
Intervention To Increase Participation in Physical Activity For Adults


Abstract
Physical activity levels in Malaysia adults are low. There is a growing problem of physical inactivity and approximately a quarter of the population report being completely sedentary. Research supports the use of the social cognitive theory in designing physical activity intervention. The aim of the study to increase the level of sedentary and inactive adults to involve in physical activity with selflearning element for helping them to increase participation in physical activity. This study used 12 weeks intervention pre-post quasi-experimental time series design with single subject. 22 volunteer participant (5 men and 17 women) staffs from teaching college in Terengganu completed this study. The inclusion criteria was sedentary (i.e did not participate in regular moderate or vigorous exercise or physical activity for 30 minutes two or more times a week for at least 6 months), inactive, age 20 to 60 years and full-time employee. The intervention consisted personal exercise plan booklet (PEPB), face-to face interaction, counselling session and telephone calls. In-person assessments occurred at baseline and 12 weeks after receiving intervention, which included wearing accelerometer for 7-day, IPAQ short form, as well as a battery of psychosocial questionnaires. Data were analyzed using the descriptive analysis, multiple regression and general linear model repeated-measure as appropriate. 22 volunteer participants (5 men and 17 women) with age mean (SD) = 44.73 (8.51). Accelerometer significantly increased their stepcounts (SD) by 8434.40 (661.10) per day over the baseline. IPAQ showed that mean vigorous intensity (SD) = 1594.55 MET-min week−1 (1306.06), moderate intensity (SD) = 1749.05 MET-min week−1 (1760.35) and walking (SD) = 2146.98 MET-min week−1(2000.32) over the baseline. Multiple regression showed that there was a significant relationship self-efficacy and social support for increasing participating in physical activity after the intervention. Intervention designed to increase participation in physical activity a modestly effective. Intervention should emphasized tailored individual behavioral strategies. Our results suggest that in future studies, learning element should be implement to all ages and population. So they can plan their activities in changing physical activity patterns. This recommendation prompts as a strategy to promote physical activity of the many recommended. Further research is needed to determine factors associated with long-term, sustained, physical activity behaviour, sedentary and inactive adults.
Keywords: Type your keywords here, separated by semicolons;
Introduction
Physical inactivity leads to higher morbidity from cardiovascular disease, stroke, metabolic syndrome, cancer diabetesmellitus type 2, osteoporosis, and mental health [1]. Physical activity levels in Malaysian adults are low. Majority of Malaysian do not meet this recommendation for physical activity and only a small percentage participates in regular and adequate physical activity [2], which may be due to the rapid industrialization and urbanization for the past several decades [3]. The prevalence of physical inactivity among Malaysian men is 37% and women is 43% and this population spent their time (74% of the day) in sedentary activities [3].
Sedentary behavior has been identified as one of the root causes of various risk of death [4] and indirectly connected with the behavior of participation in physical activity [5]. Past studies have shown that participation in regular physical activity can reduce the risk of cardiovascular [6], type-2 diabetes [7], obesity [8], osteoporosis [9], some risk of cancer [10] and depression [11].
Physical activity is actively identified to benefit their health in the long run for all ages, abilities and body size [12]. According to Centers for Disease Control and Prevention, weight control, reduction in the prevalence of noncommunicable disease risk, strengthen bones and muscles, increasing their ability to perform daily activities and increase the chances of a long life is a benefit that can be obtained with sufficient physical activity However the latest challenge faced is to encourage individuals to increase participation in physical activity to be a practice, especially among adults with sedentary behavior in their daily lives [13]. To achieve this, a study in the field of sports science to be developed as a strategy for an individual to get benefit from physical activity.
Exercise is a form of physical activity is structured and designed to achieve a specific purpose [12]. Usually exercise is planned with the aim to improve the physical fitness component. Thus, an individual is recommended to do physical activity of moderate intensity for at least 30 minutes five or more days a week to stay healthy and get the health benefits [14].
Physical activity interventions for adults should be formed by emphasizing strategies to approach the behavior of a cognitive approach [15]. Previous studies demonstrated the effectiveness of behavioral interventions to improve physical activity in which the standards of behavior interventions to better demonstrate the effectiveness of the intervention
compared to the use of cognitive measures [8]. The intensive physical activity for 10 weeks showed effectiveness in weight loss and reduce the risk of cardiovascular disease in adults who suffer from overweight [16].
Previous studies using intervention strategies focused on individuals is limited. This is supported by McCarthy et al (2002) that further studies should focus on individuals to increase physical activity to meet the needs based on their goals. The program focuses on individuals is an effective strategy for specific goals can be accomplished either to improve their health or fitness level [17].
Social Cognitive Theory [18] form the basis of intervention studies in which psychosocial factors (self-efficacy and social support) to be predictive factors have been shown to be effective to increase the physical activity of a variety of adult populations. Self-efficacy of an individual's beliefs about their ability to perform is very important for an individual to remain and abide in physical activity as a routine in the lives of study participants. Self-efficacy has been successful in increasing physical activity in which the higher the self-efficacy of an individual, the higher the achievable goals [18].
