
Family functioning and disability: a study on Italian parents with disabled children


Abstract
The family of disabled persons often goes through periods of instability and mismatch; the birth of disabled children may affect communication, problem solving, satisfaction and general family functioning. The present study aims to explore the perception that both parents of disabled children have of their family functioning, measuring: the dynamics of the familiar functioning; the perception that the parental couple has about parenting and family functioning; the similarities between fathers and mothers in the perception of these dimensions. The research involved 50 parent couples (age: M=50.84; S.D=7.23), who have 100 disabled children. They completed: Family Assessment Device (
Keywords: Parentsdisabilityfamily functioningsatisfaction
Introduction
Family is an interpersonal system in balance between tendencies to stability and potential changes
(Malagoli Togliatti, & Catugno, 1996), that goes through a continuous process of identity construction
defined as “the family life cycle", characterized by developmental tasks that different members are
facing, and ending with the end of life (Erikson, 1982; Pellerone, 2013; Pellerone, Passanisi, &
Bellomo, 2015); therefore, the notion of "development stage" is no longer applied to individual
members, but to the family as a whole, highlighting the interdependence between the individual life
cycle and the family life cycle.
The family development model proposed by McGoldrick and Carter (1980) assumes that family
passes through a succession of distinct steps or stages that mark its path: the young adult between two
families, the young couple, the family with young children, the family with teenagers, the
“springboard” family for the children, and the family in old age. Each stage is characterized by specific
development tasks, that involve a renovation of the relations in torque level, of the parent-child
relationships and of the ones with the family of origin, and whose solution allows the passage to the
next stage and the acquisition of a family identity.
Families, therefore, evolve over time according to both the specific trajectories of each single
nucleus, and the phases of the life cycle; the individual evolutionary stages are linked to physical,
social, emotional-affective changes and critical events that the family could go through. According to
Hill (1949) the crisis is the result of multiple factors, namely: the stressful event and the consequent
difficulties; the greater or lesser capacity of the family to find resources; the representation the family
has about the event and its severity.
The overcoming of a critical event is given by several factors (Craparo, et al., 2014; Zani, 1997),
such as: the ability of the family to recognize and organize the available resources; the meaning it
confers to the event and to the family history; the way in which the family has dealt with the
developmental tasks related to the previous phases; and the relations with the external environment
(Magnano, Ramaci, & Platania, 2014; Pace, et al., 2015; Santisi, Magnano, Hichy, et al., 2014).
Therefore, the process of change required by stressful events includes several components, such as: a
new awareness by the family members; the attempts to arrive at a shared definition of the event; and the
search for structural changes in the family system to solve the problem (Pellerone, & Miccichè, 2015).
The more an individual, a couple, a family favor the aspects of emotional closeness and flexibility,
the more the event or the stressful situation has the possibility to be overcome, through coping
strategies that aim to achieve different goals (Patterson, 2002; Pellerone, 2015): reducing the number of
requests; acquiring resources not yet available for the family; reusing the resources already available;
learning to draw and to endure the tensions that go with the adaptation phase; and changing the way to
see the situation. Analyzing the operation of the family (as it is perceived by members of the system),
Olson and his colleagues identified, in 1983, three dimensions, which contribute to the overcoming of a
stressful event: cohesion, adaptability and communicationcommunication (Blandini, Fecarotta,
Buscemi, et
Cohesion is the size that indicates the distance or proximity from the psychological, cognitive and
affective point of view, and it is pointed out through the emotional connection among the individual
members. Adaptability indicates the ability to change the family structure based on events that occur
during the life cycle. Communication is a mode that family members use to express their needs and/or
feelings. According to the different locations that families can take on within the three dimensions, the
authors identify sixteen types of family functioning that can be summarized in three main models: the
balanced family, the intermediate family and the extreme family.
a)The balanced families are considered the most functional, because they can both maintain an
internal cohesion (ensuring a feeling of safety), and allow the differentiation of the various
members as unique individuals; they show such a flexibility that allows the different members
to adapt themselves and adjust the family structure to changes; furthermore,
appears characterized by self-confidence and confidence in the others.
b)The intermediate families can be characterized by the combination of reduced flexibility and
good cohesion, or vice versa; in the first case, the rigid family appears to be characterized by
high levels of emotional closure and inadequate flexibility, rules perceived as inviolable, and
limited communication to structural models that make difficult an exchange based on
reciprocity. Conversely, the chaotic family is characterized by a too high flexibility, difficulties
in organizing themselves adequately when placed in front of negative and para regulatory events
(sudden and unexpected), since incapable of establishing rules, roles and functions. In contrast,
looking at the size of cohesion, the enmeshed families have poor differentiation among the
various members that appear stuck in highly conditioning relations. At the opposite pole, in the
disengaged families there are not authentic emotional connections and you may find difficulties
in the organization of the structure and in the establishment of firm rules; this nucleus appears to
be extremely complex because the families lived do not have a sense of valid belonging.
c)Finally, the extreme families represent the different types of dysfunctional family, being the
most problematic in terms of global functioning. They are the result of the intersection of the
extreme models on the pole of cohesion and flexibility: chaotic disengaged, chaotic enmeshed,
stiff entangled, stiff disengaged.
