
Parental Resilience and Adolescence Depression: Moderating Effect of Children’s Psychosocial Functioning


Abstract
Studies have shown a high prevalence of depression in adolescents. Researchers also found that psychosocial impairment is associated with depressive symptomatology in adolescence. It is now well established that parental psychopathology, mainly maternal depression, may be associated with a variety of maladaptive outcomes for children. The topic of resilience in parents, however, has been neglected. It is important to study the resilience in parents as a protective factor against the development of depressive symptomatology in children, and the variables that moderate and mediate this relationship. The main aims of this study are to examine the potential protective role of parents’ resilience regarding the development of children’s depressive symptoms and the moderating effect of children psychosocial functioning. The sample was composed by 130 adolescents aged between 14 and 17 years. Psychosocial functioning was assessed with the Adolescent Longitudinal Interval Follow-up Evaluation (
Keywords: Depression symptomatologyadolescentpsychosocial functioningresiliencesatisfactionmoderation
1.Introduction
Adolescence is the period of life between 10 and 19 years old, and encompasses the transitional phase from childhood to adulthood (Pinto, Fraga & Ramos, 2010) where the individual develops clear conceptions of himself and others (Fernandes et al., 2008). This life cycle stage involves a rapid growth and various physical and psychosocial changes (Resende, Santos, Santos, & Ferrão, 2013). Mood swings may happen, which are part of normative adaptation to changes in the body and in relationships in adolescence (Pinto et al., 2010).
At this stage, the adolescent faces several challenges, as well as stress and anxiety provocative situations. Suffering and difficulties may arise not only for the adolescent, but also for the people around him, including family and friends (Arnett, 1999). The emotional instability characteristic of this developmental phase may increase the likelihood of developing mental disorders or symptoms, such as depressive symptomatology (Brito, 2011).
Among the most common disorders in adolescence we have schizophrenia, mood disorders (e.g. depression and bipolar disorders), eating disorders, substance abuse and even sexual problems (e.g. gender identity disorder) (McIntosh, Helms, Smyth, 2003; Pinto et al., 2010).
In the last two decades there has been an increase in the number of cases of depression beginning in childhood and adolescence (Coutinho, 2001). Depression in adolescence can have a lasting nature and can affect multiple individual functions, leading to psychosocial damages (Bahls, 2002). For this reason, authors (Gladstone, Beadslee, & O'Connor, 2011; Kovacs, 2006) have carried out studies in order to understand this disturbance in this developmental phase.
In adolescence, according to the DSM-V (APA, 2002), the presence of depressive symptoms is manifested by irritability, depressed mood, loss of energy, demotivation and lack of interest in activities that were previously pleasurable. Individuals may present retardation or psychomotor agitation, low self-esteem, feelings of blame, isolation, concentration difficulties and sleep and food alterations. Depression leads to school performance losses and difficulties in interaction with colleagues and relatives. Risk behaviors, self-harm and suicidal ideas or attempts can also be present (Brooks, Harris, Trahls, & Woods, 2002). In the presence of depressive symptoms, the adolescent could also express an increase in behavioral problems (Saluja et al., 2004) and substance abuse (Kubik, Lytle, Birnbaum, Murray, & Perry, 2003) that cause vulnerabilities and may compromise the adolescent’s future (Arnarson & Craighead, 2009; Rao & Cohen,2009).
Depression can be understood through the interaction between genetic, psychological and social factors (Correia & Linhares, 2007). Sheeber, Hops, and Davis (2001) suggest that family and social relationships are relevant factors in understanding depressive symptoms in adolescents, because of the relation between problematic family relationships, presence of parental psychopathology, low socio-economic level, interpersonal conflicts, low academic achievement and low satisfaction with
life and a high risk for the adolescent to develop depressive symptomatology (Bahls, 2002; Gladstone, & Beardslee, 2009; Pérez & Urquijo, 2001).
Literature has found that children of depressed parents are more likely to develop psychological diseases during childhood and adolescence and to have a compromised psychosocial functioning in a number of areas, compared with children of parents without depression (Beardslee, Versage, & Glandstone, 1998; Jaser et al., 2007; Lewinsohn, 2003).
