
Effect of Aerobic Training on Ventilatory Thresholds, Aerobic and Anaerobic Thresholds in Recreational Endurance Athletes


Abstract
The study purpose is to determine if aerobic training affects aerobic capacity, as well as anaerobic threshold,minute ventilation (VE), ratio of expired carbon dioxide to oxygen utilization (VCO2, VO2). The research methods used were: bibliographical study, observation, Bruce protocol with the computerized assessment of expired gases. Three recreational athletes were tested for basal VO2max and data were used to determine their first (VT1) and second (VT2) ventilatory thresholds, VE (L/min), VCO2/VO2 (%). The intervention consisted in a 2-month period of aerobic training focused on building volume at 65% VO2. Exercise volume was controlled across the 2-month period by varying duration and frequency. Intensity during exercise was controlled by monitoring the subjects’ heart rate (HR) to stay within targeted HR zones. In the first 4 weeks, it was used a volume of around 300km (65% VO2max), and for the second 4 weeks, the volume increased to around 380km (65% VO2max). After two months of training VO2max, VT1 and VT2, we found significant improvements in both ventilatory thresholds, and also in VE, VCO2 and VO2. VO2max did not improve significantly, but there were improvements in all three subjects in their VT1, VT2, VCO2/VO2 and VE. When exercise volume is controlled and individualized based on VT, adaptation to training improves both VT1 and VT2, the subject performing no anaerobic activity over a period of 2 months.
Keywords: Aerobic capacity, ventilatory threshold, adaptation to aerobic training
Introduction
The practice of leisure sports activities has grown in recent decades, many followers of this form of
exercise pushing the functional, motor and physical limits of the body beyond the typical recreational
sphere of these activities and getting closer to performance sports area through rigorous preparation,
the level of demands and participation in different competitions.
The involvement in this type of activity ensures a balance between satisfying one’s need for
exercise, acquiring and maintaining an optimal health condition, belonging to a group, surpassing
oneself and increasing self-esteem.
Starting from the premise that an active lifestyle actually means better quality of life, regardless of
the activity in which the individual is engaged, we can assert that the healthy body culture is the result
of the interaction of hereditary, environmental, but particularly educational factors.
Recreational sport, regarded as a set of prophylactic measures used to reduce or eliminate the states
of fatigue or exhaustion caused by effort, becomes an alternative to harmful leisure activities (TV
watching, computer games, alcohol, tobacco or drug consumption etc.).
According to Epuran (2013: 334), physical relaxation is a privileged means of stress release, under
the conditions where urban environment has continuously reduced the individual’s possibilities of
expression through movement and where work multiplies the physical and mental stressors.
In this context, jogging has emerged as a variant of practice, sometimes even as a “form of
addiction”, which offers the individual the opportunity to discover his/her own body, to exceed its
limits and achieve unexpected performances (Bota, 2006: 150).
Well-systematized training sessions focused on appropriate prescription have led to progressive
increases in the covered distances, from maximum 20 km/week – for an occasional runner to 20-70
km/week – for a classical runner and more than 70 km/week – for a competitive runner (Stollenwerk,
1984). In some situations, the practitioner engages in long-distance, middle-distance or even marathon
competitions, permanently setting a higher expectation level for his/her own motor and functional
capacity.
Specialists draw attention that the engagement in recreational jogging programmes should occur
after careful medical examination, because of the risk of overexertion caused by too high exercise
intensity or increased number of kilometres, which may affect the individual’s health condition.
Thus, practitioners must establish the fitness level objectively, so that they can schedule long-term
training tasks and identify the target effort zone using concrete data about exercise capacity.
An important criterion for assessing the functional capacity is thee maximal oxygen consumption
(VO2max). The VO2max value represents a factor assessing the cardiorespiratory system adaptability
(Bota, 2000: 291).
