
Children’s Obesity Treatment by Physical Activity


Abstract
The goal of this study was to find out whether the obese and overweight children reduced their body weight after a 4-week stay in the Children’s Treatment Centre of Kretin. Physical activity plays the crucial role in obesity prevention. Particularly in children, physical activity also helps to develop other qualities - confidence, independence, self-control, emotional stability and overall well-being and satisfaction. It reduces stress, anxiety or aggression. The lack of movement has a negative impact to incidence of overweight and obesity and consequent diseases. Obesity causes a strain to skeletal and joint system in a growing body. Orthopaedic problems further occur in difficult and painful locomotion. The treatment of children’s obesity depends on its level and the age of the child. The complete change of lifestyle often represents the foundation stone of the therapy. This study brings results concerning weight loss in children after a 4-week treatment at the Children’s Treatment Centre of Kretin, Czech Republic. Due to overweight or obesity, the children have a daily programme which includes 2 hours of active physical activity, either indoor or outdoor. At the beginning of the 4-week therapy, the children are measured for their body weight, body height, BMI and fat amount. At the end of the curative stay, the same parameters are measured again to verify a weight loss. After completion of the 4-week curative stay, all children have lost some weight but remained in the same percentile of BMI category, i.e. their initial category of overweight or obesity remained unchanged.
Keywords: Children, overweight, obesity, physical activity
Introduction
Overweight and obesity are chronic metabolic diseases characterized by the presence of excessive
body fat in a person’s body. Overweight and obesity result from living conditions and lifestyle leading
to a long-term imbalance in energy intake and its expenditure. According to World Health
Organization (WHO), approximately a half of adult and a fifth of child population in Europe, Czech
Republic included, suffer from overweight or obesity. One of the most obvious reasons to obesity epidemic spread is the significant decrease in physical
activities as a result of modern technologies lowering the needs for physical effort and inadequate
intake of food with high energy value. Obesity occurs as a direct result of a positive energy balance,
when the equilibrium is disrupted as the energy intake exceeds its expenditure. Nowadays, there have
been discovered several other factors disrupting the metabolism in fat tissue, causing its accumulation
(Hainer et al., 2004: 293).
Overweight in children is caused by multiple factors, such as heritage, physical and psychical
condition of mother before conception, her nutrition during pregnancy and lactation period, and also
eating habits in family which affect children all the childhood and persist to maturity (Fořt, 2014: 23).
Other significant reasons for obesity might be genetic predisposition. Inappropriate and irregular eating
might play its role as well. For example, children who have breakfast regularly show lower probability
of future obesity (Kalman et al., 2011: 59).
Nowadays, every fifth child in Europe suffers from overweight or obesity. Overweight or obesity
incidence in children and youth in the Czech Republic, as well as other European countries, has been
increasing. Increased body weight is becoming the mostly reported health problem in childhood.
Approximately 80% of obese children remain obese in their adult age.
Obesity causes a strain to skeletal and joint system in a growing body. Orthopaedic problems, such
as scoliosis or kyphosis, as well as varicose veins or hip deformations might often occur. Excessive
weight might also lead to later arthritis. The growth of these children is also somewhat limited
(Valentová, 2010: 45).
In-time and continual measures against overweight and obesity will prevent later unwanted impacts
which are further divided as physiological, orthopaedic, and psychosocial. From psychological and
social aspects, obese children suffer from low self-confidence, difficulties in team interaction, and
feelings of inferiority or even discrimination (Lisá et al., 2008: 45).