In the presence of depressive symptomatology, adolescents' psychosocial functioning is compromised (Claudino, Cordeiro, & Arriaga, 2006; Goldstein et al., 2009; Greer, Kurian, & Trivedi, 2010; McCabe, 2011), preventing him from achieving successfully developmental tasks that would be expected for his age and context (Lewinsohn, Rohde, Seleey, Klein, & Gotlib, 2003). In adolescents, it is common to observe social problems, such as greater isolation in relation to peers, low academic achievement, less involvement in recreational activities, adult dependency and difficulties in problem solving (Claudino et al., 2006; Dunn & Weintraub, 2008; Gledhil, 2010; Nilsen et al., 2013).
Torgalsbφen (2012), in a study on schizophrenia found that subjects with better psychosocial functioning or in other words with better interpersonal relationships and social skills, recovered fully after a few years, compared with subjects with weak psychosocial functioning. This data proved to be useful in the development of more effective interventions.
Costa (2011) evaluated the psychosocial functioning of adolescents through a semi-structured interview, A-LIFE. Results showed that adolescents with psychopathology present higher values of invalidation in psychosocial functioning. In this study, it was not possible to establish a relationship between parental psychopathology and psychosocial functioning of adolescents.
Goldstein et al. (2009), in a study with bipolar children and adolescents, aged between 7 and 17 years, using A-LIFE to assess psychosocial functioning, found that higher levels of depressive symptomatology led to greater psychosocial invalidation and less satisfaction in these young individuals, compared to young people who were in partial remission or recovery.
Studies have established that the suffering of parents, such as depression, especially in mothers, can be associated with a variety of results related to poor adaptation in their children (Bahls, 2002; Barker, Copeland, Maughan, Jeffer, & Uther, 2012; Bercker et al., 2012; Biederman et al., 2008). On the other hand, studies have found that parents with more suitable parental characteristics, more resilient and more involved in the lives of their children, promote a more adequate psychosocial functioning (Gladstone, Boydell, & Mckeever, 2006; Wong, 2008).
However, the topic of parental resilience has been neglected and, in literature, few studies explore the relationship between parents' resilience and depressive symptomatology in children. Resilience is the ability for an individual to overcome, with success, adverse conditions or situations involving risk to his/her well-being, development and mental health; moreover, resilience levels may increase throughout the life cycle of the individual (Bauman, Adams, & Waldo, 2001; Reppold, Mayer, Almeida, & Hutz, 2012).
The present study aims to investigate parental resilience as a possible protective factor regarding the development of depressive symptomatology in adolescents and to understand which variables moderate this relationship. Understanding this relationship may be important for the development of programs that prevent the onset of depressive symptomatology and that include parents and adolescents.
2.Material and methods
2.1.Participants
The sample was collected in public schools in the central area of the country. It consists of 131 adolescents and their parents who were enrolled in a research project about prevention of adolescent depression (PTDC/MHC-PCL/4824/2012).
Regarding the sample of adolescents, 89 were females (67.9%) and 42 were males (32.1%), between the ages of 13 and 17 years old (M = 14.47; SD = .816). Most students indicated good school performance (n = 70; 53.4%), 42% satisfactory (n = 55) and only a minority of 15.3% said they had already failed (n = 20).
With respect to parents, 85.5% were female (n = 112) and 14.5% were males (n = 19), aged between 28 and 66 (M = 42.79; SD = 6.05). In relation to the socio-economic level of the family of the adolescent, 42.7% presents a low socio-economic level, 46.6% a medium one and 9.9% a high level.
With regard to civil status, the majority of the parents were married (n = 97, 74%), 13% divorced, 4.6% were widowed, 3.8% separated, 3.1% were in a non-marital partnership and 1.5% indicated being single.
2.2.Instruments
To obtain the total score of psychosocial functioning the mean was calculated, adding all of the domains and dividing by the number of domains. It should be noted that high scores indicate low levels of psychosocial functioning. The note in each domain resulted from the mean of the functioning in that area during the follow-up period that is the level of functioning in each month of follow-up, which goes from 1 to 5 and was divided by the number of months of follow-up. The same procedure was taken to assess adolescents' satisfaction with their functioning in the various areas of life. Keller et al. (1987) found a good inter-evaluator reliability for the interview.
2.3.Procedure
Initially, participants were informed about the objectives of the investigation as well as about the anonymity and confidentiality of the data, providing prior written consent about the participation in the investigation. The CDI was administered in a classroom context. The Resilience scale (RS23) was included in the evaluation protocol for parents and after completed was handed over to investigators. The Adolescent Interval Longitudinal Follow-up Evaluation (A-LIFE) was applied in a reserved place to every adolescent.