1.1.Problem statement
During a family life cycle, the critical events are various and can be caused by a variety of factors:
the entrance or leaving of a component in the family, the psychosocial deviances related to the
development of the children, or the birth of a handicapped child. In particular, the presence of a child
with physical and/or psychological disability causes a block in the family life cycle: this tends to inhibit
the conjugal integration between the parents and the general level of the family functioning; the
confusion of roles, the feeling of helplessness and dissatisfaction might induce a growing state of
malaise which, in some cases, can degenerate into psychopathological forms (Larcan, & Cuzzocrea,
2011; Valtolina, 2000; Vianello, 2002).
Having a child with disabilities has a significant impact on parents, particularly in terms of stress,
mental health (DeMeyer, 1979; Olsson, & Hwang, 2001; Yirmiya, Shakes, & Solomonica-Levi, 1998)
and family functioning (Hastings, & Brown, 2002).
Literature suggests a mutual relationship between the problematic behavior of the child, the parents’
stress and their consequent behavior (Pace, Cacioppo, & Schimmenti, 2012; Pace, & Zappulla, 2011;
Schimmenti, et
the problematic behavior of the child, and their psychological resources, such as problem solving
(Floyd, Harter, & Costigan, 2004), coping strategies (Opperman, & Alant, 2003; Pellerone, 2013) and
resilience (Herring at al., 2006; Van Riper, 2007).
Another dimension that influences the overall functioning of the family is the type of disability that
affects one of the members; the international literature shows that higher levels of stress are present in
families of children with autism than in those with physical disabilities (Fombonne et
Holroyd, & McArthur, 1976; Pellerone, & Bellomo, 2015).
Especially the parents of children with pervasive developmental disorders (PDD) seem to show an
impaired level of mental health (Fisman, & Wolf, 1991), greater levels of stress (Dyson, 1997;Wolf,
Noh, Fisman, et
functioning, fatigue or exhaustion (Emerson, 2003; Hedov, Anneren, & Wikblad, 2000).
Moreover, comparative studies confirm that parents of children with ASD exhibit higher levels of
stress, depression, anxiety and emotional exhaustion than: parents of children with Down syndrome or
other types of mental retardation (Holroyd, & McArthur, 1976; Olsson, & Hwang, 2001; Wolf, Noah,
Fishman, et
1991), or parents of children with chronic diseases (Bouma, & Schweitzer, 1990).
The presence of a child with disabilities also alters the normal family life cycle, resulting in a minor
sense of parental cohesion, less marital satisfaction, and a more general problematic family functioning
(Hutton, & Caron, 2005; Montes, & Halterman, 2008).
Compared to family cohesion, it appears to be correlated to the type of disability and to the social
competence of children with disabilities; for example, mothers of children with conduct disorders
report lower levels of cohesion than mothers of children with behavior disorders.
In reference to the family functioning, instead, recent literature shows that the majority of primary
caregivers report high levels of personal and marital stress, little time for family activities, lack of
spontaneity in communication and reduced flexibility in the management of professional and daily
activities (Bluth, Roberson, Billen, et al., 2013).
Lewandowski and colleagues also demonstrated that the level of family functioning is related to the
children’s coping strategies and to the negative perception that parents have about the child’s illness. In
particular, the use of coping strategies appears related to problem solving and communication skills,
and to the general family functioning (Lewandowski et al., 2010); in contrast, low levels of negative
thoughts seem to correlate with high scores on the communication domains, the emotional
involvement, the definition of intra-family roles and the behavioral control (Pellerone, Craparo, &
Tornabuoni, 2016).
Therefore, a number of factors appear to influence the overall functioning of a family with a
disabled child, including: the type of disability, the amount and nature of disability-related disorders,
the structural and psychological characteristics of the family and the related emotional, relational and
educational dynamics, the socio - cultural level and the quantity and quality of social supports that the
family has. Unfortunately, though, in literature, from time to time, only one or more of these factors
were examined, highlighting specific effects that cannot explain the process in its entirety, leaving not
clarified many relevant aspects that have not been possible to control, and suggesting, however, always
cautious in the interpretation of the results (Hodapp, Glidden, & Kaiser, 2005; Hodapp, & Urnbano,
2007).