As Malaysian adults are less physically sufficient active, one needs to start interventions that influence behavior associated with sedentary, inactive and full time workers. Therefore, the focus of this study is to increase the participation of adults in physical activity that emphasizes the elements of individual learning by doing moderate-intensity physical activity to increase knowledge and acquire skills specific behaviors that enable them to increase physical activity to achieve health benefits and be a best practice.
Methods
Study design
A 12 weeks quasi-experimental time series pre post design with single subject. Randomized technique was adopted, in which the selection of participants was based on predetermined selection criteria and willingness to participate. Participants’ recruitment was conducted from September 2013 to November 2013 using email notices, flyers, and word of mouth from potential participants. Specific inclusion and exclusion criteria were attached in the advertisements. Prior, to the screening, interested participants would be contacted to ensure they fulfilled the listed criteria and only qualified participants were allowed to attend the screening session. Sampel size calculation showed that a minimum number of 16 participants were required for this study.
Participants
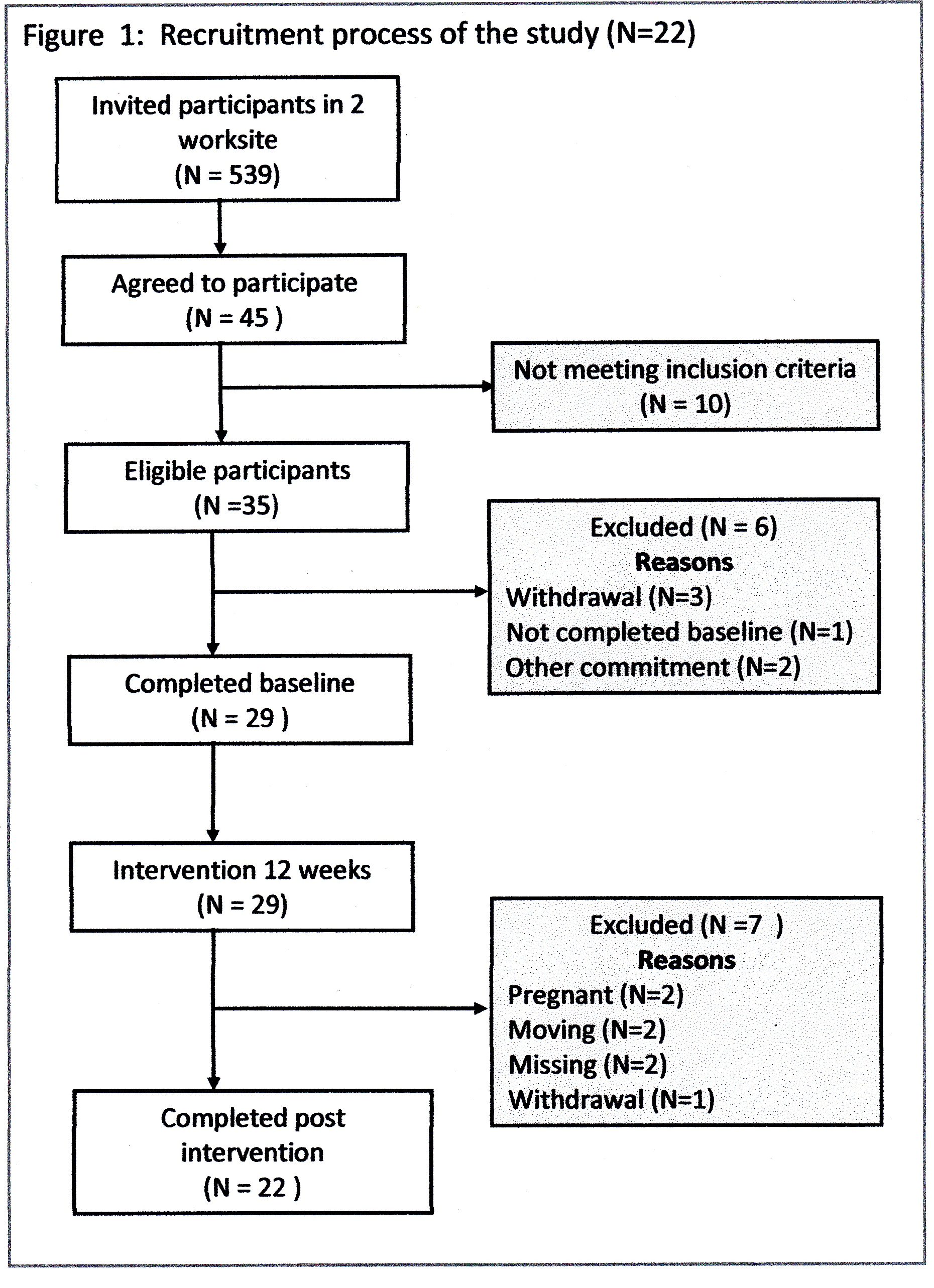
Volunteer participants from teaching college and university staffs completed in this study included 22 participants (5 men, 17 women) ranging in age from 20 to 60 years, with mean age 44.738.51. Sixteen participants (four men and twelve women) were excluded from the analyses due to withdrawal, missing, outside commitment, pregnant and moving. The inclusion criteria was sedentary, inactive (i.e did not participate in regular moderate or vigorous exercise or physical activity for 30 minutes two or more times a week for at least 6 months), age 20 to 60 years and full-time workers. All participants were healthy and no serious medical conditions that could limit participation in moderate physical activity, such as unstable angina, uncontrolled hypertension, diagnosed or hospitalized with chest pain, heart attack or heart surgery in the past 6 months and no severe functional impairments due to multiple medical or psychiatric conditions and willing to give full of commitment in participating in physical activity. All participants provided written, informed consent. Medical clearance screening was undertaken using the Physical Activity Readiness Questionnaire (PAR-Q) [19]. The recruitment process of the study in Figure 1.
