
Use Of Mobile Apps In Increasing Adolescents′ Compliance With Physical Rehabilitation Programs


Abstract
In a world that relies more on mobile apps, especially with the emergence of COVID-19, which accelerates this process, we considered using mobile apps in special education, especially medical rehabilitation and physiotherapy in adolescents. The research aimed to check if adolescent compliance may increase and if they became more interested in the rehabilitation process because, in most cases, adolescent rehabilitation is the long run. The research consisted of mobile apps Google Sheets and WhatsApp for 19 days. Adolescents were separated into experimental (6 participants) and control groups (6 participants). They had been performance athletes, leisure athletes, and sedentary. They had to complete in Google Sheets every day after they were doing their exercises. The experimental group received a message from the physiotherapist they were working with through WhatsApp every day to remind them about the exercises. At the end of the research, we found out that the adolescents that are receiving text messages are more likely to do their exercises at home than the adolescent that do not receive text messages. Because the research aimed to see if the compliance with the treatment is increasing by using mobile apps, we can confirm that mobile apps can increase adolescent compliance. Our research considers that using mobile apps can increase compliance with the treatment, and it might bring long-term benefits to the rehabilitation process.
Keywords: Adolescent, compliance, physiotherapy, special education, treatment
Introduction
There is a wide range of specific exercises and reports on their effectiveness, but monitoring the execution of the exercises still creates difficulties (Anwer et al., 2015; Negrini et al., 2008; Negrini et al., 2009). There are also studies that show how important the physiotherapist's supervision is in how the exercises are performed (Kuru et al., 2016; Schreiber et al., 2015), but this is not so easy to achieve in the context where patients have to perform the exercises every day at home, without supervision by the physiotherapist. Recommended home exercise is a tool used by many medical recovery professionals to achieve more satisfactory results (Hayden et al., 2005; Vos et al., 2012) although there is low compliance. Both the physical and financial implications are considerable, so we should look for more viable ways to monitor and increase patience compliance. Even before the COVID-19 pandemic began, monitoring patients at home became difficult, but since then a lot of aspect about it have changed. With the advent of COVID-19, the worldwide medical system has shifted away and limited physical contact (Bokolo, 2020), so monitoring home exercise and compliance has become a critical aspect of the recovery program. There is a growing interest in the mobile application industry in how these applications can influence people's behavior, which means that those in the industry could also use this knowledge to increase compliance and monitor patients’ activity (Merolli et al., 2021).
The use of wireless technologies and especially smartphones in healthcare has increased exponentially in the last decade among both patients and healthcare professionals, 90% of them claim that they have a positive effect on the quality of life (Ramey et al., 2019) and implicitly on the quality of medical care. In the US, those who use their mobile phone as a source of internet access are teenagers, 28% in 2021, and the percentage of those who own a smartphone is 85% (Pew Research Center, 2022). This is important because in our research we needed the subjects to own a smartphone and know how to use it. In most cases, teenagers are very attracted to smartphones as a tool (Punukollu & Marques, 2019), and it is becoming more and more indispensable. In her work (Reupert, 2019) “Editorial: the future of mental health promotion is on the Internet”, Andrea Reupert discusses the possible benefits of adolescent mental health in the use of mobile applications, which leads us to think about the possibility of using them in physical recovery of these developing adults (Levinger et al., 2017). With the evolution of the Internet and its increased accessibility among all age groups, we realize that the Internet and mobile apps can be a facilitator in our work.
In the medical system, physiotherapists aim to increase compliance with treatment. Medical recovery is often based on exercises that patients have to perform at home. The exercises are specific for the pathology they suffer from and for the patient's ability to perform them correctly (Argent et al., 2017). Although physical therapy is often indicated, compliance with recovery programs can be a real impediment and a real challenge for the medical system (Alkan et al., 2021). Exercise is an important therapeutic part in recovery and these recommended exercises at home are of great importance in medical recovery (Bachmann et al., 2017). Patient compliance is one of the most important aspects to the success of recovery treatment (Bachmann et al., 2017) and lack of compliance raises major issues, even medically regressive (Palazzo et al., 2016). The World Health Organization defines compliance as "the extent to which a person's behavior - taking medication, following a diet and / or changing his lifestyle, corresponds to the recommendations agreed upon by a healthcare provider" (Sabaté, 2003, p. 136). In his paper (Lenoir et al., 2019) emphasizes that compliance with treatment is imperative to achieve high performance in any therapy.