Moreover, in the past, most of the studies examined the patterns of reaction to the stress of disabled
children’s mothers, leaving the perception of the fathers’ family functioning on the side (Keller, &
Honig, 2004; Ricci, & Hodapp, 2003); only recently the literature has emphasized the differential
aspects of the parental couple, and the differences were usually interpreted in relation to the different
involvement of fathers and mothers in care activities towards the child (Crowe, VanLeit, &
Berghmans, 2000; Pelchat, Lefebvre, & Perreault, 2003).
In particular, this comparison showed differences in the levels of perceived stress and the
impairment of health; for example, a Swedish report on parents with Down syndrome children showed
that mothers who spent more time taking care of their children with disabilities had lower scores in the
perception of well-being than fathers. In addition, a recent study about family, reported that mothers
experience more stress and pessimism about the future of the child, and they use antidepressants or
other therapies more frequently than fathers. In the same report, mothers of children with intellectual
disabilities consider the use of specific coping strategies, such as communication and continuous
dialogue with the family, friends, and social-health operators, more effective than fathers do.
The condition of disability of a child requires a family to implement not easy adaptation processes,
since most of the parents expresses feelings of fatigue and suffering regarding the path to take to
understand the situation and to find adequate family functioning modes.
In certain circumstances, the intervention of parent training appears to be a valid instrument to the
support and enhancement of parenting, aimed at restoring a balanced family functioning. It is a
program that aims to stimulate changes in the educational function of the family, reducing stress and
discomfort that the disability situations present. The application of the parent training also involves the
removal, inside the family, of the factors that determine problem behaviors in children with disabilities,
since increasing the autonomy of the child in the home area contributes to improve the quality of the
family life.
2.Purpose of the study
The present study aims to explore the perception that both parents of disabled children have of their
family functioning, measuring: the dynamics of the familiar functioning; the perception that the
parental couple has about parenting and family functioning; the similarities between fathers and
mothers in the perception of these dimensions.
In agreement with the literature we expected that:
a)mothers of children with disability report greater distress than fathers (Gray, 1994; Hastings, 2003; Konstantareas, Homatidis, & Plowright, 1992; Milgram, & Atzil, 1998; Wolf, Noh, Fisman, et al., 1989); b)parents of older children manifest a higher level of family stress than parents of younger children (Donenberg, & Baker, 1993; Bromley et al., 2004; Lecavalieret al., 2006; Tomanik et al, 2004); c)between the predictors of the family functioning there are: the presence of cohesion, adaptability, the small hallway and enmeshment.
3.Research method
3.1.Participants
The research involved 50 parent couples (age:
(44 males and 56 females) attending two cooperatives for people with disabilities in the town of
Catania and Enna.
The instruments were administered during working hours in the cooperatives, providing, through an
information letter, a brief description of the investigation carried out, and specifying the scientific
nature and general objectives of the research. Moreover, an informed consent form was signed by the
parties before responding to the anonymous questionnaires.
3.2. Instruments
Participants completed an anamnestic questionnaire, the
Evaluation Scales IV and the Family Assessment Device.
Anamnestic data were collected through the administration of a questionnaire constructed ad hoc
and divided into two parts: the first to acquire basic information, age and professions of parents; the
second for establishing the type of disability, sex age of child.
Family Adaptability and Cohesion Evaluation Scales IV (FACES IV) is a 20-item self-report
instrument that yields two orthogonal dimensions, cohesion and adaptability (Olson, 2011; Visani et
extremely high levels (enmeshed). Adaptability ranges from extremely low (rigid) to extremely high
(chaotic). Scores near the center represent optimum levels of these dimensions. Family mean and
distance from center (DFC) scores were calculated to determine family levels of reported adaptability
and cohesion as well as each family's relative position from the center of the circumplex.
Family function was measured with the Family Assessment Device (FAD) byEpstein, Baldwin, and
Bishop (1983) in Italian version of Grandi et colleagues (2007). Each item consists of a statement and
likert scale with four possible response options (strongly agree, agree, disagree, on strongly disagree).
The scale is applicable to both one- and two-parent families. The Family Assessment Device is based
on a transactional-functional model described by Epstein and colleagues. It contains scales measuring:
problem solving, communication, roles, affective responsiveness, affective involvement, and behavior
control. The General Functioning scale contains two items from each of these six domains and is
highly correlated with the total scone of the Family Assessment Device. The General Functioning scale
has demonstrated internal-consistency reliability and construct validity” and may be scored either as a
continuous scale ranging from 12 to 48, on as a categorical measure with a score of 27 or greater
defined as “dysfunctional.”