2.4.Analytic Strategy
Data was entered and analysed using the Statistical Package for Social Sciences (SPSS), version
22.0 for Windows.
Descriptive analyses were performed to calculate frequencies, means and standard deviations in order to characterize the sample (n = 131), taking into account sociodemographic variables. Analysis of gender differences was obtained through student's t-tests; p values less than or equal to .05 (Marôco, 2010) were considered to be statistically significant. Pearson correlations were performed to assess correlation between variables, using the reference values mentioned by Pestana and Gageiro (2008): r < .20 corresponds to a very low correlation; .20 < r < .39 to a low correlation; 40 < r < .69 to a moderate correlation; 70 < r < .89 to a high correlation; and .90 < r < 1 to a very high correlation.
In order to explore whether psychosocial functioning and satisfaction with life had a moderating effect on the relationship between parental resilience and depressive symptomatology of adolescents, hierarchical multiple linear regressions were computed, after checking for respective assumptions. For the moderation analyses, values from the predictor variable (RS23) and moderator variable (psychosocial functioning and satisfaction with life) were standardized, i.e., tailored to a mean of 0 and standard deviation 1, before the interaction term. This procedure of variables standardization reduces potential multicollinearity problems and facilitates the interpretation of the model intercepts. Then, a variable that corresponds to the multiplicative term between the predictor variable – resilience - and the moderator - psychosocial functioning - was created. Three key terms were reached: total of RS23; psychosocial functioning score and the multiplicative term (total resilience * psychosocial functioning). Later, hierarchical multiple regressions were conducted in which resiliency was entered at first as predictive, then the psychosocial functioning was inserted as a possible predictor and in a third step the term of interaction between resilience and psychosocial functioning was inserted for the prediction of depressive symptomatology.
Multiple hierarchical linear regressions were conducted having as a moderator variable the total score of psychosocial functioning and its domains (relationship with family, relationship with friends and recreational activities). However, no significant interactions were found for these variables and for which this data is not described in the results.
3.Results
3.1 Preliminary analysis
Based on the analysis of the Kolmogorov-Smirnov test, it was found that data of the variables
under study did not follow a normal distribution (K-S,
3.2 Descriptive analysis
For descriptive analyses (cf. table
Gender differences were analyzed using Student's t-tests for independent samples (see table
No statistically significant differences were found between genders for the variables satisfaction and parental resilience.
3.3Study of the relationships between resilience, psychosocial functioning and depressive symptomatology
Pearson correlation coefficients were made to analyse the relationships between the variables in study (cf. table
Concerning the association of the variable psychosocial functioning with the CDI, a low positive relation with the total psychosocial functioning was found (
3.4Analyses of prediction effects
Taking into account the results obtained in the correlations, a multiple regression analysis (enther method) for the total sample was computed, in order to understand if resilience, PF and its domains that presented significant correlations with the total of CDI and with life satisfaction, had a significant predictor effect on depressive symptomatology. Results showed that resilience produces a significant model [R2 = .094, F (1) = 13.449, p < .001], able to explain 9.4% of the variance in depressive symptomatology.
With regard to PF domains, results showed a significant model [R2 = .162; F (1) = 6.108, p < .001], explaining 16.2% of the variance of depressive symptomatology. Family relationship (β =. 258, p <. 01) appears as a predictor of depressive symptomatology. The PF domain, relationship with family, contributes significantly and independently to the prediction of depressive symptomatology. This allows us to say that weak family relations are associated with higher levels of depressive symptomatology.
3.5 Analysis of Moderation effects
3.5.1 Study of the Moderating Effect of School Performance in the Relationship between Parental Resilience and Depressive Symptomatology of Adolescents
Hierarchical multiple linear regressions were conducted to verify the existence of a moderating effect of academic performance in the relationship between parental resilience and adolescents’ depressive symptomatology. There was a significant interaction effect between resilience and
school performance (β = - .239, p = .005). Analysing the variables separately, it was verified that resilience is a predictor of depressive symptomatology (β = - .307; p < .001). However, school performance alone is not predictive of depressive symptomatology (β = .128; p = .127) (cf. table
In a first step, resilience was entered as a predictor and, later, school performance was entered.