The Treatment Centre Kretin is situated in the picturesque village of Kretin. Besides children with
overweight and obesity, the Treatment Centre also treats children with nutritional intake disorders
(anorexia, asthenia), repeatedly ill children, in particular those with breathing difficulties (relapsing,
persistent cough, chronic rhinitis, asthma, allergic rhinitis, etc.) and children with locomotor system
impairments (poor body posture, mild types of scoliosis). Even though the Centre is situated in the
historic château, it is furnished in a modern style. Besides newly furnished rooms, the building offers a
fitness room with a gym, hydrotherapy - including a sea bath, whirlpool, sauna and small basins for
alternating foot baths. Upon recommendation of physicians, children undergo numerous treatments
supervised by physiotherapists (curative physical exercising, inhalations, nasal baths, bio lamp,
magnetotherapy, podoscope examination, spirometry, etc.). The building itself is surrounded by a
splendid Château Park established in the 19th century. The park includes a nature trail around rare
wooded species, a FIT-trail training route, a large and a small playground, mini-golf, Russian ninepins
and trampolines. During warm weather, an outdoor heated swimming pool (12m x 6m) is available in
the garden, and children can bathe there from May to October (, n.d.). After
admission, children go through medical entrance examinations which determine overweight or obesity
and diagnose other possible health problems. Body weight and the ratio of body fat are measured by
the In-Body device. Body height is also measured. Over the course of the 4-week treatment, children
are subjected to a reduction programme which includes 6 meals a day: breakfast, snack, lunch, snack,
dinner and late dinner (the later dinner always consists of a fruit). Children further undergo a treatment
programme that includes daily exercise in the gym, afternoon long walks, Nordic walking, passing
FIT-trails in the park around the spa, swimming in the outdoor swimming pool and a large number of
other rehabilitation treatment options based on doctor’s decisions (magnetotherapy, sauna, whirlpool
baths, inhalations, alternating foot baths, wind machines, massage, sea bath, and others).
Every day in the Children’s Treatment Centre of Kretin is divided into several phases, which are
modified according to programme variety. Wake-up is at 6.30 a.m., followed by the hygiene. Curative
physiotherapeutic procedures take place between 7 and 8 o’clock. The procedures are intended for
children on the basis of spa doctor’s prescription, and involve mainly inhalation of Vincentka mineral
water, nasal irrigation by sea water, bio lamp. Procedures are followed by morning PE lesson either in
a gym, fitness centre or jogging in a park under physiotherapists’ supervision. In the morning, each
group of children perform one of the activities mentioned above, in the meantime the children play
board games. After lunch, children go for a walk, ending at 3-4 p.m., according its length and
difficulty. Then an afternoon snack is served, and after it, children are engaged in outdoor activities in a
park or sport grounds within the vicinity of the Centre.
The activities range from games such as badminton, volleyball or football to team competitions
developing speed, nimbleness and other skills. After dinner, children might devote their time to more
relaxing activities like singing competitions, quizzes, or lectures of healthy lifestyle and nutrition (1
lecture a week), or a debate with children’s psychologist where children express their feelings by the
means of various ways (painting, drama, living statues, etc.). Children are also offered a private talk
with the psychologist to solve their personal problems (i.e. in the relation with friends, parents, family,
etc.). This offer is appreciated and frequently used by children. The last meal served is late dinner,
which is always a piece of fruit. Before sleeping, children are allowed to watch television, chit chat in
their rooms or play board games. These activities are supervised by professional children nurses and
physiotherapists.
The purpose of this paper was to find out whether the obese and overweight children reduced their
body weight after a 4-week stay in the Children’s Treatment Centre of Kretin, what their weight, BMI
and body fat loss was, and whether the decrease in their body weight was significant enough to allow
the change of their BMI category - the move from category “obesity” to “overweight” and from
“overweight” to “normal body weight” category.
Materials and methods
2.1. Participants
The tested group consisted of 16 children (6 boys and 10 girls) who participated in a curative stay at
the Children’s Treatment Centre of Kretin during 25th March - 21st April 2015. The age range of boys
was 5-13, and the age range of girls, 6-15 years.
2.2. Body weight measurement
The children’s body weight was measured by the InBody 220 device which determines not only
body weight, but also, when the body height is given, on the basis of bioelectrical impedance, other
characteristics such as BMI, the amount of fat tissue, proportion of water in the body and lean muscle
mass. Children entered the InBody 220 device barefoot. The accuracy of body weight was measured to
0.1 kg.
2.3. Body height measurement
Body height was measured by anthropometry ± 0.5 cm. During measuring, children stood straight,
heels together, tips slightly apart. The head is vertically upward, like looking into the distance
(Frankfurt horizontal).