4.Data analyses
All analyses were conducted with SPSS software (v 23.0).
In reference to preliminary data the following analyses were performed: descriptive statistics in
order to examine variables involved in the perception of their family functioning; Pearson’s
correlations were determined to measure the relation between scores of Family Adaptability and
Cohesion Evaluation Scales and the Family Assessment Device.
To verify the hypothesis that parents of older children manifest a higher level of family stress than
parents of younger children, a Multivariate analysis of variance (MANOVA) is carried out.
To verify the hypothesis that mothers of children with disability report greater distress than fathers,
Student’s t test for independent samples was used to compare the mean between groups (mothers
versus fathers).
To explore the predictive variables of the family assessment, analyses of hierarchical regression for
separate blocks were used: (a) sex and age of parents in the first block; (b) sex, age and type of
disability of children in the second block; (c) the level of family cohesion and adaptability in the third
block. Each block of independent variables was evaluated in terms of what it added to the explanation
of the variability of the dependent variable at the time of its entry, evaluating the weight of all
predictors.
Findings
Preliminary analyses
A descriptive statistic is carried out in order to examine variables involved in the perception of their
family functioning. Table
to the administration of the Family Adaptability and Cohesion Evaluation Scales.
Table
administration of the Family Assessment Device.
Pearson’s correlation was done to measure the relation between the dimensions of Faces and Fad: in
reference to the mothers, the correlation analysis shows that (Tab.
correlates negatively with the bilanced cohesion and flexibility, the enmeshment, the rigid adaptability,
the communication and the satisfaction scales; the roles correlate negatively with the disengagement,
the enmeshment, the chaotic adaptability, the communication and the satisfaction scales; the affective
responsiveness correlates negatively with the rigid adaptability and the satisfaction scale; the affective
involvement correlates negatively with the chaotic adaptability; the adaptive behavior control
correlates positively with the cohesion, and negatively with the enmeshment, the rigid and chaotic
adaptability, the communication and the satisfaction scales; at the last, the general functioning
correlates negatively with the cohesion, the enmeshment, the communication and the satisfaction scales.
Another Pearson’s correlation was done to measure the relation between dependent variables: in
reference to the fathers, the correlation analysis shows that none of the dimensions of the Faces
correlates significantly with the dimensions of the Fad (Table
Results
In reference to the first research hypothesis, the T-test for independent groups revealed no
significant differences between the father and the mother in dimensions of Faces and Fad (
So, the hypothesis that mothers of children with disability report greater distress than fathers is not
confirmed.
In reference to the second hypothesis, the Manova emphasizes the influence of independent
variables on Faces and Fad scores of mother; in particular the data show:
a)the main effect of mother’s age on the level of enmeshment (F=5.25;
affective responsiveness (F=5.28;
higher scores in the dimensions of enmeshment;
b)the main effect of child’s gender on the level of enmeshment (F=7.65;
of daughters show greater enmeshment;
c)the effect of interaction between mother’s age and child’s gender on the level of cohesion
(F=9.84;
male children manifest more cohesion; older mothers of daughters have greater
enmeshment.
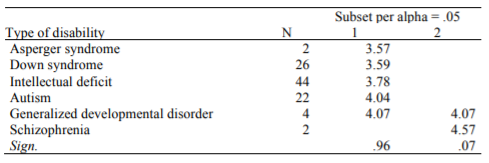
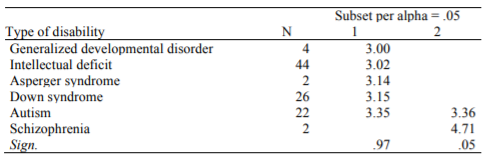
The Manova also shows the influence of the type of disability on fad and faces scores of both
parents; the data underline the main effect of the cohesion (F = 2.58;
2.74;
levels of family cohesion (Table 5); parents of children with pervasive developmental disorder
manifest lower levels of disengagement (Table 6).
To explore the predictive variables of the family assessment, analyses of hierarchical regression for separate blocks were used. The data analysis shows that predictors of the ability of problem solving are (Table 7): child’ sex and family flexibility (24.4% of the general variance).