The variable resilience resulted in a statistically significant model, in the first step
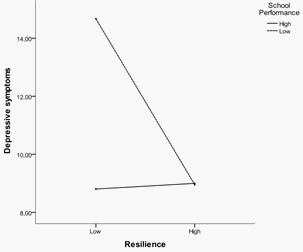
In order to understand the moderating effect of school performance in the relationship between parental resilience and adolescents’ depressive symptomatology, a graphic of the results was computed (cf. Figure
Considering the main effects, it is possible to observe that higher levels of resilience in parents relate to minor depressive symptoms in adolescents, i.e., there is a negative relationship between resilience and depressive symptomatology. A main effect for the variable school performance was not observed, which indicates that this variable alone is not predictive of depressive symptomatology.
With regard to the interaction, it can be said that when parents’ resilience is low, a high school performance leads to lower levels of depressive symptoms, compared to a low school performance. When parental resilience is high, the mean scores of depressive symptoms tend to be similar whether adolescents’ school performance is high or low. This effect is visible in the approach of the graph lines of school performance levels high and low when parents’ resilience is high. In fact, the data allows us to say that parents with high levels of resilience seem to function as a protective
factor for the development of depressive symptomatology when adolescents’ school performance is low.
on the relationship between Resilience and depressive symptomatology.
3.5.2 Study of the Moderating effect of Satisfaction in the relationship between Parental Resilience and Adolescents’ Depressive Symptomatology
Regression coefficients for parental resilience and satisfaction with life evaluated by teenagers were analysed and a significant interaction effect between them was observed (β = -.193, p < .001). Examining the variables separately, it was found that both variables are predictors of depressive symptomatology (Resilience: β = -.307; p < .001; Satisfaction: β = .489; p < .001) (cf. Table
In a first step, resilience was entered as a predictor and, later, satisfaction was entered. The
variable resilience resulted in a statistically significant model in step 1 [
parental resilience. It was found that the interaction term is a significant predictor which together with the two predictors explains 37.0% of the variance in depressive symptoms (cf. Table
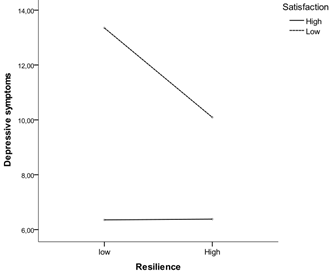
In order to interpret the moderating effect of satisfaction in the relationship between resilience and depressive symptomatology, a graphic of the results was computed (cf. Figure
Regarding the effect of the interaction we can say that when resilience is low, high levels of satisfaction with life lead to lower levels of depressive symptoms when comparing to low levels of satisfaction with life. When levels of satisfaction are high, low or high levels of resilience do not differentiate adolescents in terms of depressive symptomatology, since the mean scores are very similar in low or high resilience. In turn, when resilience is high, low satisfaction tends to differentiate from high satisfaction in terms of prediction of depressive symptomatology. Thus, parents with high levels of resilience seem to act as protective factors of depressive symptoms in adolescents, regardless of the level of satisfaction, since the two lines of satisfaction tend to approach when parental resilience is high.
4.Discussion
In the present study we attempted to verify if parental resilience would have a protective role in the development of depressive symptomatology in adolescents and whether psychosocial functioning would have a moderating effect on the relationship between parental resilience and depressive symptoms in adolescence. The study of this relationship can be useful to the extent that authors argue that environmental factors may emerge as vulnerabilities or protective factors in the development of anxiety disorders, depression and reaction to stress (Nobre, Castro, & Esteves, 2012). Moreover, regarding the development of depression in adolescents, within these environmental factors, we can consider that parental resilience can have an important role. The innovative contribution of our study is investigating this important adolescents’ context variable (parental resilience) assuming that more resilient parents may be more competent at parenting and dealing with life situations, being able to promote more effective coping skills in children. We also studied the effect of one variable that can affect the relationship between parental resilience and depressive symptomatology of adolescents, which is adolescents' psychosocial functioning. The possible mechanisms of action of parental resilience should be investigated in future studies.
