
Explore Closely but Remote During the Corna Period


Abstract
The Israeli healthcare system is a universal system, based on the National Health Law of 1995, which mandates all citizens in the country to join one of four official health medical organizations (HMO's), known as Kupat Holim. (Clallite,Macabi,Meuhedet and Leumit) ,are non-profit public organizations. They provide community health services; some provide hospitalization services. The Research Aims to investigate the cultural and social aspects associated with implementation of the National Health Law at the Arab societies, regarding the phenomenon of independent clinics in Arab villages and cities (Muslim, Christian, and Druze). To develop a new conceptual framework regarding new methods of motivating independent physicians in addition to the monetary rewards that is in use today, to examine the physicians and managers attitudes towards continuing and expanding the model of independent clinics in Arab society. The preliminary findings showed that all managers and physicians of the independent clinics are familiar with the law, emphasizing the issue of equality (especially of rights). Physicians consider the financial reward an important factor when signing the contract and a motivating factor for the continuation of it. Physical conditions, technology and advanced training are seen as equally important factors but come after the financial reward. Publicly praising them with the same specific reward is better than just writing a letter and filing it in the personal file. Most physicians agree that the method of operating independent clinics should be continued compared to only 50% of managers who prefer not to continue with the method.
Keywords: Health Insurance Law, HMO's -Health medical organization, independent clinics, Incentive system, Special societies
Main Text -(The Theoretical Rationale of the Study)
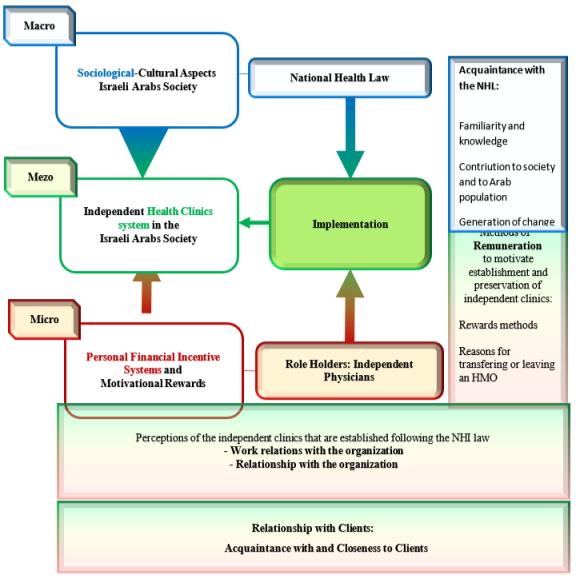
The topic of the current research is the different cultural and social aspects of implementing the Israeli National Health Law, i.e., exploration of the phenomenon of the "Independent Health Clinics" in the Arab societies in Israel (Muslim, Christian, and Druze).The conceptual framework includes the following: research disciplines: Sociology of health services, culture and multiculturalism, public health services: Institutions or organization (in this study: "Independent Health Clinics") and rewards (in this study: remuneration incentives).This research present all methods of remuneration incentives that are known and used, including models of communication with HMOs. At the end proposing major and motivating alternatives which may reinforce physicians' commitment and loyalty to an HMO. The product of the law was an increase in the accessibility of health services and their distribution throughout the country, the lack of physicians at the Arab society, especially in the periphery, and at the same time the competition to get every client forced the HMOs to change and expand the concept of operating the medical services. One of the ways in which the HMOs operated was to build independent clinics through independent Arab physicians, entrepreneurs, or associations. The Independent physicians and clinics exist in all the HMO, physicians can work during the day as a salaried worker and in the afternoon and in the evening to find themselves working as independent physicians in their clinic. Some also combine activity in the morning and swing between being an employee and an independent physician, some work as independent physicians full-time and continue their work in other places such as a hospital, there is no fixed law regarding the form of their employment, some have received permission to work in the area where they work as employees and others are allowed to work in another area. Many professional physicians were allowed to work as independent primary care physicians in their own independent clinics. In Maccabi and Clallit, HMOs some physicians work independently within the central HMO, not in their private independent clinics, the majority still work privately. By 2001, about 2.5 million clients received medical services from independent physicians, about 40% of the residents of Israel, Maccabi and Cllalit were the first HMOs that employed independent physicians, Leumit and Meohedit joined later (Bin Nun et al., 2020). There are several contract methods with independent clinics, one of them is provide services to one or more HMOs under a contract in return to payments according to the numbers of patients (might attend or not the clinic) that belonged to this clinic.