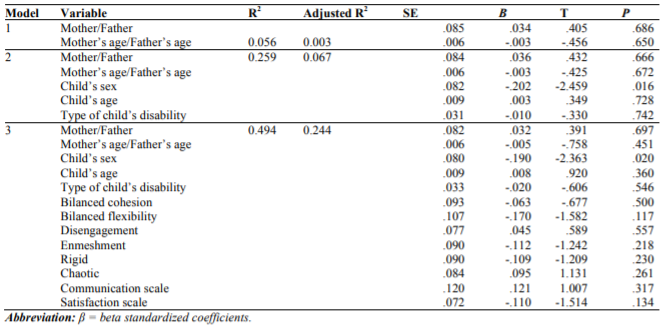
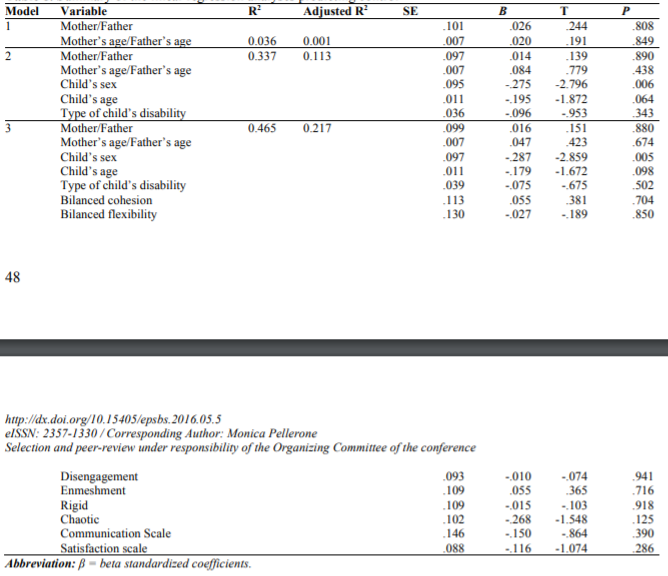
Predictive variable of family communication is the level of family disengagement (β=-2.09), accounting for only 8% of the variance. Predictive variable of the affective responsiveness is the mother’s age (β=2.09), accounting for 16.2% of the variance. At the last, predictors of control are (Table 8): sex and age of child (21.7% of the general variance). Therefore, appears confirmed the third research hypothesis
Discussion and conclusion
In this study, through analysis of the perception of the characteristics of the family system of
parents with disabled children, it has been possible to verify the existence of similarities and
differences in the perception of family ties between fathers and mothers. Specifically, the study
explored: the dynamics of family functioning; the perception that the parental couple has their own
family functioning; and the similarities between fathers and mothers in the perception of their family
functioning and parental.
The analyzes showed that the mothers with high level of satisfaction and communication manifested
high perception of general family functioning, ability of problem solving, effective responsiveness, and
behavior control. Against, the mothers characterized by enmeshment manifested low level of problem
solving, clarity in the definition of roles and general functioning; likewise the mothers with perception
of rigid family adaptability seemed to manifest low level of problem solving, affective responsiveness
and behavior control.
The mothers with a perception of chaotic family adaptability were characterized by poor definition
of roles, reduced involvement and control. At the last, disagreement in the literature, in the mothers
with good level of cohesion were present low level of problem solving and general functioning.
The first hypothesis that mothers of children with disability report greater distress than fathers
appears not to be confirmed, although it appears interesting how: mothers with older child got higher
scores in the dimensions of enmeshment; older mothers of male children are more entangled; younger
mothers of daughters show greater flexibility; and older mothers of daughters have greater cohesion. In
reference to the fathers’ score, the father of a son manifested greater flexibility, the father of a daughter
more affective response; and the fathers of grown children seem to experience greater emotional
response.
Also the type of disability seems to affect the overall family functioning, in fact: while the parents
with children with Asperger syndrome exhibit lower levels of family cohesion, instead the parents of
children with pervasive developmental disorder manifested lower levels of disengagement. It has been
suggested that the presence of behavior and emotional problems contributes significantly to the stress
of parents of children with Asperger syndrome and pervasive developmental disorder.
At the last the third research hypothesis appears confirmed, in fact: sex of child and the family
flexibility seem to be predictive variables of the family ability of problem solving; predictive variable
of family communication is family disengagement; predictive variable of affective responsiveness is
the age of mother; and above all, predictors of behavior control are sex and age of child.
Literature points out how a harmonious family environment, characterized by good functioning, can
lead parents to be more sensitive to the children’s pain, to develop less depression and greater
functional involvement. While these protective effects have been identified, most of the research till
today has focused on the negative outcomes associated with the poor functioning of the family. Future
research should explore the functioning of the family as a possible protective factor.
References
- Blandini, M., Fecarotta, P., Buscemi B., Ramaci, T., & Buscemi, A. (2015). Anti stress protocol based on the Psychological Functional Model. International Journal of Education and Research, 3 (3), 459-468 [ISSN: 2201-6333 (Print), ISSN: 2201-6740 (Online)].
