
Moni, K. B., & Jobling, A. (2000). LATCH-ON: A program to develop literacy in young adults with Down syndrome. Journal of Adolescent and Adult Literacy, 44(1), 40-49.
Seyfort, B., & Spreen, O. (1979). Two-plated tapping performance by Down’s syndrome and non-Down’s syndrome retardates.Journal of Child Psychology and Psychiatry, 20(4), p. 351-355.
Shumway-Cook, A., & Woollacott, M. H. (1985). Dynamics of postural control in the child with Down syndrome. Physical Therapy, 65(9), 1315-1322.
Shumway-Cook, A. (1992). Role of the vestibular system in motor development: Theoretical and clinical issues.In H. Fossberg & H. Hirschfeld (Eds.), Movement Disorders in Children (pp. 209-216). Basel: Karger.
Woollacott, M. H., & Shumway-Cook, A. (1986). The development of the postural and voluntary motor control systems in Down’s syndrome children. In Motor Skill Acquisition of the Mentally Handicapped, Issues in Research and Training (pp. 45-71). North-Holland: Elsevier Science Publishers.
Wuang, Y. P., Wang, C. C., Huang, M. H., & Su, C. Y. (2000). Prospective study of the effect of sensory integration, neurodevelopmental treatment, and perceptual-motor therapy on the sensorimotor performance in children with mild mental retardation. American Journal of Occupational Therapy, 63(4), 441-452.
Uyanik, M., & Kayihan, H.(n.d.).Down syndrome: Sensory integration, vestibular stimulation and neurodevelopmental therapy approaches for children. International Encyclopaedia of Rehabilitation.
Retrieved from http://cirrie.buffalo.edu/encyclopedia/en/article/48/
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
10 June 2016
Article Doi
eBook ISBN
978-1-80296-010-5
Publisher
Future Academy
Volume
11
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-509
Subjects
Sports, sport science, physical education
Cite this article as:
Georgescu, M., Cernea, M., & Balan, V. (2016). Postural Control in Down Syndrome Subjects. In V. Grigore, M. Stanescu, & M. Paunescu (Eds.), Physical Education, Sport and Kinetotherapy - ICPESK 2015, vol 11. European Proceedings of Social and Behavioural Sciences (pp. 258-265). Future Academy. https://doi.org/10.15405/epsbs.2016.06.35