The physicians' behavior and function within different medical organizations is influenced by the various incentive systems: (1) Moral incentive –which is related to the professional ethic and individual professional considerations of the physician, and is rooted in the physician's sense of social mission; (2) social incentive –which is related to external considerations and to the physician's work environment; (3) material incentive –material rewards have an impact on various measures of medical personnel’s actions, including professional behavior and commitment (Vardi et al., 2008). Other researchers focused on the material incentive (Chaix-Couturier et al., 2000), moral incentive (Ostbye et al., 2005) and social incentive content (Brassey et al., 2001). Some of research focused on the national health insurance law without referring to its consequences on the independent clinic phenomena (Horev & Keidar, 2010). Followed literature review, it seems that no previous research has investigated the cultural and social aspects associated with implementation of the National Health Law in the Israeli Arab society regarding the phenomenon of independent health clinics. The incentive model of the independent physicians has not been studied yet. The Ministry of Health’s (M.O.H) regulation is not involve directly and it might need to be more in the future.
The current research – mix methods design, the article is related to the first study
The research methodology is mixed, qualitative, and quantitative, with qualitative being the first. To examine the phenomenon through the eyes of the managers and the physicians, it was necessary to collect data, it was decided that the data collection would be done through interviews and by general contract analysis. No structured interview guides were found from other studies and therefore guides for managers and physicians were constructed structured, reliable, and valid.
Qualitative research: Interviews with: (1) independent physicians who work in their own clinic and manage them; (2) General and professional managers of clinics and districts (see table 1). (3) Documental analysis – Reviewing Documentation (internal general contract as example) as a basic for the study.
Following analysis and summary of findings and conclusions from the interviews: -
Stage B – Quantitative research begun by constructing and validating a survey questionnaire and selecting participants (physicians and managers) from all four HMOs
The research aims
To investigate the cultural and social aspects associated with implementation of the National Health Law in the Israeli at the Arab-Muslim, Christian, and Druze societies, regarding the phenomenon of independent health clinics in Arab villages and cities.
To develop a new conceptual framework regarding new methods of motivating physicians in addition to the material rewards that is in use today, in the context of independent health care services in the Israeli Arab societies.
To examine the physicians and managers attitudes towards continuing and expanding the model of independent clinics in Arab society in Israel.
The research questions
How does the implementation of the National Health Law affect the foundation of independent health care clinics in the Arab societies in Israel (cultural and social aspects) according to physicians and managers?
What are the main components of methods of motivating physicians, in addition to the existing material rewards according to physicians and managers?
Should the idea and the model of independent clinics in Arab society in Israel Continue? and perhaps expand according to physicians and managers?
The research hypothesis
Both physicians and managers agree that the NHI law has changed the way the independent clinic model operates in the Arab society.
All three method of remuneration are important to establish and preserve independents clinics in the
Arab society:
Social and moral incentives are important while the physician signs a contract.
Financial rewards are important for the preservation of physicians in the independent clinic.
Combining three types of rewards (social, moral, and Financial) into one motivational remuneration system for independent physicians will lead to formulating a standard contract, regarding terms of their occupation.
Both physicians and managers will agree that the idea of independent clinic model operates in Arab society should continue and perhaps be expanded
Participants
Interviews with physicians (six men) and seven managers (Five men and two woman) from two competing HMOs
Most are from the Arab sector (Muslim, Christian and Druze). One manager - Jewish
Age and Seniority: Physicians - Age - Mean 58.3 (46-69) / Seniority - Mean 31.2 (19-43)
Independent physicians
General regional managers, 2. Professional regional managers
General district managers, 2. Professional district managers
Method of sampling in qualitative research
A non-probabilistic method, Convenience-Availability Sampling. The method allows flexibility, while gathering data, and broadens the ability to select profile of requested population (Patton, 1998). The managers and physicians were not randomly selected. They represent Two HMOs equally. All belong to the Arab society (Muslim, Christian and Druze), another interviewee who is not an Arab, a physician and a manager who until recently worked at one of the HMOs and moved to another. She represents the other who does not belong to the Arab society.
To summarize the sampling methods performed at the qualitative research stage by Stratified sampling, physicians and managers by HMO, from two HMOs and by an Arab society from the three religions. Inside the strata sample - a non-random convenience availability sample was performed.
Instrument: Interview Guides (see figures 01-04)
Based on the literature review, National Health Insurance Law of 1994-1995.