Although it was not the primary objective of the study we examined the relationship that gender might have with the variables investigated and in the future we intend to better explore its role in the relations established between parental resilience, psychosocial functioning and depressive symptomatology in adolescents. Results found statistically significant differences between genders with girls presenting more depressive symptoms than boy, which reinforces what has been found in literature (Azevedo & Matos, 2014; Costa, 2011; Resende, Santos, Santos, & Ferrão, 2013). Statistically significant differences between genders were also found for the psychosocial functioning domains, family relationship and school performance. It was found that girls report worse relations with the family and males worse school performance, corroborating studies where these differences were found (Costa, 2011; Gledhil, 2010; Goldstein et al., 2009).
However, we must be careful regarding the generalization of the results, since mostly female participants constitute the sample. It would be important for future research to replicate these data in a bigger sample representative of the two genders.
With regard to the gender of the parents, the results we obtained corroborate data found by Wagnild (2009) and indicate that there are no statistically significant differences between genders concerning resilience.
Results obtained in this research showed a negative association between parental resilience and the presence of depressive symptoms in their children, allowing us to affirm that parents’ resilience acts as a protective factor of depressive symptoms in adolescents. Thus, children of parents with high levels of resilience tend to express less depressive symptoms when compared with children of less resilient parents (Gladstone, Boydell, & Mckeever, 2006; Wong, 2008).
Regarding the relationship between psychosocial functioning and depressive symptomatology, a positive association was found allowing to conclude that when the adolescent presents a suitable psychosocial functioning, including stable relations with family and friends, recreational activities (e.g. theatre groups, sports, television, internet) and a satisfactory school performance, tends to present lower levels of depressive symptomatology. Thus, adaptive psychosocial functioning acts as a protective factor in the development of depressive symptomatology. Regarding the variable satisfaction that the adolescent has with the various areas of his/her life, it revealed a positive relationship with depressive symptomatology. A similar result was found by Costa (2011). These data corroborate results from other studies (Claudino et al., 2006; Goldstein et al., 2009; Greer et
al., 2010; McCabe, 2011) that showed that worse psychosocial functioning is associated with higher levels of depressive symptomatology.
In the present study it was found that a domain of psychosocial functioning (school performance) and the variable satisfaction with life have an interaction effect on the relationship between parental resilience and depressive symptomatology of adolescents.
With regard to the effect of the moderator variable school performance, it is possible to affirm that when parental resilience is low, a high performance leads to lower levels of depressive symptoms compared with a low school performance. That is, the adolescents’ perception as effective seems to act in the prevention of depressive symptomatology. However, when there are high levels of resilience in parents, lower or higher levels of school performance reflect similar levels of depressive symptomatology. Thus, the results obtained in this study allow us to conclude that resilience acts as a protective factor for the development of depressive symptoms when adolescents indicate a low school performance. The results found here can be explained by previous studies (Gladstone, Boydell, & Mckeever, 2006; Wong, 2008), in which more resilient parents showed greater involvement in the life of the adolescent and provided greater support to the adolescent, promoting a more effective emotional self-regulation.
In relation to the results obtained for the variable satisfaction as a moderator of the relationship between resilience and depressive symptoms, it is possible to conclude that when parental resilience is low, high levels of satisfaction with life lead to lower levels of depressive symptomatology. When levels of satisfaction are high, regardless of the levels of parental resilience, levels of depressive symptoms tend to be similar. This fact can be explained considering that adolescents with high life satisfaction are more effective in solving problems and develop appropriate coping strategies, preventing the development of psychopathology. However, when adolescents’ satisfaction with life is low, parents with high resilience act as a protective factor of depressive symptomatology, thus observing a clear diminution in levels of depressive symptomatology when compared with low levels of parental resilience.
The results obtained in this research lead to the conclusion that parents’ resilience, more elevated school performance of the adolescent and their satisfaction with the various areas of life, are protective factors of the adolescent, preventing the development of depressive symptomatology.
It is considered pertinent the replication of data obtained in this study in other samples of the community clinical samples and institutionalized adolescents. In future research it would be interesting to also study the influence of gender on the relationship between resilience and depressive symptomatology.
The collection of information concerning parental resilience levels was conducted by a self-report questionnaire. In future studies, it would be important to conduct face-to-face interviews with the parents to improve the reliability of the information.
Regarding the application of the A-LIFE in the evaluation of adolescents’ psychosocial functioning, it is considered that in future studies would be interesting to assess inter-evaluator reliability. Moreover, to carry out investigations with a longitudinal design could also be advantageous, adolescents at risk of developing depressive symptomatology.