2.4. Measurement of fat contents
Body fat content was determined by bioelectrical impedance (BIA). Measurements were performed
on the InBody 220 device, which uses the method of directly controlled bio impedance analysis by the
means of eight touch electrodes (,n.d.).
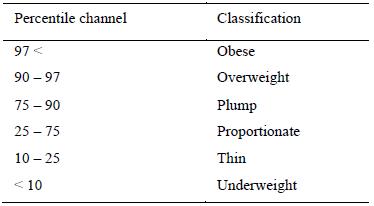
2.5. Body mass index (BMI)
The children’s BMI was calculated by the InBody 220.To evaluate BMI in children, we use
percentile graphs that compare an individual child against the population standards for children of the
same age. Graphs differ for boys and girls. Percentile graphs outline the zone in which the BMI value
is considered normal - this value corresponds to the age and gender of the child. The curves above and
below this zone indicate the percentage of children of the same age who have the same BMI value. The
zone between the 25th and 75th percentile, to which 50% of all values belong, is considered a zone of
medium values (Table 1).
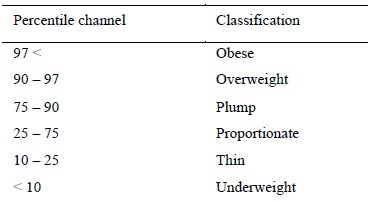
Source: www.szu.cz
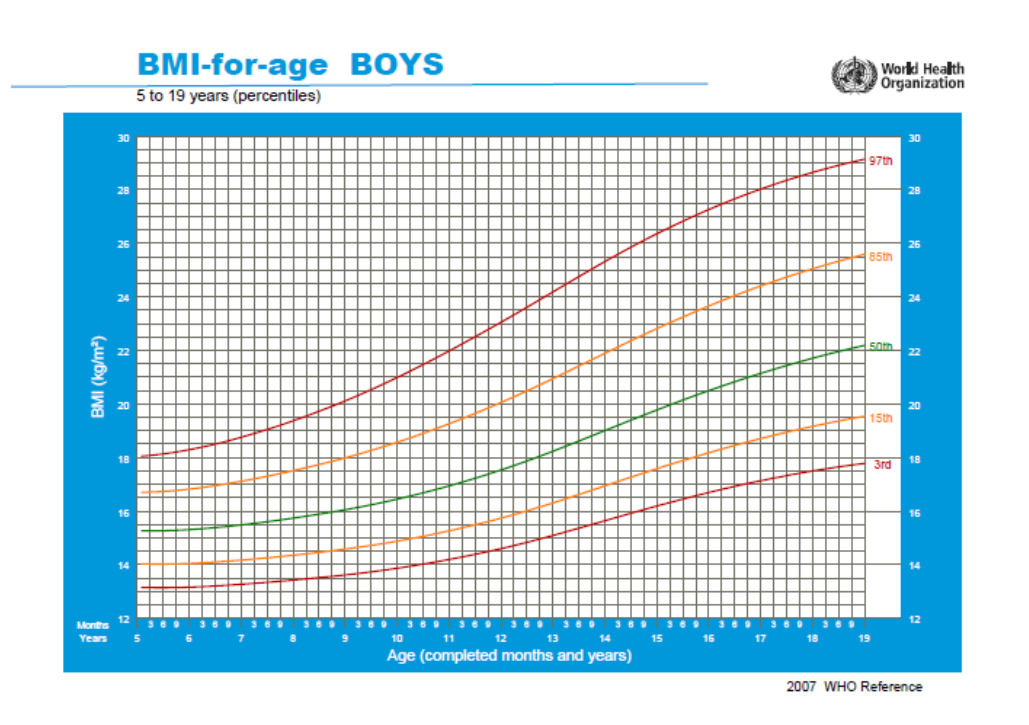
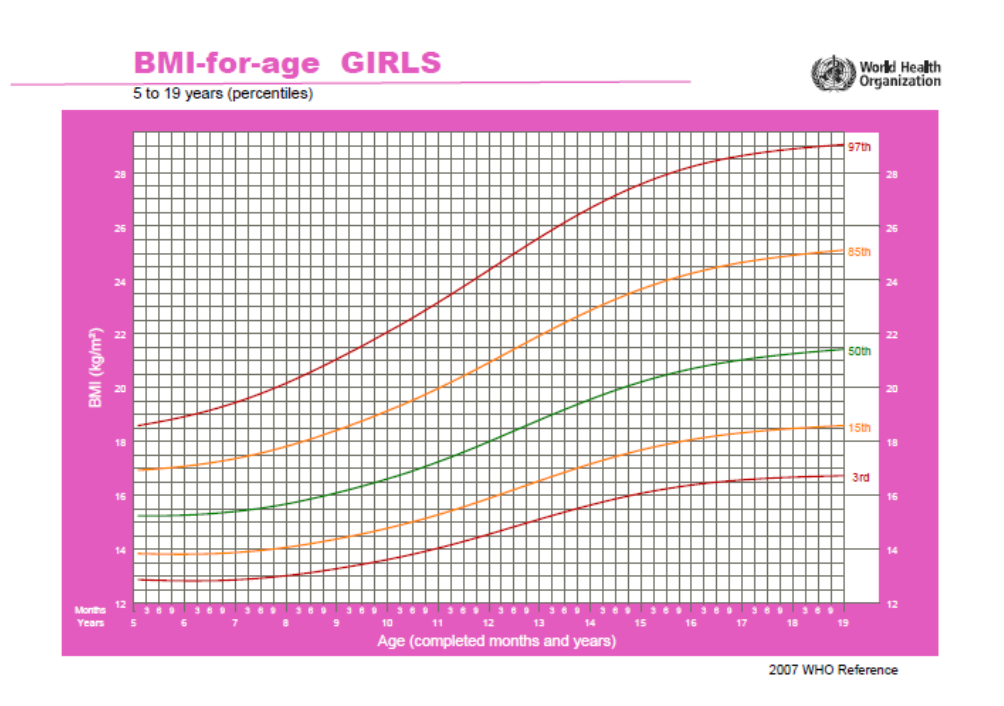
Percentile graphs of the World Health Organization are shown below - Figure 1 represents boys and
Figure 2 represents girls.
2.6. Procedure
After the admission to the Centre, all children were measured for body weight and height, BMI
calculation and the amount of fat. The same parameters were measured at the end of the stay, after 4
weeks of the weight reduction programme.
Results
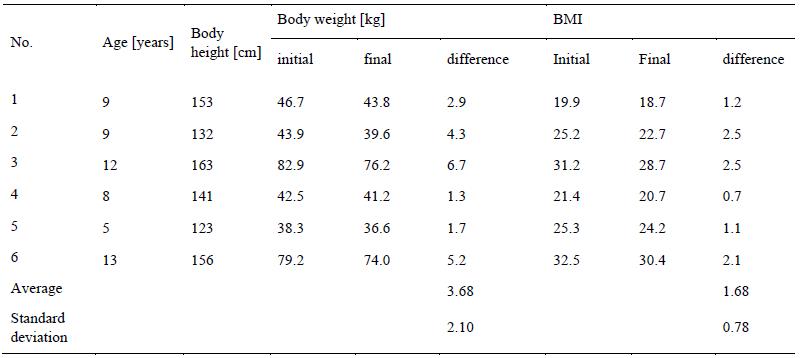
Parameters measured in children before and after their stay in the Sanatorium are shown in the
following tables. Body height, initial and final body weight, and initial and final BMI are given in
Table 2 for boys and in Table 3 for girls.