Validation of its content, construct, and face validity- for the population of Physician and Manager.
Ensuring relevance and ability to answer the research aims, questions, and hypotheses.
Content Analysis of the answers to the interviewer's questions was done by the researcher.
A sample of questions’ answers were analyzed by one manager and one physician (to ensure. content and construct validity)
Examination of interview’s guide validity (content, construct, and face validity)
Four expert judges validated the interview guide. (Content and construct validity):
The validators were asked several questions:
Are the questions included in the interview guide appropriate for the research topic? (Suitable, compatible).
Do the questions encompass and summarize the research topic? (Inclusiveness).
Are there any other questions to add to the interview guide that are relevant to the research? If so please suggest a suitable wording.
Are there any unnecessary questions that are irrelevant to the topic and that can be left out? Why? (Exclusiveness)
Is the wording clear to the interviewees? (Face validity)
Their answers were briefly summarized in writing.
Following the consultation with them, changes were made to the interview guide
Validation: Validation by conducting an interview in practice
Physician - Strengthen the existing one, asked us to address and asked about the importance of updating the knowledge and specialization among the independent physicians and integrating them as they do with the physicians in the regular clinics.
Manager - Had nothing to add but reinforce the guide, praising the idea and wishing success in research.
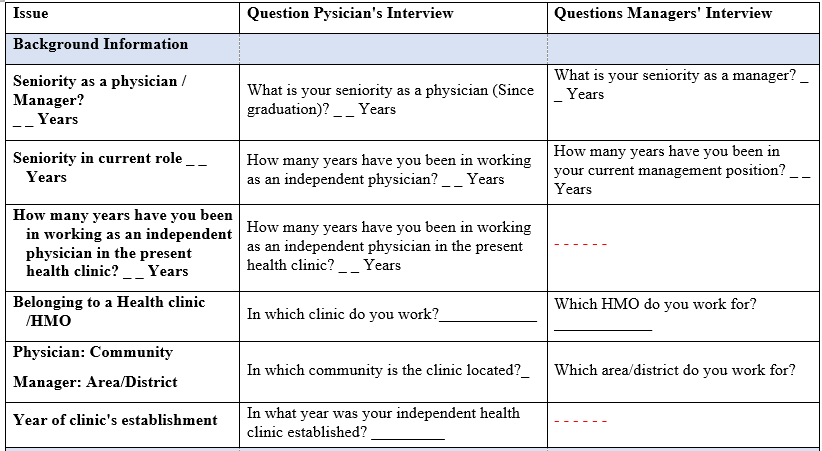
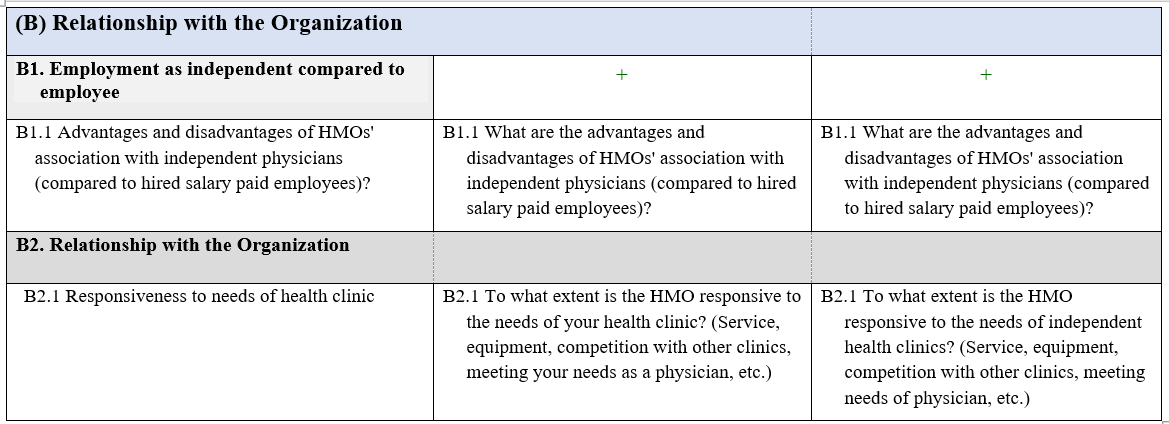
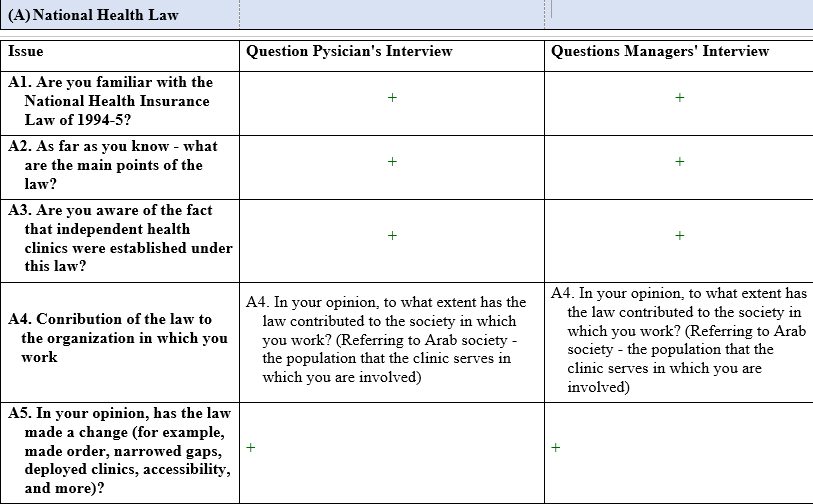