Procedure
The behavioural impact of the intervention was assessed over 12 weeks intervention period. Therefore in time series design the baseline and post test data assessment had two point measurement. The primary outcome measure was accelerometer step count [20]. Accelerometer data were collected over a 7-day period. A secondary measure of physical activity was conducted using the International Physical Activity Questionnaire (IPAQ short form version and self-report) [21-22]; a 7-day recall utilised to assess the domain and activity type of potential changes in activity. Meanwhile to measure self-efficacy and social support variable, Self-Efficacy for Exercise Regulation [23] and Social Support for Exercise [24] were used.
The baseline assessment consisted of two study visits scheduled one week apart. At the first visit, informed consent was obtained, demographic data were collected and participants were given an accelerometer to wear for the next seven days. Seven days after the participants’ initial visit, participants returned their accelerometer. Two weeks after returning accelerometer, participants completed physical activity and psychosocial data. Psychosocial and physical activity data were collected again at 12 weeks assessment (post intervention).
The intervention consisted personal exercise plan booklet (PEPB), face-to face interaction and telephone calls. PEPB guided participants to choose activities that took into account their health, preferences, and abilities. It offered information on ways for them to exercise safely, motivate themselves, overcome barriers, and develop a balanced exercise regimen. Participants were requested to engage in moderate-intensity physical activity and increase their current physical fitness level.
Participants received a 30 minute physical activity consultant (face-to-face interaction and counselling session) in week 1 from the member trainer. Minimal amount of face-to-face and counselling contact was necessary for behaviour change. Moreover, the potential for greater participant adherence exists, because participants are able to engage in the intervention at their own convenience. The participants were motivated by trained member to incorporate lifestyle physical activity. PEPB was adopted as a motivational and feedback tool to monitor their daily physical activity and their current fitness levels. Following the 12 week intervention programme, participants were received five short telephone consultation in week 2, 3, 5, 7 and 10. Participants received individual physical activity consultation focusing on relapse prevention strategies, encouragement and maintenance of activity. The main self-learning elements of the brief were goal setting and self-monitoring.
Self-report data
Physical Activity
The self-reported, validated short form of the Malay version of International Physical Activity Questionnaire – Short Form (IPAQ-SF) was used to assess levels of physical activity among participants for the last 7 days [21]. The IPAQ short form was self-completed via e-mail. Participants were asked to recall the type and duration of their physical activities in the last 7 days. For the analysis of physical activity data, the following MET-values were used: walking = 3.3 METs, moderate physical activity = 4.0 METs and vigorous physical activity = 8.0 METs. The results were presented as the estimation of energy expenditure in metabolic equivalent-minutes per week (MET-min week−1). The MET-min week−1 was calculated as follows: minutes of activity/day×days per week×MET-value. From this continuous variable of total physical activity scores, the data were categorized according to the IPAQ scoring guidelines. Participants with a total physical activity of <600 MET-min week−1 were classified in the ‘low’ category, 600–2999 MET-min week−1 in the ‘moderate’ category, and ≥3000 MET-min week−1in the ‘high’ category [25].
To collaborate self-report physical activity findings, participants were asked to wear Actigraph accelerometer for a seven day period at both baseline and 12 weeks (post intervention). Participants wearing accelerometer-measured step count was measured over 7 days at baseline and again for 7 days immediately post-intervention used a 1-minute epoch. Participants were instructed to put on the monitor at the beginning of the day and take it off before bedtime (excluding shower, and water activities). Participants were given verbal and pictorial description as the correct monitor placement and were called the day prior to wearing the monitor as a reminder. Participants were prompted to follow the same day sequence at all assessment time points during the study. Additionally, participants completed a log documenting the time that they wore the accelerometer. The log was returned in person, along with the monitor.
Self-Efficacy
The Self-Efficacy for Physical Activity Scale (SEPA) scale is a ten-item scale with five-point Likert response levels assessing respondents’ confidence in their ability to be physically active despite common barriers (adverse weather, lack of time, when tired, in a bad mood, or on vacation). A summary score is calculated by averaging responses to all ten items, yielding a possible range of one to five points. Higher scores reflects higher levels of self efficacy for physical activity [26]. The SEPA has shown strong internal consistency across multiple studies (r = 0.76 – 0.85) and significantly differentiates individuals in different stages of exercise behavior change [26-27]. Four week test-retest reliability is 0.89. Construct validity has been supported through association with numerous measures of physical activity [27].