t-test: Body weight – boys; T = 0.335; t(crit) = 2.228; T˂ t(crit)
BMI – boys - T = 0.605; t(crit) = 2.228; T˂ t(crit)
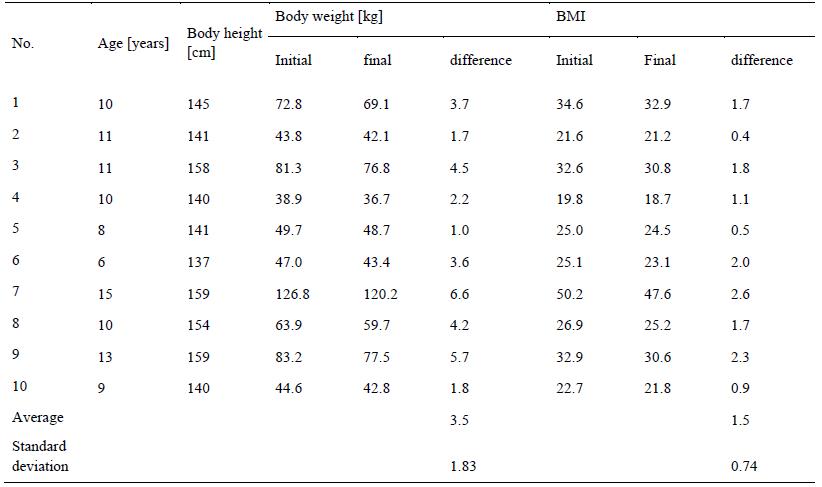
t-test: Body weight – girls; T = 1.083; t(crit) = 2.101; T˂ t(crit)
BMI – girls - T = 0.386; t(crit) = 2.101; T˂ t(crit)
The amount of body fat before admission and after completion of the programme at the Centre is
given in Table 4 for boys and Table 5 for girls.
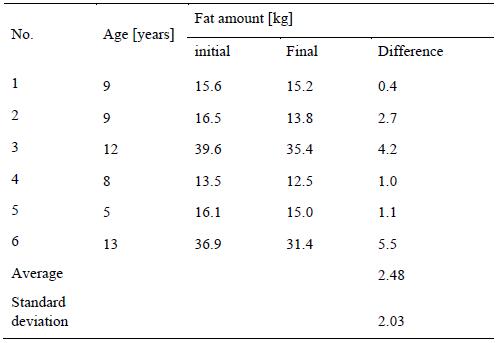
t-test: Fat amount – boys; T = 0.419; t(crit) = 2.228; T˂ t(crit)
t-test: Fat amount – girls; T = 0.407; t(crit) = 2.101; T˂ t(crit)
Discussions and conclusions
As it is obvious from the results, the treatment of overweight and obesity in the Children’s
Treatment Centre of Kretin is really successful – after completion of the 4-week curative stay, all
children have lost some weight. The difference between initial and final weight was in boys 3.68 ± 2.10
kg and in girls 3.50 ± 1.83 kg in average. The biggest difference was reported in 2 children, a boy aged
12 (no. 3) who lost 6.7 kg, and a girl aged 15 (no. 7), who lost 6.6 kg. However, considering initial and
final BMI value of these children, we have to acknowledge that, despite their weight loss, both of the
children remained in the category of obesity, since their body weight had been too high. The result of t-
test revealed that T˂ t(crit.), which means that there do not exist statistically significant differences
between initial and final body weight either in boys (0.335 ˂ 2.228) or in girls (1.083 ˂ 2.101) on the
probability level 0.05, i.e. the changes in body weight were rather insignificant. Thus, the stay in the
Sanatorium might just represent a good starting point on their way to weight reduction, provided that
they are able to keep their newly acquired eating habits and physical activities even after returning to
domestic environment.
None of the children grew up during their stay, merely weight loss has been reported, which means
that BMI value has decreased as well. The average difference between initial and final BMI values was
1.68 ± 0.78 in boys and 1.50 ± 0.74 in girls. The biggest difference in BMI values before and after the
stay was reported in two boys aged 9 (no. 2) and 12 (no. 3). The BMI decrease in both of them was of
2.5. However, the biggest BMI decrease was reported in a girl aged 15 (no. 7), who has decreased her
BMI by 2.6. Other findings of the t-test have shown that BMI changes were not highly significant
either in boys (0.605 ˂ 2.228) or in girls (0.386 ˂ 2.101).
In all children, it was also reported the lowering of body fat weight at the end of their curative stay.