Problem Statement
In most cases, low patient compliance results in poor recovery (Clark et al., 2019) and low patient compliance is often justified by patients. The success of the treatment depends very much on the compliance of the beneficiary. Compliance with treatment is essential for a favourable outcome in terms of medical recovery (Picha et al., 2019). There is evidence to suggest that non-compliance with recovery treatments is somewhere between 30% - 50% (Bassett, 2012) or other paper suggest 50% - 70% (Essery et al., 2017; Kolt & McEvoy, 2003; Palazzo et al., 2016).
Research Question
In the field of medical recovery, it is known that patient compliance is important and often problematic. Healthcare professionals often look for ways to increase patient compliance with treatment. Given that we need increased compliance for treatment and the predisposition of teenagers to use smartphones, we ask: can mobile applications increase the compliance of children under treatment?
Purpose of the Study
The purpose of this research is to check whether the use of two common and free applications (GoogleSheets and WhatsApp) can influence the compliance of adolescents with their recommended treatment at home.
Research Methods
This research is part quantitative because of the data that we collected in the table and a qualitative because we had to use observation in validating the data from the table. We opted for a combination of quantitative and qualitative because we are working with people, in healthcare and education, and they are different so we have to adapt. As (Busetto et al., 2020) write;
Reasons for combining methods can be diverse, including triangulation for corroboration of findings, complementarity for illustration and clarification of results, expansion to extend the breadth and range of the study, explanation of (unexpected) results generated with one method with the help of another, or offsetting the weakness of one method with the strength of another. (p. 5)
Design of the experiment
Two groups of patients, randomly selected in the order in which they were written in the table. The first half of the table were introduced in the control group, the second half the experimental group.
In order to be eligible, patients had to be diagnosed with a diagnosed musculoskeletal disorder and recommended medical recovery or physical therapy. Patients had to be between 9 and 17 years old.
Circumstances of the experiment
The participants were patients in a private recovery clinic in Zalău, Sălaj, Romania in April 2021, for a period of 19 calendar days.
Patients were instructed on the exercises and how to perform them correctly for at least 10 physical therapy sessions prior to the start of the experiment. The exercises were customized for each patient based on pathology, age, endurance, coordination and goals set by the therapist following discussions with relatives and patients.
Patients have been granted access to a Google Sheets file via either their personal e-mail address or that of their parents. The file contained a table with the following data: the first column "First name and last name" from the second column to the last in the table were the dates of the days when the experiment took place. Next to each name, each day had a box that could be ticked (Figure 1).
Figures
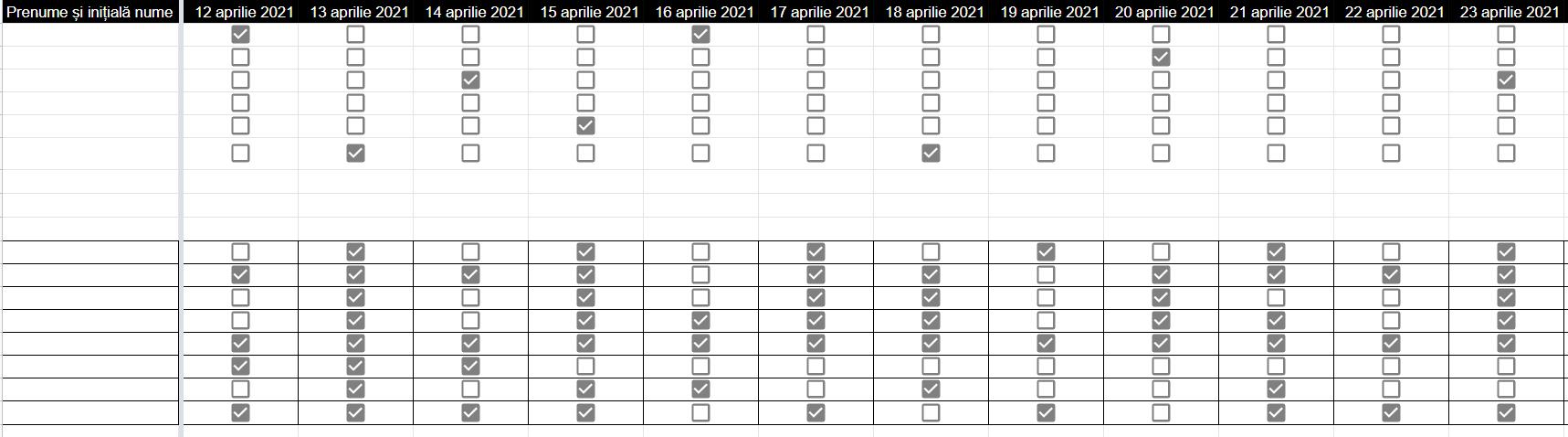
The experimental group, consisting of six patients, received a message every day through the WhatsApp application in which they were reminded that they had to perform their exercises, and then tick the box associated with the day.