Social Support
The Social Support for Exercise Survey [24] measured social influences associated with performance of physical activity. This ten-item questionnaire asks participants to rate their level of agreement using a 5-point Likert scale with 10 statements regarding how often their family and friends provide support for exercise. The Social Support for Exercise has demonstrated adequate test-retest reliability (0.79 and 0.77 for the family and friends scales respectively, p<0.0001) [24] and had internal concistency estimates (Cronbach’s alpha) ranging from 0.84 to 0.95 in the present study.
Data Analysis
Data analysis was performed with SPSS 20.0 for Windows (SPSS, Inc., Chicago, IL). All statistical tests were two-sided and the significance level was set at p<0.05. Confidence intervals were estimated at the level 95% level. Descriptive statistics were used to describe the main characteristics of the study sample. For these characteristics the baseline and post intervention were analyzed with repeated measure Analysis of Variance (ANOVA) was used to evaluate the effects on change over time (group x time effect). Multiple regression analysis and discriminant function analyses was used to determine which variable discriminate between each other. Effect sizes (ES) were calculated using Cohen (1988). ES <.20 indicated a low effect, between 0.50 and 0.80 a moderate effect, >0.80 high effect.
Results
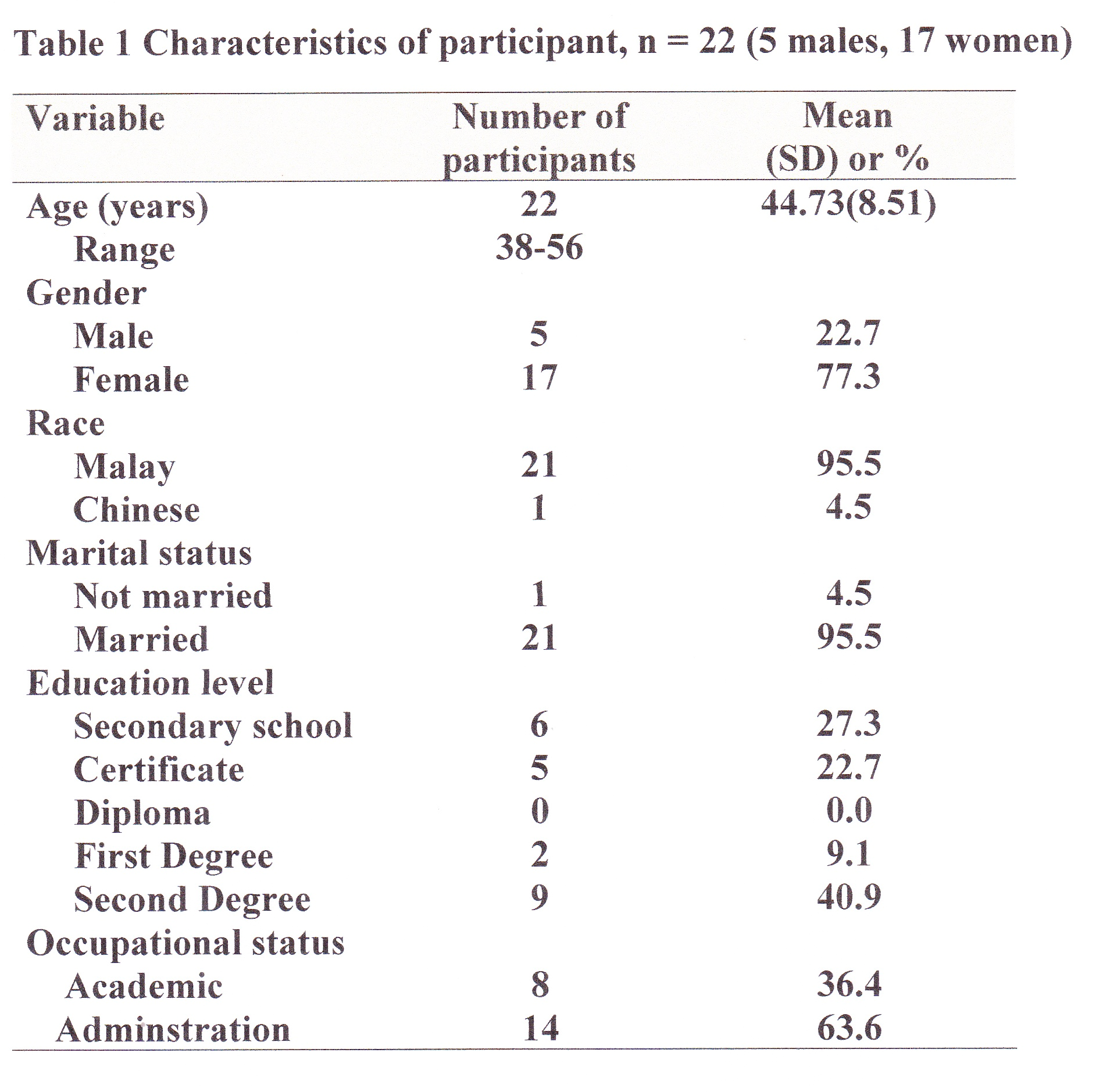
A total of the 35 participants in this study, 22 completed 12 weeks intervention study with a response rate 62.9%. Thirteen participants were lost due to study because of withdrawal, missing, pregnant, other commitment and moving to other places. Demographics characteristics are highlighted in Figure 2. Research participants (N=22) were predominantly female (77.3%) and male (22.7%), with mean age of 44.73 8.51. Most of the participants were Malays (21, 95.5%), married (21, 95.5%) and had studied up to a second degree (9, 40.9%). Most of the participants were administration staff (14, 63.6%). The physical characteristics of the participants are shown in Figure 2.