- Bluth K., Roberson, P.N.E., Billen, R.M., & Sams , J.M. (2013). A Stress Model for Couples Parenting Children with Autism Spectrum Disorders and the Introduction of a Mindfulness Intervention. Journal of Family Theory & Review 5 (3), 194-213.
- Bouma, R., Schweitzer, R. (1990).The impact of chronic childhood illness on family stress: a comparison between autism and cystic fibrosis. J Clin Psychol. 46(6), 722-30.
- Bromley, J., Hare, D. J., Davison, K. & Emerson, E. (2004). Mothers supporting children with autistic spectrum disorders: social support, mental health status and satisfaction with services. Autism , 8, 409-423.
- Craparo, G., Gori, A., Mazzola, E., Petruccelli, I., Pellerone, M. and Rotondo, G. (2014). Posttraumatic stress symptoms, dissociation, and alexithymia in an Italian sample of flood victims. Neuropsychiatric Disease and Treatment, 10, 2281-2284. [doi: http://dx.doi.org/10.2147/NDT.S74317].
- Crowe, T.K., & VanLeit, B., Berghmans, K.K. (2000). Mothers’ perceptions of child care assistance: The impact of a child’s disability. American Journal of Occupational Therapy, 54 (1), 52-58.
- DeMeyer, M. K. (1979). Parents and children in autism. Washington, DC: V. H. Winston.
- Donenberg, G. & Bake,r B. L. (1993). The impact of young children with externalizing behaviors on their families. Journal of Abnormal Child Psychology , 21, 179-198.
- Dumas, J.E., Wolf, L.C., Fisman, S.N., & Culligan, A. (1991). Parenting stress, child behavior problems, and dysphoria in parents of children with autism, Down syndrome, behavior disorders, and normal development. Exceptionality, 2(2), 97–110.
- Dyson, L.L. (1997). Fathers and mothers of school-age children with developmental disabilities: parental stress, family functioning, and social support. Am J Ment Retard, 102, 267–279. [doi: 10.1352/0895-8017].
- Emerson, E (2003). Mothers of children and adolescents with intellectual disability: social and economic situation, mental health status, and the self-assessed social and psychological impact of the child's difficulties. J Intellect Disabil Res, 47, 385–399. [doi: 10.1046/j.1365-2788.2003.00498.x].
- Epstein, N.B., Baldwin, L.M., & Bishop, D.S. (1983). The Mc Master Family Assessment Devise. Journal of Marital and Family Therapy, 9, 171-180.
- Erikson, E. H. (1982). The life cycle completed: A review. New York: Norton.
- Fisman, S., & Wolf, L. (1991). The handicapped child: psychological effects of parental, marital, and sibling relationships. Psychiatr Clin North Am, 14, 199–217.
- Floyd, F.J., Harter, K.S., & Costigan, C.L. (2004). Family problem-solving with children who have mental retardation. American Journal on Mental Retardation, 109 (6), 507-524.
- Fombonne, E., Simmons, H., Ford, T., Meltzer, H., & Goodman, R. (2001). Prevalence of pervasive developmental disorders in the British nationwide survey of child mental health. J Am Acad Child Adolesc Psychiatry, 40, 820–827. [doi: 10.1097/00004583-200107000-00017].
- Gray, D. E. (1994). Coping with autism: stresses and strategies. Sociology of Health & Illness, 16, 275–300 Hastings, R.P. (2003). Child behaviour problems and partner mental health as correlates of stress in mothers and fathers of children with autism. J Intellect Disabil Res, 47, 231–237. [doi:
- Hastings, R.P., & Brown, T. (2002). Behavior problems of children with autism, parental self-efficacy, and mental health. Am J Ment Retar, 107, 222–232. [doi:
- Hedov, G., Anneren, G., & Wikblad, K. (2000). Self-perceived health in Swedish parents of children with Down's syndrome. Qual Life Res, 9, 415–422. [doi: 10.1023/A:1008910527481].
- Herring, S., Gray, K., Taffe, J., Tonge,B., Sweeney, D., Einfeld, S. (2006). Behaviour and emotional problems in toddlers with pervasive developmental disorders and developmental delay: associations with parental mental health and family functioning. Journal of Intellectual Disability Research, 50 (12), 874-882. [doi: 10.1111/j.1365-2788.2006.00904.x ].
- Hill, R. (1949). Families Under Stress: Adjustment to the Crises of War Separation and Reunion. New York: Harper & Row, 46-87.
- Hodapp, R.M., Glidden, L.M., & Kaiser, A.P. (2005). Siblings of persons with disabilities: toward a research agenda. Mental Retardation, 43 (5), 334-338.