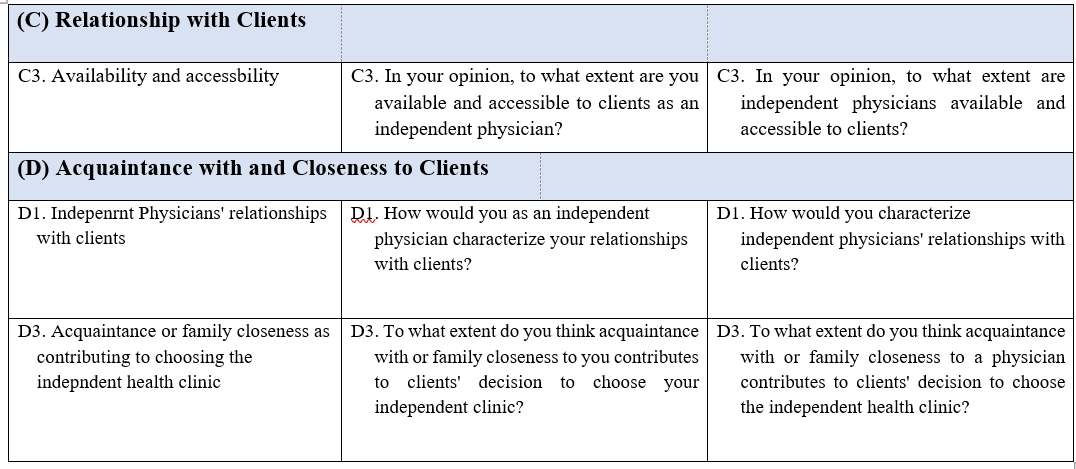
The guides were similar in most of the categories. The categories included background data, questions that are related to state national health law, work relationship with the organization, relationship with Clients and Acquaintance with and Closeness to Clients.
National health law- answers the first research aim and question
Work relationship with the organization in the manner of advantages and disadvantages of the method and the area of remuneration as a motivational contributor to willingness to work and the relationship itself with organization in the manner of attentiveness and satisfaction - answers the sequined research aim and question.
Relationship with Clients and Acquaintance with and Closeness to them- answers the third research aim and question.
The managers and physicians were not randomly selected. They represent two HMOs equally. All belong to the Arab society another interviewee who is not an Arab, a physician and a manager who until recently worked at one of the HMOs and moved to another competitive HMO. She represents the other who doesn’t not belong to the Arab society.
Systematic content analysis of the Interviews (see figure 5)
Qualitative Interview Analysis:
Each interview recorded and transcribed
Reading and separating into “units of meaning”
The findings of the systematic analysis are coded
Themes and patterns were Identify in each unit of meaning, classified into categories
Summary of the themes and categories
Building a "category tree" of the themes
Formulation of items for the quantitative questionnaire
Example for statements suggested for the questionnaire based on the produced themes:
To what extent do you agree with the claim that the system of operating independent clinics should be continued?