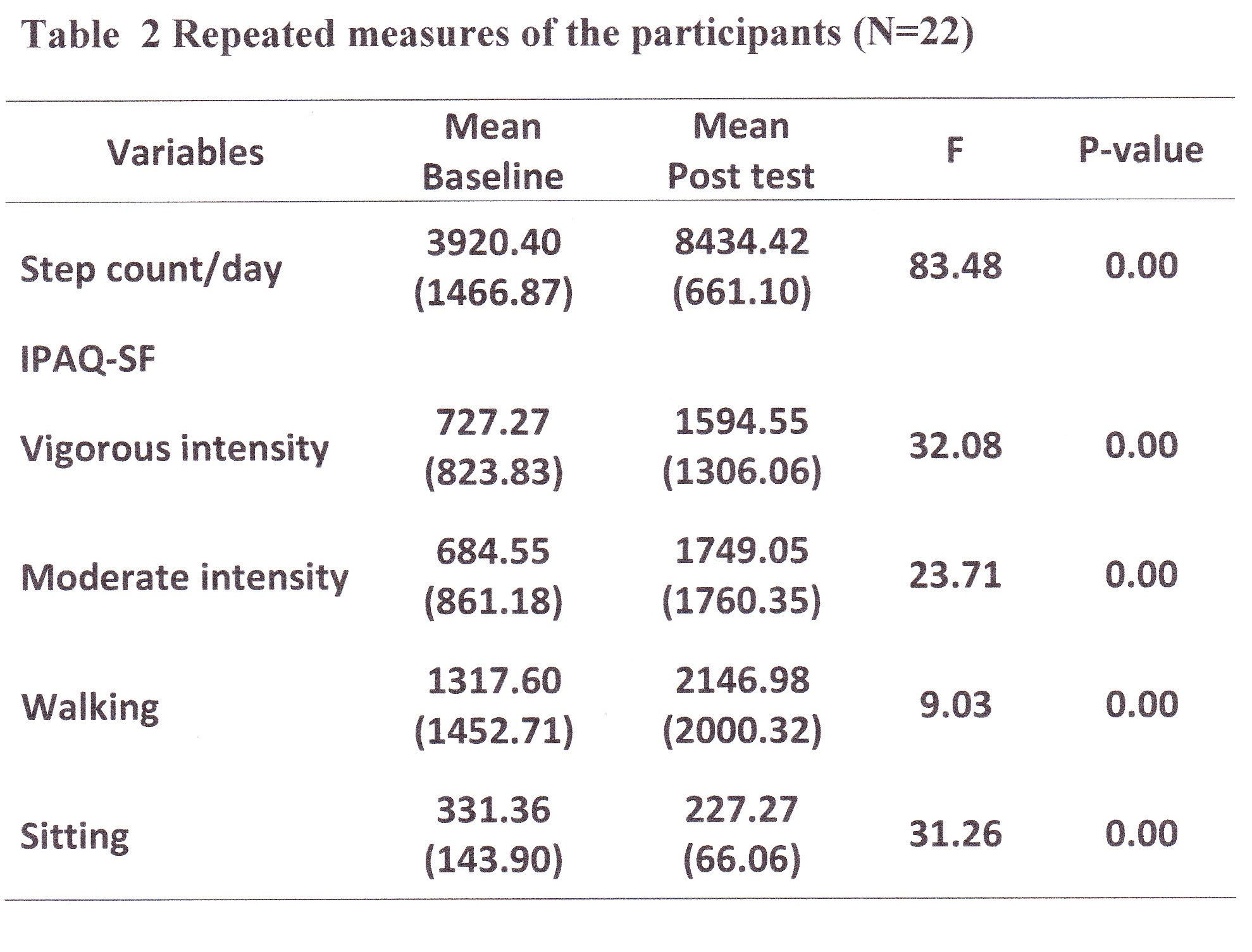
A significant main effect of time ( < 0.001) was found for accelerometer step-counts attributable to significant
increases in steps/day mean (SD) post intervention = 8434 steps/day (661.10) over the mean steps/day baseline (SD) = 3920.40 (1466.87), p < 0.00. Meanwhile IPAQ-SF variables showed that there were significantly increased in vigorousintensity (SD) = 1594.55 MET-min week−1 (1306.06), p < 0.00; moderate-intensity (SD) = 1749.05 MET-min week−1 (1760.35), p < 0.00 and walking (SD) = 2146.98 MET-min week−1 (2000.32), p < 0.00 over the baseline. The repeated measures results are shown in Figure 3.