To sum up, it is considered that this research represents a groundbreaking contribution that explores how psychological adaptive characteristics of parents, in particular resilience, may be protective factors in the development of depressive symptoms in adolescents. Understanding the relationship between parental resilience and depressive symptomatology in adolescents and the variables that moderate this relationship can help clinical professionals to intervene at an early stage, by applying depression prevention programs that include a parent component and which promote interpersonal skills and problem solving on the adolescent, to help him/her became autonomous and to grow healthily.
Acknowledgements
We would like to express our gratitude to all the participants that made this study possible and to FCT that funded the study. This work is funded by ERDF – European Regional Development Fund through the COMPETE Program (operational program for competitiveness) and by National Funds through the FCT – Fundação para a Ciência e a Tecnologia (Portuguese Foundation for Science and Technology) within project “Prevention of depression in Portuguese adolescents: efficacy study of an intervention with adolescents and parents” (PTDC/MHC-PCL/4824/2012).
References
- American Psychiatric Association., (2013). Diagnostic and statistical manual of mental disorders (5th.
- (), ed.). Arlington, VA: American Psychiatric Publishing.
- American Psychological Association, (2010). Publication manual of the American Psychological.
- (), Association (6th ed.). Washington, DC: Author.
- Arnarson, E.Craighead, W. (2009). Prevention of depression among icelandic adolescents. Behavior
- (), Research and Therapy, 47, 577-585.
- Arnett, J. J. (1999). Adolescent storm and stress, reconsidered. American Psychologist, 54, 317-326. Azevedo, A., & Matos, (2014). Ideação suicida e sintomatologia depressiva em adolescentes [Suicidal ideation and depressive symptomatology in adolescentes]. Psicologia, Saúde e Doença,15 (1), 180-191. doi: 10.15309/14psd150115 Bahls, S. C. (2002).. Aspectos clínicos da depressão em crianças e adolescentes. [Depression in childhood and adolescence: clinical features] Journal de Pediatria. , 78(5), 359-366, A. P
- Barker, E. D.Copeland, W.Maughan, B.Jaffee, S. R.Uher, R. (2012). Relative impact of maternal depression and associated risk factors on offspring psychopathology.1192/bjp.bp.111.092346 Bauman, S., Adams, J. H., & Waldo, M. (2001). Resilience in the oldest-old.. British Journal of Psychiatry. Counseling and Human Development, 34 (2), 1-19. , 200(2), 10-, 124-129. doi
- Beardslee, W. R.Versage, E. M.Gladstone, T. R. (1998). Children of affectively ill parents: A review of the past 10 Am Acad Child Adolesc Psychiatry,. doi: 10.1097/00004583-199811000-00012 Biederman, J., Petty, C., Hirshfeld-Becker, D. R., Henin, A., Faraone, S., V., Dang, D., Jakubowski, A., & Rosenbaum, J. F. (2006). A controlled longitudinal 5-year follow-up study of children at high and low risk for panic disorder and major depression. Psychological Medicine, 36 (8), 1141-1152. doi: 10.1017/S0033291706007781 Brito, I. (2011). Ansiedade e depressão na adolescência. [Anxiety and depression in adolescence]. Revista Portuguesa de Clínica Geral, 27 (2), 208–214. Retrieved from http://www.scielo.gpeari.mctes.pt/scielo.php?script=sci_arttext&pid=S087071032011000200010&ln g=pt&nrm=iso Brooks, T.l., Harris, S.K., Thrall, J.S., & Woods, E.R. (2002). Association of adolescent risk behaviors with mental health symptoms in high school students.1016/S1054-139X(02)00385-3 Claudino, J., Cordeiro, R. & Arriaga, M. (2006). Depressão e Suporte Social em Adolescentes e Jovens Adultos. Um estudo realizado junto de Adolescentes Pré-Universitários. [Depression and social support in adolescents and young adults]. Educação, Ciência e Tecnologia, 185-196. doi: 10.1590/S0102-79722011000400015 Correia, LL. & Linhares, MBM. (2007). Maternal anxiety in the pre and postnatal period: A literature review. Revista latino-Americana de Enfermagem, 15 (4), 677-683. doi: 10.1590/S0104-11692007000400024 Costa, A. S. (2011).. Journal of Adolescent Health, 31, 240-246. doi: 10. Tradução da Entrevista A-LIFE - Adolescents Longitudinal Interval Follow-up Evaluation - Estudo Preliminar do Funcionamento Psicossocial numa Amostra de Adolescentes Portugueses [Translation of A-LIFE - Adolescents Longitudinal Interval Follow-up Evaluation -. , 37(11), 34-41, years. J
- (), Preliminary Study of Psychosocial Functioning in a Sample of Portuguese Adolescents] (Unpublished master’s thesis). Faculty of Psychology and Educational Sciences, University of Coimbra, Coimbra, Portugal.