Both the physicians and the clients benefit from this system (1)
(2) This system should be maintained in condition that the HMOs supervise the independent clinics
Main findings
The findings obtained in the study were found to confirm the objectives and questions of the study. Most managers and physicians replied that they are familiar with the law (Managers Yes – 5 of 7, generally yes – 2 of 7, Physicians (Yes – 5 of 6, generally yes – 1 of
Physicians and managers recognized that the National Health Insurance Law had an impact on Arab society in the context of developing independent clinics, contributed to reducing health disparities and made the service accessible to Arab. Most of them knew that the law allows "the right of all citizens to receive treatment"" , the "Treatment is equal for everyone, the law allows medical service to be provided to the entire population regardless of socioeconomic status, allows equality between the HMOs and all residents, It is built on the principle of social solidarity, regardless of whether the citizen Works or doesn't work",and "a person pays a health tax to the State of Israel and the state provides him with free health services according to the health basket established by law".They replied that the insured person can choose any HMO he is interested in according to personal choice. In other words, pre-existing conditions and age are irrelevant when applying for basic health insurance in Israel. The basic baskett services offered multiple of treatments such as physician's visits, medications, and hospitalizations included in the National Law. In summary, all the interviewees showed to varying extents how familiar they are with the law. The proficiency in the field of services provided by the law was not similar between the physicians and the manager, the minority of interviewees emphasized the expanding of the services in the health basket with a wide variety and accessibility to services in the Arab population which the law contributed to. On the subject of advantages and disadvantages of the method of contracting the HMO with an independent physician, The interviewees were asked about the relationship with the HMO, the advantages and disadvantages of the method and the contract method of the HMO with an independent physician. The physicians and managers expressed how useful and desirable this method is, it allows flexibility, one independent physician commented on how flexible and accessible it is to clients when the physical clinic is in the client's environment. "As I mentioned, there is flexibility in the opening hours and their activities are closer to homes and residences.". In addition, it is claimed that "the clinics are less busy, so this allows more time for the physician to meet with the patient and do the meeting properly". "Enables a personal approach and a more personal relationship" it brings adequate compensation for the physician, develops interdependence between the patient and the physician, allows for a personal approach and a positive relationship, Physicians note a high sense of belonging of clients to the independent clinic."The client depends on me , because he knows that there is no better than me, who knows his health condition,economic and social status more than me?"Adds a lot to the physician in the area of the manager when the physician is also manager himself. "Independent clinics are usually managed by a physician who is considered by the HMO as a strength, he brought the customers. Managers indicate positive feedback for the most part "generally positive about the Physicians ".A close physician to the patient that lives at the same community makes the relation more close and related.Physicians emphasized that at the beginning of the agreement the HMO is more attentive to them. They (The HMOs) are attentive, they help in a good way, they want to keep their customers, the organization behaves with us, as independents, as if it were a regular clinic, we also claim that a center HMO clinic really meets all their needs. In terms of equipment, in terms of maintenance and in terms of everything. They provide 100% service A minority of managers answered that listening and responding to them is not at the level they demand and that it depends on the HMO they work for.All the physicians satisfied with the communication .The managers expressed satisfaction to a large extent with the way of communication. "In my area I can testify that there is a good connection, I am satisfied because we serve more than one HMO and we were able to create competition with the HMOs and this improved our status, satisfied, it gave me the freedom to practice medicine, 100 percent as I believe it should be, to be the contact with the patients" The physicians and managers expressed how useful and flexible the method is "As I mentioned, there is flexibility in the opening hours and their activities are closer to homes and residences"."I managed the clinic according to my perception, how I saw myself as a family physician in relation to availability, communication, time control, receiving clients, the hours of reception, everything was actually adapted to both my needs and the needs of my patients but of course I made sure there was service, almost every day the clinic was open and there was almost no service". "Enables a personal approach and a more personal relationship".It was found that physicians characterize their relationships as friendly, family, childhood friends. The managers characterize the relationships as close, caring and preserving clients (personal family relationship). Only one manager stated that closeness is not the main factor. contact with clients according to the physicians opinion and according to the managers' opinion exists, in large part it is based on personal and family relationships especially in the village, in the urban area it is based mainly on personal acquaintance, existing friendships and even childhood friendships, in part it is not based at all on any friendship or family relationship, based on Just