- Hodapp, R.M., Urbano, R.C. (2007). Adult siblings of individuals with Down syndrome versus with autism: Findings from a large-scale US survey. Journal ofIntellectual Disability Research, 51 (12), 1018-1029. Holroyd, J., & McArthur, D. (1976). Mental retardation and stress on the parents: a contrast between Down's syndrome and childhood autism. Am J Ment Defic, 80, 431–436.
- Holroyd, J., McArthur, D (1976). Mental retardation and stress on the parents: a contrast between Down's syndrome and childhood autism. Am J Ment Defic, 80, 431–436.
- Hutton, A. M., & Caron, S. L. (2005). Experiences of families of children with autism in rural New England. Focus on Autism and Other Developmental Disabilities, 20 , 180–189.
- Keller, D., & Honig, A.S. (2004). Maternal and paternal stress in families with school-aged children with disabilities. American Journal of Orthopsychiatry, 74 (3), 337-348.
- Konstantareas, M. M., Homatidis S. & Plowright C. M. S. (1992). Assessing resources and stress in parents of Grandi, S., Fabbri, S., Scortichini, S., & Bolzani, R. (2007). Italian validation of the Family Assessment Devise (FAD). Rivista di Psichiatria, 42(2), 114, 122.
- Larcan, R., & Cuzzocrea, F. (2011). Funzionamento della famiglia e sviluppo psicosociale dei fratelli di individui con disabilità intellettive. Psicologia clinica dello sviluppo, XV (1), 141-171.
- Lecavalie,r L., Leone, S. & Wiltz, J. (2006) The impact of behaviour problems on caregiver stress in young people with autism spectrum disorders. Journal of Intellectual Disability Research, 50, 172-183.
- Lewandowski, A.S., Palermo, T.M., Stinson, J., Handley, S., & Chambers, C.T. (2010). Systematic review of family functioning in families of children and adolescents with chronic pain. The Journal of Pain, 11(11), 1027–1038. [doi: 10.1016/j.jpain.2010.04.005].
- Magnano, P., Ramaci, T., & Platania, S. (2014). Self-efficacy in learning and scholastic success: implications for vocational guidance. Procedia Social and Behavioral Sciences, 116, 1232–1236 [doi:10.1016/j.sbspro.2014.01.374].
- Malagoli Togliatti, M. & Catugno, A. (1996) Psicodinamica delle relazioni familiari.Bologna: Il Mulino, 32-56.
- McGoldrick, M., & Carter, E.A. (1980). The Family Life Cicle: A Framework for Family Therapy. New York: Gardner Press.
- Milgram N. A. & Atzil M. (1998) Parenting stress in raising autistic children. Journal of Autism and Developmental Disorders, 18, 415-424.
- Montes, G., & Halterman, J. S. (2007). Psychological functioning and coping among mothers of children with autism: A population-based study. Pediatrics, 119, 1040–1046.
- Olson, D.H. (2011). Faces IV and the circumplex model: validation study. Journal of Marital and Family Therapy, 3(1), 64-80.
- Olson, D.H,. Russell, C.S., & Sprenkle, D.H. (1983). Circumplex Model of Marital and Family Systems: Vl. Theoretical.Update Family Process, 22 (1), 69–83.
- Olsson, M.B., & Hwang, C.P. (2001). Depression in mothers and fathers of children with intellectual disability. J Intellect Disabil Res, 45, 535–543. [doi: 10.1046/j.1365-2788.2001.00372.x].
- Opperman, S., & Alant, E. (2003). The coping responses of the adolescent siblings of children with severe disabilities. Disability and Rehabilitation, 25 (9),441-54.
- Pace, U., Cacioppo, M., & Schimmenti, A. (2012). The moderating role of father’s care on the onset of binge eating symptoms among female late adolescents with insecure attachment. Child Psychiatry and Human Development, 43, 282–292.
- Pace, U., Madonia, C., Passanisi, A., Iacolino, C., & Di maggio, R. (2015). Is Sensation Seeking Linked Only to Personality Traits? The Role of Quality of Attachment in the Development of Sensation Seeking among Italian Adolescents: A Longitudinal Perspective. Mediterranean Journal ofSocial Sciences, 6 (2), 260-267. [doi:10.5901/mjss.2015.v6n2s1p260].
- Pace, U., & Zappulla, C. (2011). Problem behaviors in adolescence: the opposite role played by insecure attachment and commitment strength. Journal of Child and Family Studies, 20, 854–862.
- Patterson, J.M. (2002). Understanding family resilience. Journal of Clinical Psychology, 58 (3), 233–246.
- Pelchat, D., Lefebvre, H., & Perreault, M. (2003). Differences and similarities between mothers’ and fathers’ experiences of parenting a child with a disability. Journal of Child Health Care, 7 (4), 231-47.