The control group of six patients did not receive any messages and were not checked at home.
Patients, both the control group and the experimental group, were instructed to tick the box for that day, including the days when they participated in the scheduled activities inside the clinic, after they were performing their exercises.
Once a week, patients, when they were physically present in the clinic, were asked: "Were the exercises done at home hard?", "How long did it take you to do them?", "Do you want to change something?",” Did you remember what the exercises you had to do?”, to check if the additions in the table are real or fictitious. The questions and answers were not recorded, because their role was only to check if the completion of the table is fictitious or real. Among the participants were patients who practiced competitive and leisure sports as well as people who did not practice sports. Table 1 summarizes the study participants.
Result
Results were measured strictly from the compliance perspective. No other data has been collected expect a free eye analysis of how to perform the exercises in order to find out if the subjects has indeed learned their exercises. No data about exercises performance had been collected.
The study lasted nineteen days, the time devoted to patients recording the data in the table. At the end of the nineteen days, the boxes ticked by the patients were counted. There were no cross-groups between control and experimental group, nor were there any requests to move from one group to another.
After counting the completed boxes, it was found that out of the six patients in the control group: one of them did not complete even once, two of them completed only once, one of them completed twice, one completed four times and one patient ten times. From the experiment group: one patient three times, one patient completed ten times, one patient thirteen times, two patients fourteen times, and one patient nineteen times. These aspects can be followed in Figure 2.

There is a big difference between the patients who were constantly reminded of the physical activities they had the responsibility to perform at home. The average number of days completed in the control group was 2.83 and in the case of the experimental group the average is 9.83. Figure 3 shows the difference.
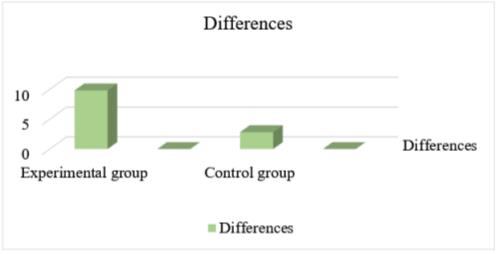
Unfortunately, the research cannot count the results from the point of view of the efficiency of the exercises, but it brings in perspective and demonstrates that by using mobile applications the compliance of children in treatment can increase and therefore the results of treatment will be better.
Discussions
By the fact that the research only aimed to see if the compliance with the treatment increases through the use of mobile applications, we can say that the research has demonstrated this. Despite the fact that we do not have confirmation that the patients performed all the exercises on the days they completed, we can say that they at least thought about the exercises and we assume that in this way they recapitulated what they had to do. It is true that we do not know if there have been any improvements in terms of recovery, but we do know that such an approach can help patients to remember the exercises, at least in terms of how they are performed. Such an approach could have long-term beneficial effects, as we believe that patients simply remember the physical activities they need to do.