knowing that this physicians exists and is in the same neighborhood or city. These connections and closness affect positively the preservation of the clinics and there growth."The managers expressed great satisfaction with the way the contract was made. "In terms of earning and contact with the HMO in a direct connection, I see an advantage" An HMO can reward without the limit of the Ministry of Finance control " The monetary reward is considered major, received high grades on all rewards, the material reward leading a direct connection with the HMO. The interviewees pointed out many disadvantages there is no commitment towards the physician, a lack of commitment and loyalty that usually comes from the physician's side," the physician is always open to offers from competitors and tends to leave if he receives offers with better conditions from another HMO". Managers also think that the material reward is the most important rewards, but they believe that the reason for the physicians transfering from the HMO to another is financial. The cause is over of stimulation and pressures exerted by the competing HMOs on the physician to leave its HMO. In the area of control and supervision" the physicians do not work under the organization in an orderly manner"," we as an HMO and managers can enforce them less", "The supervision is more on the HMO clinics". A female physician expressed the level of the independent physician's relationship with the system: "If you are only independent, you disconnect from the system. To feel a bit of a sense of not belonging and a sense of a certain disconnection, not so close to the sources of knowledge. Four out of six physicians versus six out of seven managers answered that customer engagement and performance improvement is the correct method as a preferred motivational reward. Motivational factors are not included in the structure of the personal contract, for example, improvement in medical quality indices, improvement in satisfaction surveys, management of a normal health economy, cost savings and unnecessary costs (hospitalizations, medications, providers, etc.). Social rewards and moral rewards are also not always part of the contract of engagement and if so, are not emphasized. It is found in research that they should be considered from the beginning and when signing the contract physicians have recommended promoting a physical and technological environment as more important than most managers. Physicians note that poor working conditions and an unsupportive environment greatly affect their work and their motivation to cope and work. Motivational factors that are related to the Physicians professionalism, conduct, availability and how close he is to the client 'affect his conduct and existence. Physicians support the recruitment of administrative and professional personnel.Managers prefer to be employees and not work as self-employed. Building an association for independent physicians, has emerged as a general issue and regardless of a specific HMO, accompanied by the promotion and development of business. The Physicians suggested promoting the pooling of resources with the rest of the HMOs in peripheral and small places to increase their income. The physicians who recommended pooling resources mentioned that the financial side is an advantage, working with several HMOs at the same time "I prefer to work with four in order to bring in even more money, it's a huge saving. In the small places far from the center this is very significant. In the small settlements there is more than one primary clinic".On a professional value level, the pooling of resources is of great importance, as one of the physicians said: the ideology says that the physician should work with any HMO or any other organization, I mean the independent physician in order to serve the patient and not serve the organization. Some physicians pointed out that the method is not convenient, "I get everything from the same HMO anyway, the method will be burdensome and preferably not". The difference between managers and physicians is that the physicians do not see the method as harming the quality of care compared to the managers, yes, the managers see the danger in starting to switch customers from one HMO to another and a danger to that central HMO. Something that can be prevented if there is a restriction on transferring of clients in these clinics in advance.Another physician suggests a change in the method and way of contracting, "Collective work. I think there is a need for a change, not only in the method, even in the way of contracting with the independent physician. I think today medicine as independent physicians should be collective medicine, a number of physicians work at the same time in a certain organization as if they were employees but They are independent." Four or five employees in a medical center will work together, independent physicians one helping the other and each getting their own. like group practice". To summarize the method which is recommended by most interviewees and according to which an independent clinic will be rewarded here is the combined method. Connecting economic, social and moral incentives on a uniform standard basis among all physicians and according to their type of specialization is the basis for a theoretical engagement framework that can become practical when implemented in practice. Such a uniform framework can be backed by the ministry, will encourage maximum uniformity in the operation of the method and will promote the preservation of independent physicians in the HMOs, without having to move from one to another. Growth of the clinics should continue to be encouraged while taking advantage of the family connection between the clients and the physician while emphasizing the observance of the rules and procedures when providing and approving treatments. It was discovered that most physicians agree that the method of operating independent clinics should be continued compared to only 50% of managers who prefer not to continue with the method.