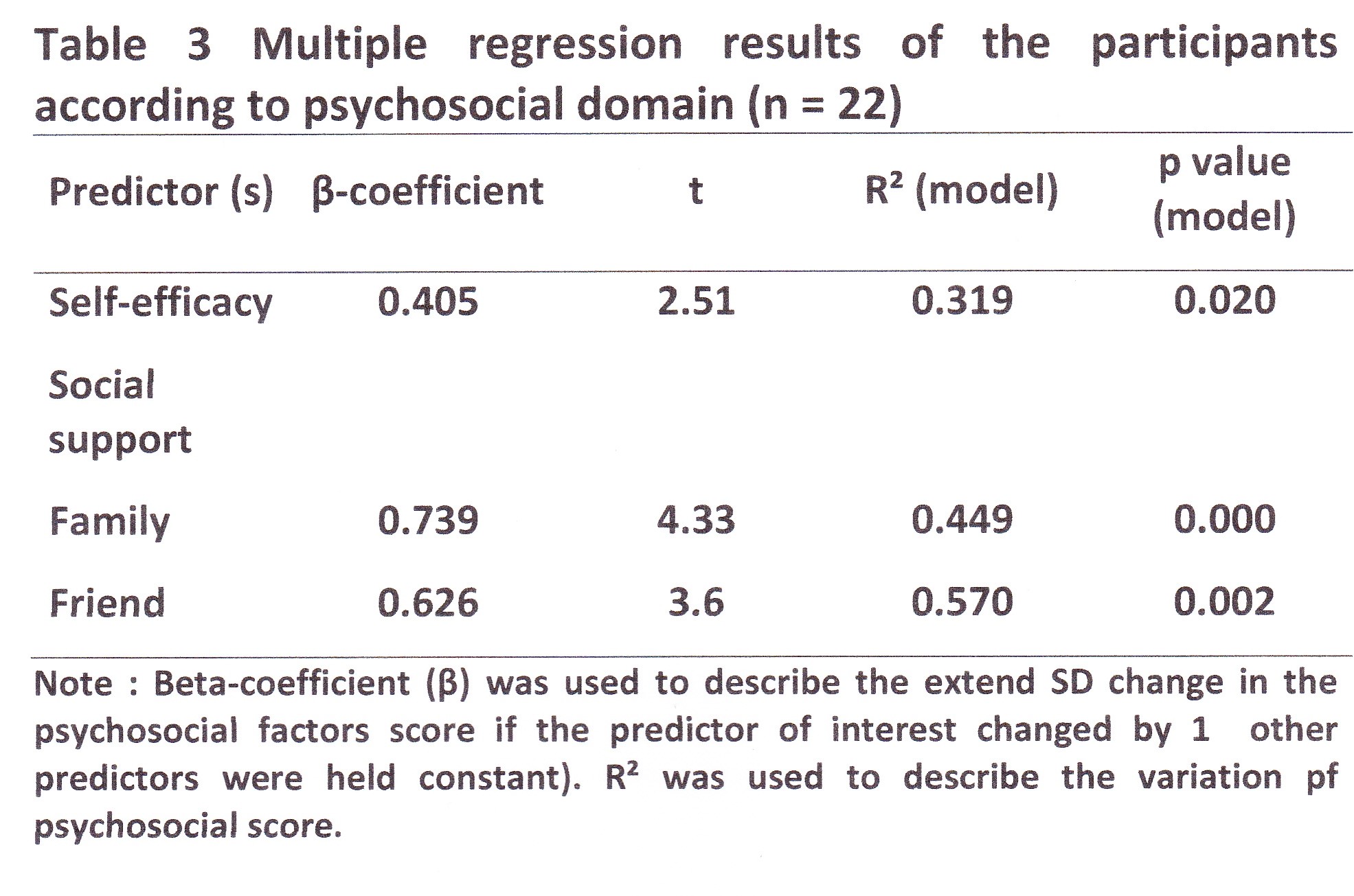
Stepwise linear regression was conducted for each variables in psychosocial factors. Three independent predictor variables on the dependent variables of self-efficacy, social support (family) and social support (friends) (F3, 18 = 10.27, p = <0.05). For self-efficacy, social support (family, friend) were selected as the significant predictors of the psychosocial factors to increase participant in physical activity. Self-efficacy as predictors of giving the β = 0.405, t = 2.51, p = 0.02, p < 0.05, and R ² = 0.319. As for social support (family) gives β = 0.739, t = 4.33, p = 0.000, p < 0.05, and R ² = 0.449. Social support (friends) showed that β = 0.626, t = 3.58, p = 0.002, p <0.05, and R ² = 0.570. This finding suggests that self-efficacy contributed to the increasing number of steps/day was 31.9%. As for social support (family) donated by 44.9% and social support (friends) was 57.0%. Multiple regression results of the participants according to psychosocial domain are shown in Figure 4.