The onset of anaerobic threshold (VT1) is described in scientific literature as the moment when
pulmonary ventilation (VE) increases disproportionally with oxygen consumption during an aerobic
exercise. At that moment, pulmonary ventilation is not linked any longer to the demand in oxygen at
cell level, the anaerobic glycolysis increasing. Inevitably, the carbon dioxide (VO2) increases buffering
the formed hydrogen ions, which will make the gas exchange rate (R; VCO2/VO2) to reach
equivalence. Subsequently, the demand in oxygen at muscle level exceeds the mitochondrial supplies,
the energy support intensifies through the anaerobic pathway and the onset of anaerobic threshold
(VT2) occurs (McArdle, Katch, & Katch, 2007: 298-299).
The purpose of this paper is to determine to what extent aerobic exercise develops both aerobic and
anaerobic capacity, assessed by the moment when the onset of ventilatory thresholds occurs and the
values of respiratory gases (VO2max, VCO2).
Materials and methods
The research methods used were: bibliographical study, observation, Bruce protocol within the
computerized Quark CPET system for indirect calorimetry.
Indirect calorimetry assessment is a non-invasive method for the simultaneous measurement of
cardiac and respiratory functions during physical effort, being used to identify the individual’s exercise
capacity level (COSMED, 2015). Quark CPET software has high quality components for a super-quick
analysis, which ensure an incomparable accuracy, reliability and also a real analysis.
Bruce protocol involves the development of a continuous maximal exercise, treadmill running,
which is structured in many stages, each one lasting 3 minutes, and uses an increase by 2% of the
treadmill gradient from one exercise stage to the other, starting at a threshold gradient of 10%. The use
of this protocol allows direct determining of VO2max, VCO2, the value of VT1 and VT2 thresholds,
heart rate, as well as the relations between these parameters of exercise capacity (Hamlin et al., 2012).
The research subjects are three practitioners of leisure activities (jogging and swimming),
participating in marathon competitions, aged between 30 and 35 years, with professions in areas that do
not require physical activity (Table 1).
Subjects were initially tested in the laboratory, using the Bruce protocol within the computerized
Quark CPET assessment system. The recorded results allowed establishing the physical exercise
parameters for the next two months of training.
The intervention consisted in applying a preparation program based on aerobic exercise, by
increasing the running volume from 300 km in the first month to 380 km in the second one. At the
same time, exercise intensity was maintained at 65% of VO2max. The heart rate of these recreational
athletes was monitored with a heart rate monitor pulse tester to determine the demand within the
targeted effort zone.
After this period of specific aerobic instruction, a final assessment was conducted to identify the
subjects’ progress, in terms of adaptation of their exercise capacity.
Results
Following the performed testing, the values of some physiological parameters were recorded to
assess the effect of the planned aerobic exercise on the investigated subjects (Table 2).
Subjects 1 and 2, practitioners of triathlon/duathlon (running and cycling), performed the initial and
final testing in the months of September and December 2014. The most relevant aspects of the
assessment regarded the physiological reaction of the body to physical demand, as follows: Subject 1 -
improved VE ventilation for VT1 by 7.47% and by 7.69% for VT2, which emphasizes that the subject
has responded to training stimuli in the preparation stage aimed to develop aerobic capacity. The VCO2
values reveal that, for VT1, this subject has improved the capacity to eliminate CO2 by 11.99% and by
4.96% at VT2 moment, which shows an increased efficiency of respiratory system, with positive
consequences on the aerobic capacity level.