The weight of body fat was decreased in boys of 2.48 ± 2.03 kg and in girls of 3.00 ± 1.61 kg in
average. The biggest reduction of fat was reported in a boy aged 13 (no. 6), who lowered his body fat
by 5.5 kg. An absolute record holder for this term was the 15 years old girl mentioned above (no. 7),
who lost 6.6 kg of fat during the stay. The decrease of body fat in the group of tested children was also
insignificant both in boys (0.419 ˂ 2.228) and in girls (0.407 ˂ 2.101).
In the Children’s Treatment Centre of Kretin, the weight loss is reached by following the principles
of healthy lifestyle, which the children did not use to obey at home. The treatment consists of various
physical activities. Although the number of these activities is suitable for domestic or school
environment, obese children tend to avoid them due to their overweight or obesity, which makes the
exercise difficult to provide properly. Taking part in speed competition, obese children are the slowest
ones, which put them in an awkward position in the eyes of their lean peers, and they often become an
object of ridicule.
The Children’s Treatment Centre of Kretin is intended for lean children with other various diseases,
but obese and overweight children form separate groups. They feel no barriers to perform an exercise,
because they are witnessed only by other children with similar problems with body weight, which is
more or less connected with certain clumsiness. The staff of the Treatment Centre has very positive
approach to children patients and any effort for an improvement is immediately praised. An inseparable
part of weight reduction programme is balanced nutrition which provides all vital elements, vitamins
and minerals to children’s body. On the contrary, sweets, light drinks and various treats, such as crisps
or chips, which some of the children were used to consume daily, are not available at all.
Even after completion of the therapies and curative procedures, all children remained in the same
percentile of BMI category, i.e. their initial category of overweight or obesity remained unchanged.
None of the changes, either in body weight, BMI or body fat content was found significant - it is a
positive finding, since the main goal of the Children’s Treatment Centre of Kretin is to initiate a
progressive weight loss by acquiring the principles of healthy lifestyle instead of fast drop of an
excessive mass, which is, from the medical aspect, totally undesirable, besides the high risk of so-
called yo-yo effect. After releasing the children from The Treatment Centre of Kretin, it will entirely
depend on children and their parents if and to what extent they are able to utilize their newly acquired
knowledge and habits.
References
Dětská léčebna Křetín. (n.d.).Retrieved from http://www.detskelecebny.cz/kretin/soucasnost.php?stranka=
soucasnost Fořt, P. (2014). Tak co mám jíst? Praha: Grada Publishing, a.s.
Hainer, V. et al. (2004). Základy klinické obezitologie. Praha: Triton.
InBody 220. Body composition analyzer. (n.d.).Retrieved from http://www.inbody.cz/soubory/katalogy-pdf/inbody220_katalog-cz.pdf Kalman, M., Sigmund, E., Sigmundová, D., Hamřík, Z., Beneš, L., … & Csémy, L. (2011). Národní zpráva o zdraví a životním stylu dětí a školáků. Olomouc: Univerzita Palackého.
Lisá, L., Kytnarová, J., Stožický, F., Procházka, B., & Vignerová, J. (2008). Doporučený postup prevence a léčby dětské obesity. Retrieved fromhttp://www.obesitas.cz/index.php?pg=doporuceni Valentová, H. (2010). Obezita a její prevence u dětí mladšího školního věku. Brno: Pedagogická fakulta Masarykovy university.
WHO (2007a). Height-for-age boys. 5-19 years (percentiles). Retrieved from http://www.who.int/growthref/cht_hfa_boys_perc_5_19years.pdf?ua=1 WHO (2007b). Height-for-age girls.5-19 years (percentiles). Retrieved from http://www.who.int/growthref/cht_hfa_girls_perc_5_19years.pdf?ua=1
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
10 June 2016
Article Doi
eBook ISBN
978-1-80296-010-5
Publisher
Future Academy
Volume
11
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-509
Subjects
Sports, sport science, physical education
Cite this article as:
Jurikova, J., & Prudilova, J. (2016). Children’s Obesity Treatment by Physical Activity . In V. Grigore, M. Stanescu, & M. Paunescu (Eds.), Physical Education, Sport and Kinetotherapy - ICPESK 2015, vol 11. European Proceedings of Social and Behavioural Sciences (pp. 158-166). Future Academy. https://doi.org/10.15405/epsbs.2016.06.22