- Coutinho, M. P. L. (2001). Depressão infantil: Uma abordagem psicossocial. [Childhood depression: A psychosocial approach]. João Pessoa: UFPB Dunn, A. & Weintraub, Exercise in the prevention and treatment of adolescent depression: A promising but little research intervention.. American Journal of Lifestyle and Medicine. , 2, 207-518, P. (2008)
- Fernandes, L. F. B.Silveira, L. R.Miyazaki, M. C.Domingos, N. A. M.Luiz, A. M. A. G.Micheletto, M. R. D. (2008). Eventos aversivos e depressão na adolescência: Relato de caso.
- (), [Aversive events and depression in adolescence: a case review]. Revista Brasileira de Terapias Cognitivas,4 (1), 65-72.
- BMBoydell, K. M.McKeever, P. (2006). 1016/j.socscimed.2005.10.038 Gladstone T. R. G. & Beardslee W. B. (2009). The prevention of depression in children and adolescents: A Review.. Canadian Journal of Psychiatry. , 54(4), 212-221, resilience. Social
- Gladstone TR, G.Beardslee W, B.O’Connor, B. A. (2011). The prevention of adolescent depression. Psychiatric Clinics of North America, 34(1), 35-52
- Gledhil, J.Garralda, E. (2010). The short-term outcome of depressive disorder in adolescents attending primary care: A cohort Psychiatry Psychiatr Epidemiol, . doi: 10.. 1007/s00127-010-0271-6 Greer, T., Kurian, B., & Trivedi, M. , 46, 993-1002, study. Soc
- Goldstein, T. R.Birmaher, B.Axelson, D.Goldstein, B. I.Gill, M. K.Esposito-Smythers, C.Keller, M. (2009). Psychosocial functioning among bipolar youth.1016/j.jad.2008.07.. Journal of Affective Disorders,– 10. 001 Jaser, S. S., Champion, J. E., Reeslmd, K. L. , 114(1-3), 174-, 183. doi
- (1987). The Longitudinal Interval Follow-up Evaluation: A comprehensive method for assessing outcome in prospective longitudinal studies. Archives of General Psychiatry, 44, 01800180050009 Kline, R. B. (2005).. Principles and practice of structural equation modeling. (2nd ed.). , 10(1001/archpsyc.1987), 540-54. doi
- Kovacs, M. (1985). The Children’s Depression Inventory (CDI). Psychopharmacology Bulletin,.. 995-998. , 21(4)
- Kovacs, M. (2006). New steps for research on child and adolescents depression prevention. American Journal of Preventive Medicine, 31, 008 Kubik, M., Lyle, L., Birnbaum, A., 10(1016/j.amepre.2006.07), 184-185. doi
- Lewinsohn, P.Rohde, P.Seeley, J.Klein, D.Gotlib, I. (2003). Psychosocial functioning of young adults who have experienced and recovered from major depressive disorder during adolescence.
- Marôco, J. (2010). Análise de equações estruturais: Fundamentos teóricos, software e aplicações[Analysis of structural equations: theoretical foundations, software and applications]. Pero Pinheiro: ReportNumber
- Marujo, H. A. (1994). Síndromas depressivos na infância e na adolescência [Depressive syndromes in childhood and adolescence] (Unpublished doctoral dissertation). Faculty of Psychology and Educational Sciences, University of Lisbon, Lisbon, Portugal
- Matos, A. P.Costa, A. (2011). Estudo das propriedades psicométricas da entrevista Adolescents Longitudinal Interval Follow-up Evaluation (A-LIFE). [Study of Psychometric properties of the
- (), interview Adolescents Longitudinal Interval Follow-up Evaluation (A-LIFE)] (Unpublished manuscript).