Discussion
The article presented the qualitative stage in the research. All interviewees cooperated and were familiar with the subject. The results in the qualitative research helped to understand the phenomenon through data collection by interview guides. The guides were built specifically for physicians and managers of the independent clinics and usual HMOs clinics. The data collection tool, which is a preliminary developer of its kind, was found to be reliable and valid in the hope that more researchers will be used in the future, to continue examine the phenomenon in Arab society and / or concentrate of a main issue from the guide. All the interviews were transcribed by an expert in the matter. With the assistance of those tools a questioner created, specifically for the quantitative survey. Both groups, the managers, and the physicians, expressed their opinion that the questions included in the guides were appropriate for the research and represent the topic. It is not possible to compare findings of the study with previous studies, because no studies that examined the impact of the law on Arab society in the context of developing independent clinics were found. The initial findings in the context of the purpose of the first study indicate that most Physicians (67.3%) and managers (84.1%) are acquainted with the law and its principles generally or well. Most of the physicians and managers correctly answered that "Every citizen must be insured in an HMO", "All residents are covered with equal medical care (regardless of socioeconomic, age, gender, and religion, country of origin of citizen c status)"," and Every Israeli citizen is entitled to medical treatment based on equal "health basket". "The patient is entitled to choose the attending physician", Less than a quarter (21.5%) answered that statement. Regarding the contribution of the National Health Law of 1994-5 (National Health Insurance Law, 1994) to society and to the Arab population; on average, they all agree that it has contributed to a high extent. However, the law brought changes especially in the following areas: " Patients can choose a physician based on their preference" All residents have medical insurance in one of the HMOs which provides them with equal entitlement to treatment in accordance with the "medical services coverage", " There are more clinics in the Arab sector and their geographic spread has grown. However, the law has generated the few changes in two areas: "clinics are more crowded than in the past", and "Physicians have less time to devote to each patient". The participants in the study on these stages demonstrated a great deal of knowledge about the law, the young did not know what was before the law, but the veterans with experience answered that the phenomenon is familiar but different compared to the past (way of contacting the physician, layout, availability, service, and competition between all the HMOs).
The second aim was to develop a conceptual framework regarding methods for motivating physicians in addition to the existing financial model, in the context of independent clinics in Arab society. The Research question related to this aim was what the main Components of methods of motivating physicians are in addition to the existing material rewards. The initial, unique findings, in the context of the purpose of this study indicate that both physicians and managers agree that the contractual reward methods are suitable for increasing the physician's motivation and satisfaction of working in an independent clinic. In addition to the existing financial rewards, social and moral rewards should be added and embedded in the primary contract. When the managers were asked about the main reasons why a certain physician left an HMO and moved to another HMO most of the managers, six out of seven answered that the transition between the HMOs for financial purposes and for the improvement of conditions. In the opinion of Physicians, the main reason for leaving is related to the respect given to the Physician. When some do not keep their initial promises, do not meet the guaranteed salary and the terms of the agreement, this is interpreted as a personal insult to the Physicians.
The third aim was to examine the Perceptions of the independent clinics that are established following the NHL– should they continue and perhaps expand? It was also found as a unique finding that most physicians agree that the method of operating independent clinics should be continued with various service factors and providers in the community. Compared to only 50% of managers who prefer not to continue with this method. The combined remuneration quoted - "Customer engagement and performance improvement are the most successful choice in motivating independent physicians to be willing to work. Four physicians out of six versus six managers out of seven answered that this is the correct method as a preferred motivational reward.
In the context of the research findings and the proposed conceptual model four theoretical models were used: (1) Dimensions of national cultures (Hofstede, 2011); (2) Social responsibility (Giddens, 1984); (3) Social capital and human capital (Dakhli & De Clercq, 2004); and (4) Organizational change (Allison et al., 2021). The above theories support the theoretical conceptual model that has been built and proposed for the future as a basis of contract between the independent physician and the HMO.
Conclusions
The research discusses various sociological-cultural aspects based on several sociological theories regarding the national health low in the Arab society in the context of the state health insurance law, systemic aspects in the context of the implementation of the state health insurance law and personal aspects in the context of motivational incentives and rewards for the physician at the level of the independent clinic in the Arab society. The interviewees both as physicians and managers, with many years of experience, are experts and experienced, well acquainted with the subject. Their answers to all the questions were matter of fact and caring, they expressed great satisfaction that the subject is finally coming up on the agenda with an emphasis that it is accompanied by research at the academic level. The acquired research will provide general knowledge to new physicians who were not familiar with the phenomenon of independent clinics.