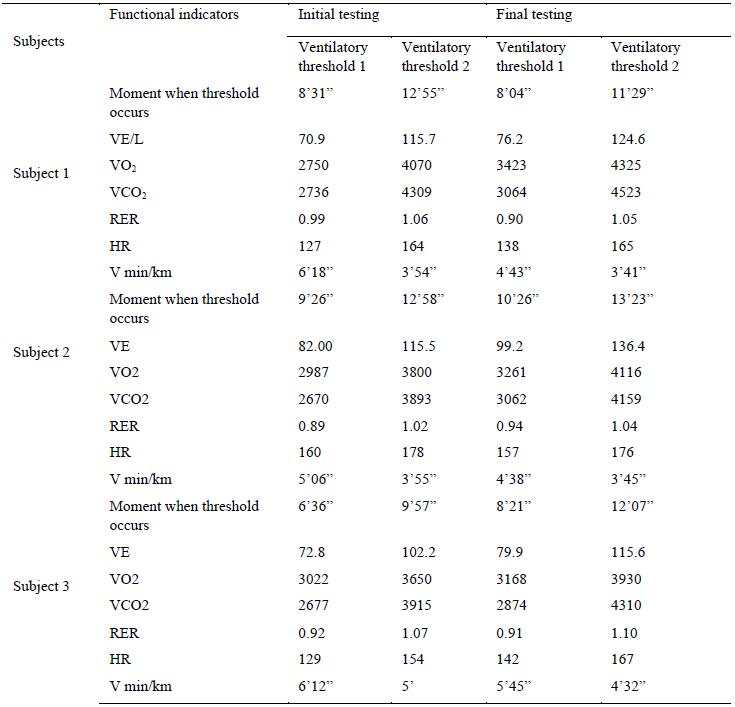
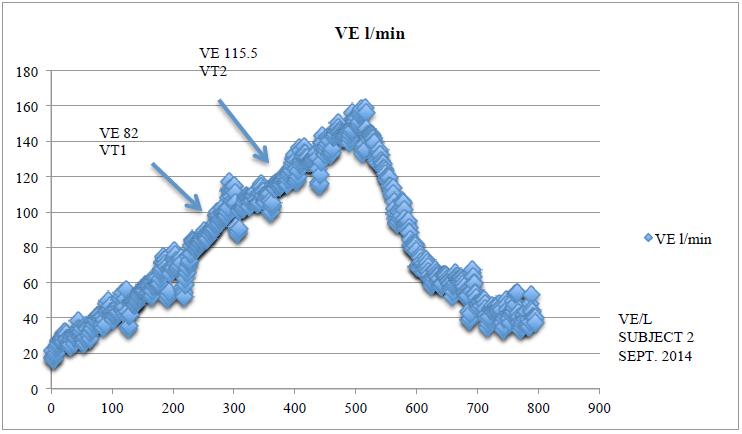
Subject 2 - improved VE ventilation for VT1 threshold, equal to 20.97%, and to 18.09% for VT2
level. As regards VCO2 at the onset of VT1 threshold, the increase was by 14.68% and by 6.83% for
VT2.
This progress is highlighted in Figure 1 (initial testing) and Figure 2 (final testing), where values
recorded for the Bruce protocol are graphically represented.
The third subject, practitioner of aerobic activities, showed an increase in VE at the onset of VT1 by
9.75% and by 13.11% at the onset of VT2. For VCO2 in VT1, the increase was by 7.35% and by
10.08% in VT2, values that might be attributed to either the non-compliance with the recommended
training program or the somatic particularities.
Regarding the heart rate values corresponding to the moment when ventilatory thresholds occurred,
we exemplify with the subject 3, who reacted best to training stimuli applied in the intervention period.
Thus, Figure 3 shows that, in the case of this subject, the onset of VT1 occurred for the basal test in
minute 9’26”, at a heart rate equal to 160 beats per min. VT2 was recorded in minute 12’58”, at a heart
rate of 178 beats per min.