- Pellerone, M. (2013). Identity status, coping strategy and decision making process in Italian university students. Procedia Social and Behavioral Sciences,106, 1399–1408. [doi: 10.1016/j.sbspro.2013.12.156].
- Pellerone, M. (2013). Time perception in children with developmental dyscalculia. Procedia Social and Behavioral Sciences,103, 1220–1227. [doi: 10.1016/j.sbspro.2013.10.450].
- Pellerone, M. (2015). Influence of identity, congruence of interest and coping strategy on decision making process. Procedia Social and Behavioral Sciences,191, 1344–1348. [doi: 10.1016/j.sbspro.2015.04.465].
- Pellerone, M., & Bellomo, M. (2015). Racial identity and disability. The perception of the “others” in a group of [doi: Italian school teachers. Procedia Social and Behavioral Sciences,197, 161–166. 10.1016/j.sbspro.2015.07.075].
- Pellerone, M., Craparo, G., & Tornabuoni, Y. (2016). Relationship between parenting and cognitive schemas in a group of male adult offenders. Frontiers in Psychology, 7, 302. [doi: 10.3389/fpsyg.2016.00302].
- Pellerone, M., & Miccichè, S. (2015). Psychiatric symptoms and psychological distress in patients suffering from advanced cancer and in those considered “cured”. The role of parenting and family relationship. Psychology Research, 5(4), 269–277. [doi: 10.17265/2159-5542/2015.04.007].
- Pellerone, M., Passanisi, A., & Bellomo, M.F.P. (2015). Identity development, intelligence structure, and interests: a cross-sectional study in a group of Italian adolescents during the decision-making process. Journal of Psychology Research and Behavior Management, 8, 239–249. [doi:
- Ricci, L.A., & Hodapp, R.M. (2003). Fathers’ perceptions, stress, and involvement with children with Down syndrome versus with other types of mental retardation. Journal of Intellectual Disability Research, 47, 273-284.
- Santisi, G., Magnano, P., Hichy, Z., & Ramaci, T. (2014.) Metacognitive strategies and work motivation in teachers: an empirical study. Procedia Social and Behavioral Sciences, 116, 1227 - 1231 [doi:10.1016/j.sbspro.2014.01.373].
- Schimmenti, A., Passanisi, A., Pace, U., Manzella, S., Di Carlo, G., & Caretti, V. (2014) The Relationship Between Attachment and Psychopathy: A Study with a Sample of Violent Offenders. Current Psychology DOI:
- Tomanik, S., Harris, G. E. & Hawkins, J. (2004). The relationship between behaviours exhibited by children with autism and maternal stress. Journal of Intellectual andDevelopmental Disability, 29, 16-26.
- Valtolina, G. (2000). Famiglia e disabilità. Milano: Franco Angeli.
- Van Riper, M. (2007). The sibling experience of living with childhood chronic illness and disability. Journal of Pediatric Nursing, 22 (2), 116-128.
- Vianello, R. (2002). La famiglia del minore in situazione di handicap. L’Integrazione Scolastica e Sociale, 1 (1), 36-46.
- Visani, E., Di Nuovo, S., Loriedo, C., Olson D.H. (2015). Faces IV. Il modello circonflesso di Olson nella clinica e nella ricerca. Milano: FrancoAngeli.
- Wolf, L.C., Noh, S., Fisman, S.N., & Speechley, M. (1989). Psychological effects of parenting stress on parents of autistic children. J Autism Dev Disord, 19, 157–166. [doi: 10.1007/BF02212727].
- Yirmiya, N., Erel, O., Shaked, M., & Solomonica-Levi, D. (1998). Meta-analyses comparing theory of mind abilities of individuals with autism, individuals with mental retardation, and normally developing individuals. Psychol Bull. 124(3), 283-307.
- Zani, B. (1997). Le dimensioni della psicologia sociale. Roma: NIS.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
14 May 2016
Article Doi
eBook ISBN
978-1-80296-007-5
Publisher
Future Academy
Volume
8
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-252
Subjects
Psychology, social psychology, group psychology, collective psychology, teaching, teaching skills, teaching techniques
Cite this article as:
Iacolinoa, C., Pellerone, M., Pacea, U., Ramacia, T., & Castorina, V. (2016). Family functioning and disability: a study on Italian parents with disabled children. In Z. Bekirogullari, M. Y. Minas, & R. X. Thambusamy (Eds.), Cognitive - Social, and Behavioural Sciences - icCSBs 2016, May, vol 8. European Proceedings of Social and Behavioural Sciences (pp. 39-52). Future Academy. https://doi.org/10.15405/epsbs.2016.05.5