The method of operating independent clinics must be continued and even expand. Resources must be pooled between the HMOs in peripheral and small places. The study contributed to the understanding of the desired incentive model that is proposed to be adopted among the independent physicians. The proposed system of communication between the HMOs and physicians in independent clinics should be preserved and strengthen the social, environmental, moral incentive and anchor them in the contract in the first place. The physician as a person who treats and invests in his patients and clinic, the financial incentive is very important to him at the beginning and throughout the engagement, the physician emphasized that all the time. The study proposed to create an independent work model based on personal remuneration according to expertise, status and personal influence of the physician in society, providing moral rewards and personal marketing of the physician between all clinics and at the locality. The qualitative research recommended to build a union, under their association within the Medical Association to advice and backup those physicians. The study had many limitations in that it was conducted during the corona period, it was very difficult to locate physicians and managers from different HMOs who were willing to be interviewed. The interviews from the HMOs were very cautious to answer directly and to give a competitive and confidential information. Ensuring the confidentiality of information while preserving the sources of information and that no one would be harmed was of great importance in the cooperation and openness of the interviewees. Another limitation of the research during the corona period were to meet face to face the interviews. Usually at the qualitative study the questions are open and the conversation to collect information is not limited and designed. This limit brought to build an interview Gide to the physician and the manager to ask equally the interviews from two competitive HMOs almost the same question. A question that can be used at quantitative research. The tools were found to be helpful and important for future research. The interviews were conducted only for participants of two HMOs, the researcher knew from advance that these participants will cooperate and will be open to answer even though there is a competition between the HMOs and others will not cooperate because they are really competitive, and the researcher don’t know them personally to be sure that they will cooperate.
The two-stage study was carried out in the North District among physicians and managers equally from Two HMOs. The first study was not carried out in all HMOs and in all the districts throughout the country. It was not carried out among all populations and religions and no comparison was made with other groups in society. The research proposal to examine the existence of the phenomenon throughout the country in the various societies while comparing between Arabs and Jewish society and comparing a village to a city. Another suggestion is to examine the quality of medicine and level of services applied at independent clinic compared to usual HMO. The study conducted in the North District, out of convenience and from the fact that the researcher started from the assumption that most of the Christian, Muslim and Druze population are mainly in the north. It is recommended to examine the phenomenon in the Arab society in the center, south of Israel and east of Jerusalem. The research can promote other research at the world where there are privet or "office" clinics. This is a pioneering article; the two studies of this research will be published in the future in one combined article.
Acknowledgments
Thanks to my conductor professor Stefan Cojocaru and all participants (Physicians and Managers from all levels and HMOs)
References
Allison, J., Cook, J., & Grimsley, S. (2021). Organizational Culture Change: Examples, Theory& Strategies. https://study.com/learn/lesson/organizational-change-examples-theory-strategies.html
Bin Nun, G., Berlovitz, Y., & Shani, M. (2020). The health system in Israel. The Ministry of defense Publishing House.
Brassey, J., Elwyn, G., Price, C., & Kinnersley, P. (2001). Just in time information for clinicians: a questionnaire evaluation of the ATTRACT project. British medical journal, 322(7285), 529-530.
Chaix-Couturier, C., Durand-Zaleski, I., Jolly, D., & Durieux, P. (2000). Effects of financial incentives on medical practice: results from a systematic review of the literature and methodological issues. International Journal for Quality in Health Care, 12(2), 133-142. DOI:
Dakhli, M., & De Clercq, D. (2004). Human capital, social capital, and innovation: a multi-country study. Entrepreneurship & regional development, 16(2), 107-128. DOI:
Giddens, A. (1984). The constitution of society: Outline of the theory of structuration. Univ of California Press.
Hofstede, G. (2011). Dimensionalizing cultures: The Hofstede model in context. Online readings in psychology and culture, 2(1), 2307-0919. DOI:
Horev, T., & Keidar, N. (2010). Light and Shadow on the development of the National Health insurance law. The ministry Health Office, Department of Economics and Health Insurance.
National Health Insurance Law. (1994). Ministry of Health Israel.
Ostbye, T., Yarnall, K. S., Krause, K. M., Pollak, K. I., Gradison, M., & Michener, J. L. (2005). Is there time for management of patients with chronic diseases in primary care? The Annals of Family Medicine, 3(3), 209-214.
Patton, M. Q. (1998). Qualitative research & evaluation methods: Integrating theory and practice. SAGE publications.
Vardi, D., Kyam, R., & Kitai, E. (2008). How we compensate physicians. Hareffua 147(12), 999-1003.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
31 May 2023
Article Doi
eBook ISBN
978-1-80296-962-7
Publisher
European Publisher
Volume
6
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-710
Subjects
Education, reflection, development
Cite this article as:
Sheabar, M., & Cojocaru, S. (2023). Explore Closely but Remote During the Corna Period. In I. Albulescu, & C. Stan (Eds.), Education, Reflection, Development - ERD 2022, vol 6. European Proceedings of Educational Sciences (pp. 420-434). European Publisher. https://doi.org/10.15405/epes.23056.38