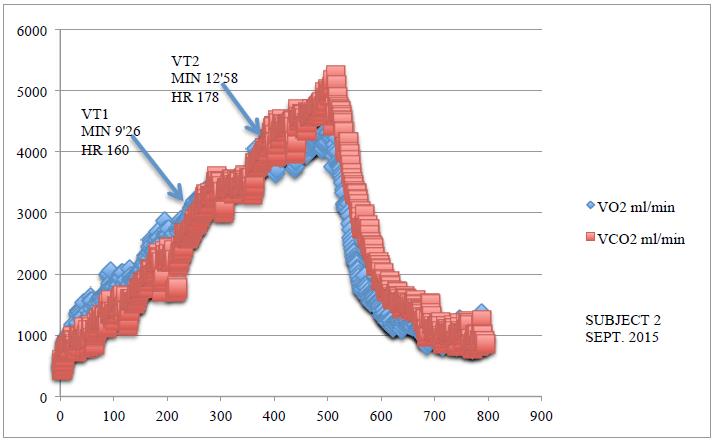
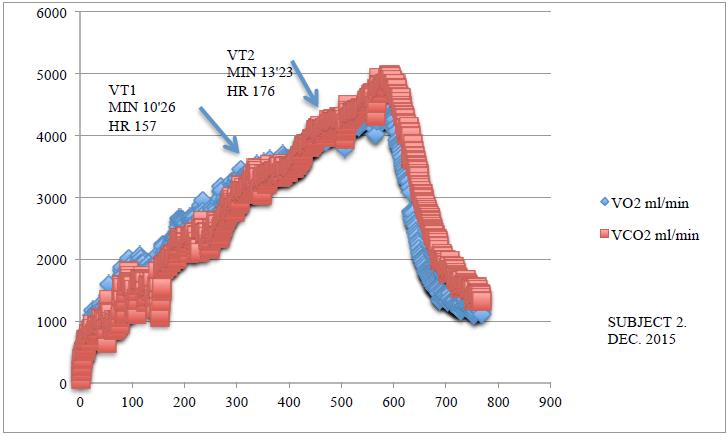
Figure 4 presents the values obtained in the final testing, where the onset of aerobic threshold
occurred in minute 10’26”, at a heart rate of 157 beats per min., and VT2 was recorded in minute
13’23”, at a heart rate of 176 beats per min.
Discussions and conclusions
Our research has suggested that aerobic training performed over a 2-month period induces adaptive
changes in the cardiorespiratory system, highlighted by the improvement of respiratory exchanges, as
well as by the delay of the moment when aerobic and anaerobic thresholds occur.
Aerobic exercise established in the moderate intensity zone, within the limits of heart rates between
140 and 160 beats per min., can lead to improved aerobic and anaerobic exercise capacity.
Heart rate monitoring allows to accurately identify exercise intensity and to set training programmes
in the targeted effort zone appropriate to the objective pursued for developing exercise capacity.
The efficiency of motor activity programmes depends on compliance with the age particularities and
individual reactivity to effort, concretized in establishing exercise volume and intensity. Computerized
Quark CPET device represents a real support in this regard, providing the information necessary to
effort dosing per exercise sequences, without jeopardizing the subject’s health, but maximizing his/her
potential.
References
Bota, A. (2006). Exerciții fizice pentru viață activă. Activități motrice de timp liber. București: Cartea
Universitară.
Bota, C. (2000). Ergofiziologie. București: Globus.
COSMED. (2015). Sport performance solution. Retrieved from
http://www.tulipmed.nu/_media/download/brochures/cosmed-sport-performance-solution.pdf
Epuran, M. (2013). Motricitate și psihism în activitățile corporale. București: FEST.
Hamlin, M. J., Draper, N., Blackwell, G., Shearman, J. P., & Kimber, N. E. (2012). Determination of maximal
oxygen uptake using the Bruce or a novel athlete-led protocol in a mixed population. Journal of Human
Kinetics, 31, 97-104.
McArdle, W., Katch, F. I., & Katch, V. L. (2007). Exercise Physiology. Energy, Nutrition and Human
Performance. Baltimore: Lippincott Williams & Wilkins.
Stollenwerk, H. J. (1984). Social-psychological aspects of jogging, aerobics and “trimming 130”. 26th
ICHPER World Congress, Israel.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
10 June 2016
Article Doi
eBook ISBN
978-1-80296-010-5
Publisher
Future Academy
Volume
11
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-509
Subjects
Sports, sport science, physical education
Cite this article as:
Tomescu, V., Urzeala, C., & Teodorescu, S. (2016). Effect of Aerobic Training on Ventilatory Thresholds, Aerobic and Anaerobic Thresholds in Recreational Endurance Athletes. In V. Grigore, M. Stanescu, & M. Paunescu (Eds.), Physical Education, Sport and Kinetotherapy - ICPESK 2015, vol 11. European Proceedings of Social and Behavioural Sciences (pp. 151-157). Future Academy. https://doi.org/10.15405/epsbs.2016.06.21