Discussion
The main goal of the study conducted on sedentary, inactive and working full time is to increase participation in physical activity. The results show the effectiveness of interventions that emphasize self-learning elements of adult. Results in a short period of time has shown succeed in increasing the number of steps and participation in physical activity. Self-efficacy and social support can be extended over a period of time. Due to the risk of metabolic syndrome in adults is increasing and the increase is significant with age, especially in urban areas [29], then interventions that emphasize self-learning element can be one of the best efforts in promoting health. The study also showed that behavior change is a very important for participants to achieve the goal of achieving good health and reduce the risk of diseases.
Using the accelerometer is one of the best practice to motivate and inspire greater confidence in achieving goals in physical activity. The effectiveness of physical activity interventions conducted in adults indicate success as the implications of this study as prevention of metabolic syndrome and increase the level of physical fitness as a whole in the future. When designing the type of intervention to a population, it is important to consider what kind of needs and effective strategies to increase the adult participation in physical activity. Self-learning elements conducted in this study could directly increase self-knowledge and skills in planning for physical activity.
Studies have also shown success in improving self-efficacy in the participants to increase involvement in physical activity. Increased self-efficacy for participants in the study is very important as a mediator in the effect of physical activity interventions [30]. In adults, social support is described as having a supportive partner or engage in physical activity group [31]. Intervention is built using social support has been identified as a strong motivator to do engage in physical activity [32] as the majority of the study participants showed increased participation in physical activity. Treiber found similar trends and find social support increased participation in physical activity survey participants where friendship and support from family members and friends who have formed during the intervention study carried out [33]. Study participants reported having a unique relationship between the family and colleagues and beneficial to increase participation in physical activity. Nevertheless a follow-up study should be conducted to see the retention of adult participation in physical activity when designing future interventions on how to maintain social support as a motivator to increase participant in physical activity.
Conclusion
Participants reported promising increases in physical activity, self-efficacy regulation for physical activity and social support over the duration of the study. These findings, in conjunction with self-reported questionnaire, indicate that perhaps the most beneficial applications self-learning elements for promoting physical activity were self-monitoring and also increase their knowledge and skill in participant in physical activity.
The little increases in step-count, physical activity, self-efficacy and social support in short time give the positive effect for adults in changing behavioral pattern in physical activity. Finding from the current study provide some preliminary support for the use of self-learning elements approach to promoting physical activity among sedentary, inactive and full-time adults. Future studies with larger samples are needed to further evaluate the physical activity and psychosocial variables to promoting physical activity among Malaysian adults.
Acknowledgements
We thank all participants and colleagues for their support and valuable time given for this study.
References
World Health Organization. Global strategy on diet, physical activity and health. Available from: http://www.who.int/dietphysicalactivity/goals/en/index.html; 2009 [cited 30 April 2009].
Poh BK, Safiah MY, Tahir A, Siti Haslinda MD, Siti Norazlin N, Farina Z, Mohd Hasyami S. (2008). Physical activity of adults aged 18 to 59 years. Putrajaya: Putrajaya; [Malaysian Adult Nutrition Survey 2003. Volume 6]
Poh BK, Safiah MY, Tahir A, Siti Haslinda MD, Siti Norazlin N, Norimah AK, Wan Manan WM, Mirnalini K, Zalilah MS, Azmi MY, Fatimah S. (2010). Physical activity pattern and energy expenditure of Malaysian adults: findings from the Malaysian Adult Nutrition Survey (MANS). Mal J Nutr 16(1):13-37.
Rossi A, Dikareva A, Bacon SL, Daskalopoulou SS. (2012). The impact of physical activity on mortality in patients with high blood pressure: a systematic review. Journal of Hypertension 30(7):1277 – 1288.
Samitz G, Egger M, Zwahlen M. (2011). Domains of physical activity and all-cause mortality: systematic review and dose-response meta-analysis of cohort studies. International Journal of Epidemiology 3:1-19.
Amin-Shokravi F, Rajabi R, Ziaee N. (2011). Exercise Effects on Risk of Cardiovascular Disease among Iranian Women. Asian Journal of Sport Medicine 2(1):37-43.
Thomas DE, Elliot EJ, Naughton CA. (2006). Exercise for type 2 diabetes mellitus. Cochrane Database System Rev 19(3):CD002968.
Jakicic JM, Davis KK. (2011). Obesity and physical activity. Psychiatric Clinic of North America 34(4): 829-840.
Nordstrom A, Tervo T, Hogstrom M. (2011). The Effect of Physical Activity on Bone Accrual, Osteoporosis and Fracture Prevention. The Open Bone Journal 3(11): 11-21.
McTiernan A. (2006). Cancer Prevention and Management Through Exercise and Weight Control. Boca Raton: Taylor & Francis Group, LLC.