- McCabe, M.Ricciardelli, L.Banfield, S. (2011). Depressive symptoms and psychosocial functioning in preadolescent children. Depression Research and Treatment, McIntosh, N., Helms, P., & Smyth, R. (Eds.). (2003). Forfar and Arneil's Textbook of Pediatrics.. Edinburgh, Churchill Livingstone. , 1-7. doi:10.1155/2011/548034
- Nilsen, W.Karevold, E.RØysamb, E.Gustavson, K.Mathiesen, K. (2013). Social skills and depressive symptoms across adolescence: Social support as a mediator in girls versus boys. Journal of Adolescence, 36, 005 Nobre, S., Reis, S., Castro, F. V., & Esteves, M. L., 10(1016/j.adolescence.2012.08), 11-20. doi
- Pestana, M. H.Gageiro, J. N. (2008). Análise de dados para as Ciências Sociais: A Complementaridade do SPSS [Data analysis for social sciences – The complementarity of SPSS] (5th ed.). Lisboa: Edições Sílabo.
- Péres, M. V.Urquijo, S. (2001). Depresión en adolescentes. Relaciones con el desempeño académico
- S1413-85572001000100006 Pinheiro, R.Matos, A. P. (2013). Exploring the construct validity of the two versions of the Resilience Scale in a Portuguese adolescent European Journal of Social & Behavioural Sciences. , sample. The
- doi: 10.15405/FutureAcademy/ejsbs, (2301-2218). Pinto, I. C., Fraga, S., & Ramos, E. (2010). Depressive symptoms and alcohol use among adolescents. In Euroepi 2010 Epidemiology and Public Health in an Envolving Europe – Congresso Nazionale AIE.. Florence. , XXXIV, 2012.2.5
- Rao, U.Chen, L. A. (2009). Characteristics, correlates, and outcomes of childhood and adolescent depressive disorders. Dialogues in Clinical Neuroscience, 11(1), 45-62
- Reppold, C. T.Mayer, J. C.Almeida, L. S.Hutz, C. S. (2012). Avaliação da Resiliência: Controvérsia em torno do uso das escalas. Psicologia:Reflexão e Crítica, 25, p. 230-210
- Resende, C.Santos, E.Santos, P.Ferrão, A. (2013). Depressão nos adolescentes – mito ou realidade? Nascer e Crescer. Revista de pediatria do centro Hospitalar do Porto, XXII(3), 145-150
- Saluja, G.achan, R.Scheidt, P.Overpeck M, Sun.Giedd, J. (2004). Prevalence of and risks factors for depressive symptoms among young adolescents. Pediatrics & Adolescent Medicine, Sheeber,, Hops, H., & Davis, B. (2001). Family processes in adolescent depression.. Clinical Child and Family Psychology Review, 4, 19-35. , 158, 760-765, L. B
- Torgalsbφen, A. K. (2012). Sustaining full recovery in schizophrenia after 15 years: Does resilience matter? Clinical Schizophrenia & Related Psychoses, . doi: 4.3., 5(4), 193-200, 10.3371/CSRP.5
- Wagnild, G. (2009a). The Resilience Scale user’s guide for the US English version of the Resilience Scale and the 14-item Resilience Scale (RS–14). Worden, MT: Resilience
- Wagnild, G. (2009b). A review of the Resilience Scale. Journal of Nursing Measurement, –, 17, 105-, 113. doi
- Wagnild, G. M.Young, H. M. (1993). Development and psychometric evaluation of the resilience scale. Journal of Nursing Measurement, 1(2), 165-178
- Wrong, M. M. (2008). Perceptions of parental involvement and autonomy support: Their relations with a self-regulation, academic, performance, substance use and resilience among American Journal of Psychology. , 10(3), 497-518, adolescents. North
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
03 August 2015
Article Doi
eBook ISBN
978-1-80296-005-1
Publisher
Future Academy
Volume
6
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-220
Subjects
Child psychology, psychology, developmental psychology, psychological testing, psychological measurement, family psychology
Cite this article as:
Pestana, C., Matos, A. P., Pinheiro, M. R., Costa, J. J., & Marques, C. (2015). Parental Resilience and Adolescence Depression: Moderating Effect of Children’s Psychosocial Functioning. In Z. Bekirogullari, & M. Y. Minas (Eds.), Cognitive - Social, and Behavioural Sciences - icCSBs 2015, August, vol 6. European Proceedings of Social and Behavioural Sciences (pp. 38-52). Future Academy. https://doi.org/10.15405/epsbs.2015.08.5