At the end of the research, we found out that the adolescents that are receiving text messages are more likely to do their exercises at home than the adolescent that do not receive text messages. Because the research aimed to see if the compliance with the treatment is increasing by using mobile apps, we can confirm that mobile apps can increase adolescent compliance. Our research considers that using mobile apps can increase compliance with the treatment, and it might bring long-term benefits to the rehabilitation process.
Conclusion
Our research suggests that the use of mobile applications may increase treatment compliance and may have long-term beneficial effects on the medical recovery process. Further studies are needed on this issue, but the results so far are favourable.
References
Alkan, H., Yardimci, B. N., Porsnok, D., Sırtbas, G., Livanelioğlu, A., & Mutlu, A. (2021). An investigation of compliance to a home-based physiotherapy program and emotional intelligence of mothers of infants at risk. International Journal of Health Administration and Education Congress (Sanitas Magisterium), 1-10.
Anwer, S., Alghadir, A., Abu Shaphe, M., & Anwar, D. (2015). Effects of Exercise on Spinal Deformities and Quality of Life in Patients with Adolescent Idiopathic Scoliosis. BioMed Research International, 2015, 1-15. DOI:
Argent, R., Daly, A., & Caulfield, B. (2017). Patient Involvement With Home-Based Exercise Programs: Can Connected Health Interventions Influence Adherence? Physical Therapy in Sport, 29-37.
Bachmann, C., Oesch, P., & Bachmann, S. (2017). Recommendations for improving adherence to home-based exercise: a systematic review. Physikalische Medizin, Rehabilitationsmedizin, Kurortmedizin, 20-31.
Bassett, S. (2012). Measuring Patient Adherence to Physiotherapy. Journal of Novel Physiotherapies, 02(07). DOI:
Bokolo, A. Jnr. (2020). Use of Telemedicine and Virtual Care for Remote Treatment in Response to COVID-19 Pandemic. Journal of Medical Systems, 44(7). DOI:
Busetto, L., Wick, W., & Gumbinger, C. (2020). How to use and assess qualitative research methods. Neurological Research and Practice, 2(1). DOI:
Clark, H., Bassett, S., & Siegert, R. (2019). The effectiveness of web-based patient education and action and coping plans as an adjunct to patient treatment in physiotherapy: A randomized controlled trial. Physiotherapy Theory and Practice, 35(10), 930-939.
Essery, R., Geraghty, A. W. A., Kirby, S., & Yardley, L. (2017). Predictors of adherence to home-based physical therapies: a systematic review. Disability and Rehabilitation, 39(6), 519-534. DOI:
Hayden, J. A., van Tulder, M. W., & Tomlinson, G. (2005). Systematic Review: Strategies for Using Exercise Therapy To Improve Outcomes in Chronic Low Back Pain. Annals of Internal Medicine, 142(9), 776-785. DOI:
Kolt, G. S., & McEvoy, J. F. (2003). Adherence to rehabilitation in patients with low back pain. Manual Therapy, 8(2), 110-116. DOI:
Kuru, T., Yeldan, İ., Dereli, E. E., Özdinçler, A. R., Dikici, F., & Çolak, İ. (2016). The efficacy of three-dimensional Schroth exercises in adolescent idiopathic scoliosis: a randomised controlled clinical trial. Clinical Rehabilitation, 30(2), 181-190. DOI:
Lenoir, D., Coppieters, I., Willaert, W., Kregel, J., Danneels, L., Cagnie, B., Meeus, M., Nijs, J., & Malfliet, A. (2019). Do sociodemographic features, pain sensitivity or pain catastrophizing relate to clinic-based adherence to physiotherapy in people suffering from chronic spinal pain? Secondary analysis of a randomized clinical trial. Musculoskeletal Science and Practice, 44, 102066. DOI:
Levinger, P., Hallam, K., Fraser, D., Pile, R., Ardern, C., Moreira, B., & Talbot, S. (2017). A novel web-support intervention to promote recovery following Anterior Cruciate Ligament reconstruction: A pilot randomised controlled trial. Physical Therapy in Sport, 27, 29-37. DOI:
Merolli, M., Francis, J. J., Vallance, P., Bennell, K. L., Malliaras, P., & Hinman, R. S. (2021). Patient-Facing Mobile Apps to Support Physiotherapy Care: Protocol for a Systematic Review of Apps Within App Stores. JMIR Research Protocols, 10(12), e29047. DOI: 10.2196/29047
Negrini, S., Atanasio, S., Fusco, C., & Zaina, F. (2009). Effectiveness of complete conservative treatment for adolescent idiopathic scoliosis (bracing and exercises) based on SOSORT management criteria: results according to the SRS criteria for bracing studies - SOSORT Award 2009 Winner. Scoliosis, 4(1). DOI:
Negrini, S., Fusco, C., Minozzi, S., Atanasio, S., Zaina, F., & Romano, M. (2008). Exercises reduce the progression rate of adolescent idiopathic scoliosis: Results of a comprehensive systematic review of the literature. Disability and Rehabilitation, 30(10), 772-785. DOI:
Palazzo, C., Klinger, E., Dorner, V., Kadri, A., Thierry, O., Boumenir, Y., Martin, W., Poiraudeau, S., & Ville, I. (2016). Barriers to home-based exercise program adherence with chronic low back pain: Patient expectations regarding new technologies. Annals of Physical and Rehabilitation Medicine, 59(2), 107-113. DOI:
Pew Research Center. (2022, June 13). Mobile fact sheet. Pew Research Center. https://www.pewresearch.org/internet/fact-sheet/mobile/
Picha, K. J., Lester, M., Heebner, N. R., Abt, J. P., Usher, E. L., Capilouto, G., & Uhl, T. L. (2019). The Self-Efficacy for Home Exercise Programs Scale: Development and Psychometric Properties. Journal of Orthopaedic & Sports Physical Therapy, 49(9), 647-655. DOI: 10.2519/jospt.2019.8779
Punukollu, M., & Marques, M. (2019). Use of mobile apps and technologies in child and adolescent mental health: a systematic review. Evidence Based Mental Health, 22(4), 161-166. DOI:
Ramey, L., Osborne, C., Kasitinon, D., & Juengst, S. (2019). Apps and Mobile Health Technology in Rehabilitation. Physical Medicine and Rehabilitation Clinics of North America, 30(2), 485-497. DOI:
Reupert, A. (2019). Editorial: the future of mental health promotion is on the Internet. Advances in Mental Health, 17(2), 97-97. DOI:
Sabaté, E. (2003). Adherence to long-term therapies: evidence for action. World Health Organization.
Schreiber, S., Parent, E. C., Moez, E. K., Hedden, D. M., Hill, D., Moreau, M. J., Hill, D., Lou, E., Watkins, E. M., & Southon, S. C. (2015). The effect of Schroth exercises added to the standard of care on the quality of life and muscle endurance in adolescents with idiopathic scoliosis-an assessor and statistician blinded randomized controlled trial: “SOSORT 2015 Award Winner”. Scoliosis, 10(1). DOI:
Vos, T., Flaxman, A. D., Naghavi, M., Lozano, R., Michaud, C., Ezzati, M., Shibuya, K., Salomon, J. A., Abdalla, S., Aboyans, V., Abraham, J., Ackerman, I., Aggarwal, R., Ahn, S. Y., Ali, M. K., Alvarado, M., Anderson, H. R., Anderson, L. M., Andrews, K. G., Atkinson, C., … Memish, Z. A. (2012). Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet (London, England), 380(9859), 2163–2196. DOI:
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
31 May 2023
Article Doi
eBook ISBN
978-1-80296-962-7
Publisher
European Publisher
Volume
6
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-710
Subjects
Education, reflection, development
Cite this article as:
Vereș, B. –. A., Șandor, I., Isidori, E., & Claudia, M. (2023). Use Of Mobile Apps In Increasing Adolescents′ Compliance With Physical Rehabilitation Programs. In I. Albulescu, & C. Stan (Eds.), Education, Reflection, Development - ERD 2022, vol 6. European Proceedings of Educational Sciences (pp. 322-329). European Publisher. https://doi.org/10.15405/epes.23056.29