Chalder M, Wiles NJ, Campbell J, Hollinghurst SP, Haase AM, Taylor AH, Fox KR. (2012). Facilitated physical activity as a treatment for depressed adults: randomized controlled trial. BMJ 344: e2758.
Bird SR, Smith A, James K. (2002). Exercise Benefits and Prescription. Nelson Thornes Ltd: United Kingdom.
Lawton R, McEachan RRC, Jackson C, Conner M. (2009). Increasing physical activity: designing and testing a workplace intervention: FINAL RESEARCH REPORT. Institute of Psychological Sciences, University of Leeds.
American College of Sports Medicine. (2010). ACSM’s Health-Related Physical Fitness Assessment Manual (3rd ed.). Human Kinetics: USA.
Conn VS, Hafdahl AR, Cooper PS, Brown LM, Lusk SL. (2009). Meta-analysis of workplace physical activity intervention. American Journal of Preventive Medicine 37(4): 330-339.
Thorndike AN, Healey E, Sonnenberg L, Regan S. (2011). Participation and cardiovascular risk reduction in a voluntary worksite nutrition and physical activity program. Preventive Medicine 52(2): 164 – 166.
Kahn EB, Ramsey, LT, Brownson RC, Heath GW, Howze EH, Powell KE, Stone EJ, Rajab MW, Corso P. (2002). The effectiveness of Intervention to Increase physical activity. American Journal of Preventive Medicine 22(4S).
Bandura, A. (2006). Guide For Constructing Self Efficacy Scales In Pajares F, Urdan, T. (2006). Self-Efficacy Beliefs of Adolescents. Information Age Pub.
Thomas S, Reading J, Shephard RJ (1992). Revision of the Physical Activity Readiness Questionnaire (PAR-Q). Can J Sport Sci 17(4): 338–345.
Cain KL, Geremia CM. (2011) Accelerometer Data Collection and Scoring Manual For Adult & Senior Studies. San Diego State University, San Diego, CA.
IPAQ, 2005. International Physical Activity Questionnaire. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)-Short and Long Forms from http://www.ipaq.ki.se/scoring.pdf 25/1/2012.
Craig CL, Marshal AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF, Oja P. (2003). International physical activity questionnaire: 12-country realibility and validity. Medicine and Science in Sport and Exercise 35(8):1381-1395.
Bandura, A. 2006. Guide For Constructing Self Efficacy Scales In Pajares, F. & Urdan, T. 2006. Self-Efficacy Beliefs of Adolescents. Information Age Pub.
Sallis JF, Pinski RB, Grossman RM, Patterson TL, Nader PR. (1988). The development of self-efficacy scales for health-related diet and exercise behaviors. Health Education Research, 3, 283-292.
Bauman A, Bull F, Chey T, Craig C, Ainsworth B, et al. (2009) The International Prevalence Study on Physical Activity: results from 20 countries. Int J Behav Nutr Phys Act 6: 21.
Marcus BH, Owen N. (1992). Motivational readiness, self-efficacy and decision-making for exercise. Journal of Applied Social Psychology 22:3-16.
Owen N, Marcus H. (1992). Motivational readiness, self-efficacy and decision –making for exercise. Journal of Applied Social Psychology, 22:3-16.
Cohen L, Manion L. (1980). Research method in education. London Groom Helm.
Mohamud WN, Ismail AA, Sharifuddin A, Ismail IS, Musa KI, et al. (2011) Prevalence of metabolic syndrome and its risk factors in adult Malaysians: results of a nationwide survey. Diabetes Res Clin Pract 91: 239–245. doi:
Olander EK, Fletcher H, William S, Atkinson L, Turner A, French DP. (2013). What are the most techniques in changing obese individuals’ physical activity self efficacy and bahaviour: a systematic review and meta-analysis. Inter J Bahav Nutr Phys Act 3:10-29 doi:
Bandura A. (2004). Health promotion by social cognitive means. Health Education and Behavior 31:143-164.
Plotnikoff RC, Brunet S, Courneya K, Spence J, Birkett N, Marcus B, Whitely J. (2007). The efficacy of stage matched and standard public health materials for promoting physical activity in the workplace: The Physical Activity Workplace Study (PAWS). American Journal of Health Promotion 2007, 21:501-509.
Treiber FA, Baranowski T, Braden DS, Strong WB, Levy M, Knox W. (1991). Social support for exercise: relationship to physical activity in young adults. Prev Med 20(6):737-750.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
14 May 2014
Article Doi
eBook ISBN
978-1-80296-000-6
Publisher
Future Academy
Volume
1
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-236
Subjects
Social psychology, collective psychology, cognitive psychology, psychotherapy
Cite this article as:
Mahmood*, M., Koh, D. C. L., & Salamuddin, N. (2014). Intervention To Increase Participation in Physical Activity For Adults. In Z. Bekirogullari, & M. Y. Minas (Eds.), Cognitive - Social, and Behavioural Sciences – icCSBs 2014, vol 1. European Proceedings of Social and Behavioural Sciences (pp. 123-134). Future Academy. https://doi.org/10.15405/epsbs.2014.05.15